
Remember me

CVCs are often utilized for intraoperative esophageal cancer management or postoperative nutrition. They are typically inserted preoperatively, and the location of the CVC tip is confirmed using X-rays. The migration rate of the central venous catheters into the azygos vein arch is reported to be approximately 1.2% and is more common when inserted from the left side compared with the right side (Fig. 4) [3]. And the incidence of migration into the azygos vein arch when inserted via the right subclavian vein, as in our case, is reported to be 0.3%. This migration can lead to complications including venipuncture. Prabaharan et al. reported a case where a CVC inserted from the right subclavian vein into the left subclavian vein SVC migrated to the SVC after extubation [4]. Talari et al. reported repeat migration of a peripherally inserted central catheter (PICC) tip into the azygos vein arch [5]. Forauer et al. observed that hand abduction or adduction causes the PICC tip to move an average of 21 mm and a maximum of 53 mm [1]. External conditions can influence the position of the CVC tip, implying that it may not consistently remain in the same position. And Zhang has pointed out that soft silicone PICCs are prone to tip migration [6].
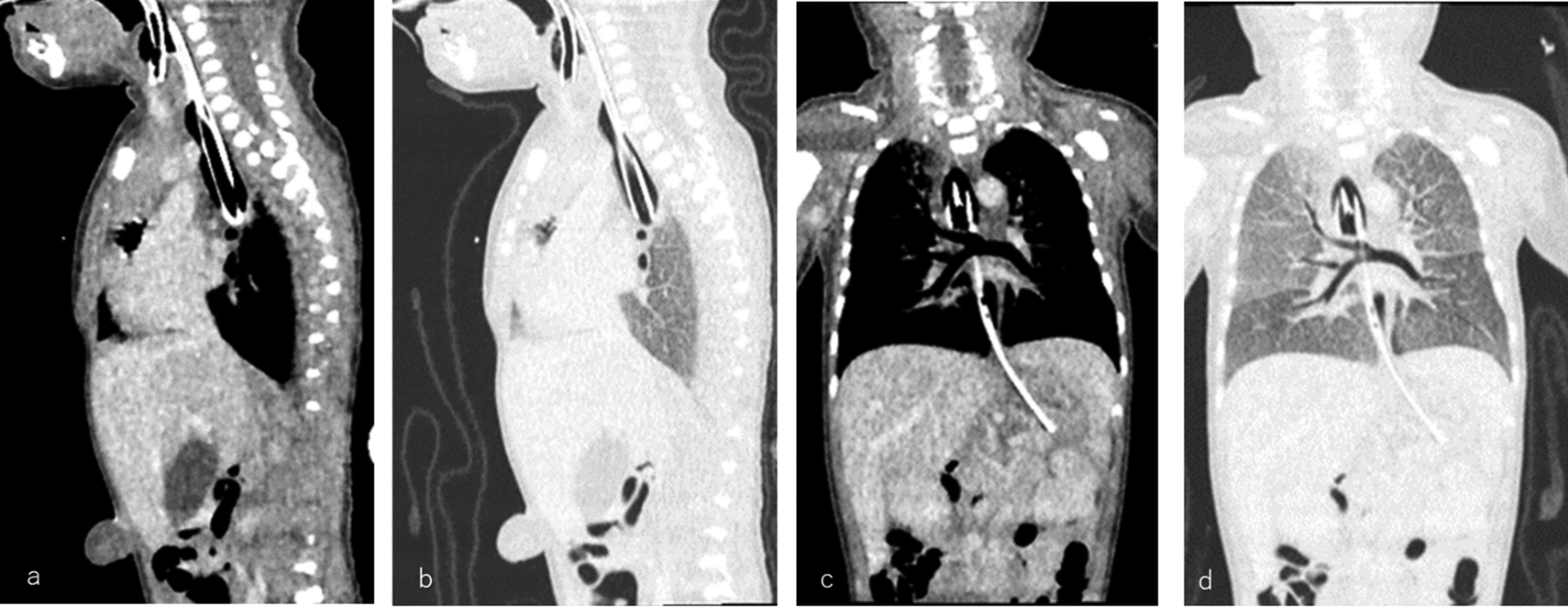
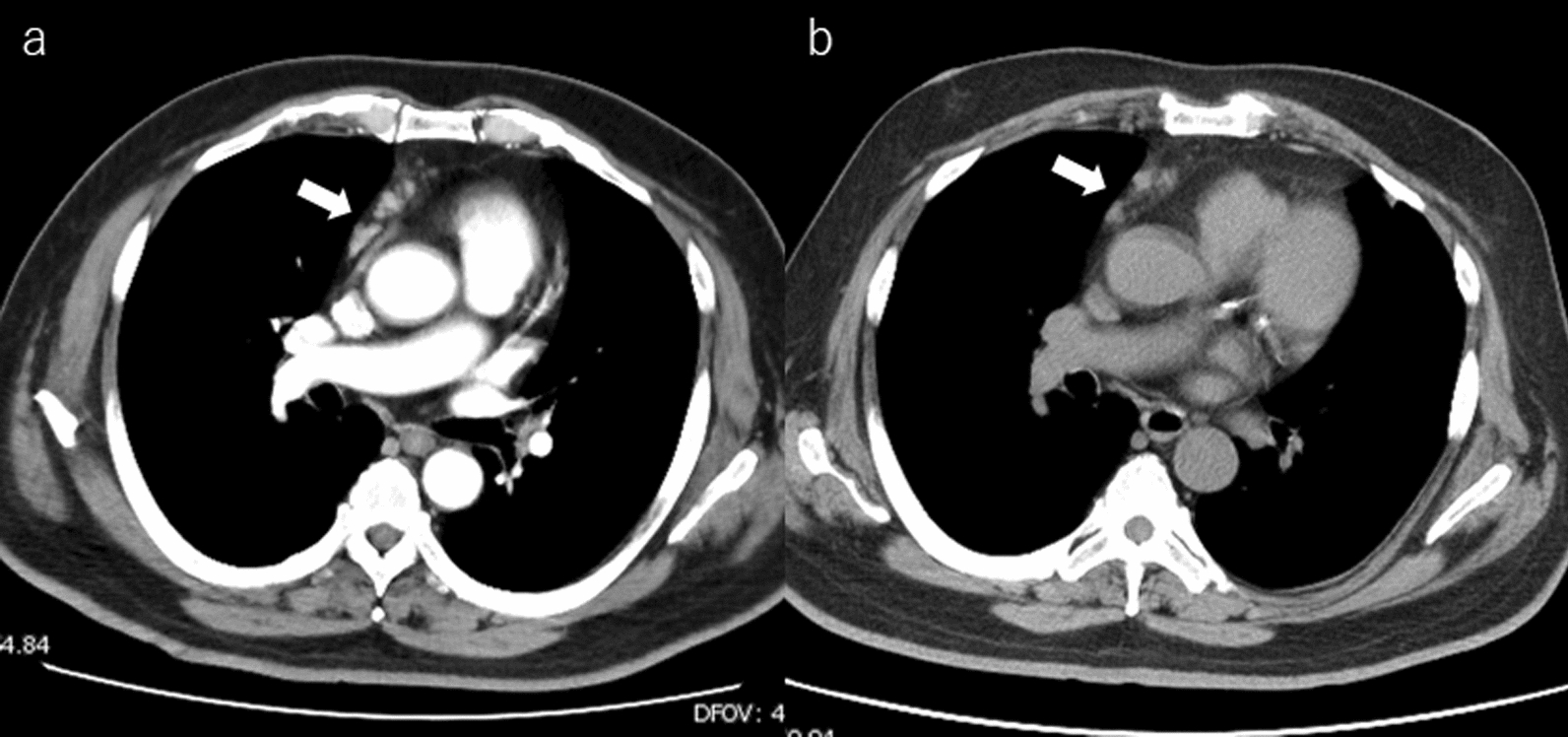
Fig. 4
Bankier et al. demonstrated absolute numbers and frequencies of the catheter malpositions in the azygos arch. a Right subclavian vein. b Right jugular vein. c Left jugular vein. d Left subclavian vein
Currently, esophageal cancer surgery is often performed in the left lateral recumbent or prone position, and the right upper extremity is often abducted and elevated [7]. Conversely, CVC insertion occurs in the supine position and confirmed by chest X-ray. This necessitates recognition that the CVC tip position may change during esophageal cancer surgery performed in the left lateral recumbent or prone positions.
During esophageal cancer surgery, the azygos vein arch is often transected to facilitate the approach to the left recurrent nerve lymph nodes. In the present case, identification of the CVC tip in the azygos vein arch prevented catheter amputation by safely removing it. Reportedly, a case exists where the CVC tip, having migrated into the azygos vein arch, required amputation [6]. Amputating a CVC can pose greater harm to the patient, potentially leading to the conversion of thoracoscopic surgery to an open thoracotomy or necessitating revision surgery, depending on the timing of the diagnosis.
Recognizing intraoperatively a CVC tip that has migrated into the azygos vein arch is challenging. Surgical options to prevent CVC dissection include preservation of the azygos vein arch through right thoracic and cervical mediastinoscopy approaches without dissection of the azygos vein arch, both of which are challenging [8, 9]. Although confirming the tip position using radiograph after CVC placement is essential, many factors can influence the position of the CVC tip during esophageal cancer surgery, such as positional changes, intraoperative changes in intrathoracic pressure, and intraoperative manipulations. To prevent cutting the catheter within the azygos arch, it is important to avoid insertion from the left side, where the catheter is more likely to enter the azygos vein arch. Most importantly, the azygos vein arch should be thoroughly examined to ensure the absence of a CVC before dissecting the azygos vein arch.
Comments (0)