
Remember me

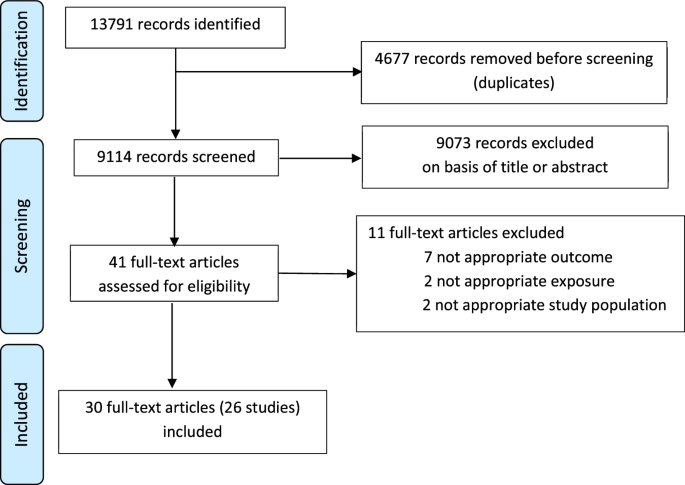
Plasma was collected from 34 patients with NSCLC (41 samples) (Supplementary Table 1) and 12 healthy participants (Supplementary Table 2) and nAb titers against WT and Omicron variants BA.5, BQ1.1, XBB1.5, XBB1.16, and XBB1.9 were assessed (Supplementary Fig. 1 and Supplementary Table 3). Patients in the monovalent cohort (n = 11) had received 2 prior vaccine doses with an average time of 6–8 months since the last dose. Healthy participants and patients with NSCLC in the bivalent cohort had received 3 prior monovalent vaccine doses, with an average time of 10–12 months since the last vaccination (Supplementary Table 1).
After 40 days of the booster, all patients in the monovalent cohort had detectable nAb titers against the WT virus, however, the nAb response to all Omicron variants was significantly reduced (P < 0.0001). Only 18% and 9% of the patients in this cohort generated detectable nAb titers to the XBB1.16 and XBB1.9 variants respectively (Fig. 1a). Importantly, the nAb response increased significantly after the bivalent booster in patients with NSCLC (Supplementary Fig. 2). All patients in the bivalent cohort generated nAbs to the WT and BA.5 variant. More than 80% of the patients had nAb titers to the BQ.1.1 and XBB.1.5 variants while more than 65% of the patients had detectable nAb to the XBB.1.16 and XBB.1.9 variants. However, the nAb titers to BQ.1.1, XBB.1.5, XBB.1.16, and XBB.1.9 were significantly reduced compared to the WT virus (P < 0.0001) (Fig. 1b). Next, we evaluated the nAb response in the plasma of healthy participants after bivalent booster. All healthy participants had detectable nAb to the WT and BA.5 viruses, while 92% of the cohort made nAb to BQ.1.1 and XBB.1.5, 83% had nAb titers to XBB.1.16 and XBB.1.9 variants. Similar to the patients with NSCLC in the bivalent cohort, the neutralizing activity against currently circulating XBB variants was significantly reduced compared to the WT virus in the healthy cohort (P < 0.0001) (Fig. 1c). Interestingly, compared to the healthy participants there was no significant difference in the nAb titers to any virus in patients with NSCLC after the bivalent booster (Supplementary Fig. 3).
Fig. 1: Neutralizing responses against the WA1/2020 strain and Omicron subvariants after monovalent and bivalent booster in patients with NSCLC and in healthy participants.
Neutralization activity against the WA1/2020 strain of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and the Omicron subvariants BA.5, BQ1.1, XBB1.5, XBB1.16, and XBB1.9 in 11 patients with NSCLC after monovalent booster (a) 15 patients with NSCLC (b) and in 12 healthy participants (c) within 40 days of receiving the bivalent booster. Top of each panel shows the focus reduction neutralization test (FRNT50 [the reciprocal dilution of serum that neutralizes 50% of the input virus]) geometric mean titer (GMT) of neutralizing antibodies against the WA1/2020 strain and each Omicron subvariant, along with the ratio of the neutralization GMT against the WA1/2020 strain to that against each Omicron subvariant and the percentage of participants with detectable neutralizing antibody titers. The connecting lines between the variants represent matched serum samples. The horizontal dotted lines represent the limit of detection of the assay (FRNT50 GMT 20). The colored bars represent the FRNT50 GMT among the participants in the cohort. Figures show the percentage of detectable neutralizing titers, mean, and SEM.
Next, we evaluated the durability of nAb response after bivalent booster in healthy participants and patients with NSCLC. Totally, 4–6 months after the bivalent booster vaccination, we observed a reduction in the nAb titers to the WT and the Omicron variants in the healthy participants. While all healthy participants had nAbs against the WT virus, more than 90% and 80% of participants had nAbs against BA.5 and BQ1.1 respectively. More than 55% of the participant had nAbs against the XBB1.5 variant and 42% of the cohort had detectable nAbs against XBB1.16 and XBB1.9 variants (Fig. 2a). Interestingly, the nAb titers in the healthy cohort was significantly reduced after 4–6 months after booster compared to the titers observed within 40 days of booster (WT P < 0.0029, BA.5 P < 0.0145, BQ.1.1 P < 0.1428, XBB.1.5 P < 0.0490, XBB.1.16 P < 0.0416 and XBB.1.9 P < 0.0530) (Supplementary Fig. 4).
Fig. 2: Durability of nAb titers in healthy participants and in patients with NSCLC 4–6 months after bivalent booster.
nAb titers to the WA1/2020 strain and the Omicron subvariants BA.5, BQ1.1, XBB1.5, XBB1.16, and XBB1.9 in 12 healthy participants (a) and 15 patients with NSCLC (b) at 4–6 months after receiving the bivalent booster. Top of each panel shows the focus reduction neutralization test (FRNT50 [the reciprocal dilution of serum that neutralizes 50% of the input virus]) geometric mean titer (GMT) of neutralizing antibodies against the WA1/2020 strain and each Omicron subvariant, along with the ratio of the neutralization GMT against the WA1/2020 strain to that against each Omicron subvariant and the percentage of participants with detectable neutralizing antibody titers. The connecting lines between the variants represent matched serum samples. The horizontal dotted lines represent the limit of detection of the assay (FRNT50 GMT 20). The colored bars represent the FRNT50 GMT among the participants in the cohort. Figures show the percentage of detectable neutralizing titers, mean, and SEM.
Interestingly the decrease in the durability of nAb response after the bivalent booster was more significant in the NSCLC cohort compared to the healthy cohort. Though there was no difference in the nAb titers in the NSCLC cohort compared to the healthy cohort within 40 days after the bivalent booster, the nAb titers to the BQ1.1 (P < 0.0123), XBB1.16 (P < 0.0095) and XBB1.9 (P < 0.0267) were significantly reduced in the NSCLC bivalent booster cohort compared to the healthy cohort 4–6 months post booster vaccination (Supplementary Fig. 5). In the NSCLC patient cohort, we observed a significant reduction in the nAb titers to the Omicron variants compared to the WT strain (P < 0.0001) 4–6 months after the bivalent booster. Though all patients had detectable nAb against the WT strain, only 27% and 13% of the cohort had detectable nAb titers to XBB.1.5 and XBB.1.16 variants, respectively. None of the patients in the NSCLC cohort had detectable nAb titers to the XBB1.9 variants (Fig. 2b). The durability of nAb response was also significantly lower in the NSCLC patients at 4–6 months compared to 40 days of the bivalent booster (WT P < 0.0164, BA.5 P < 0.0161, BQ.1.1 P < 0.0024, XBB.1.5 P < 0.0002, XBB.1.16 P < 0.0002 and XBB.1.9 P < 0.0002) (Supplementary Fig. 6).
Next, we examined if cancer treatment modality and patient demographics of our monovalent and bivalent cohorts influenced our findings discussed above. Age, race, gender, cancer stage, and vaccine type were not statistically different between the cohorts (Supplementary Table 1). As some patients were actively receiving cancer therapy, we also determined whether different cancer therapies influenced the antibody response to vaccination. Patients in our cohorts were divided into different subsets based on their cancer therapy (chemotherapy, immunotherapy, targeted therapy, combination therapy (immunotherapy and chemotherapy), and patients under surveillance. There was no significant bias toward a specific therapy in either of our cohorts which corroborates previous studies5,6 that the type of cancer therapy that the patients received does not influence the nAb response to vaccination (Supplementary Table 1).
Comments (0)