
Remember me
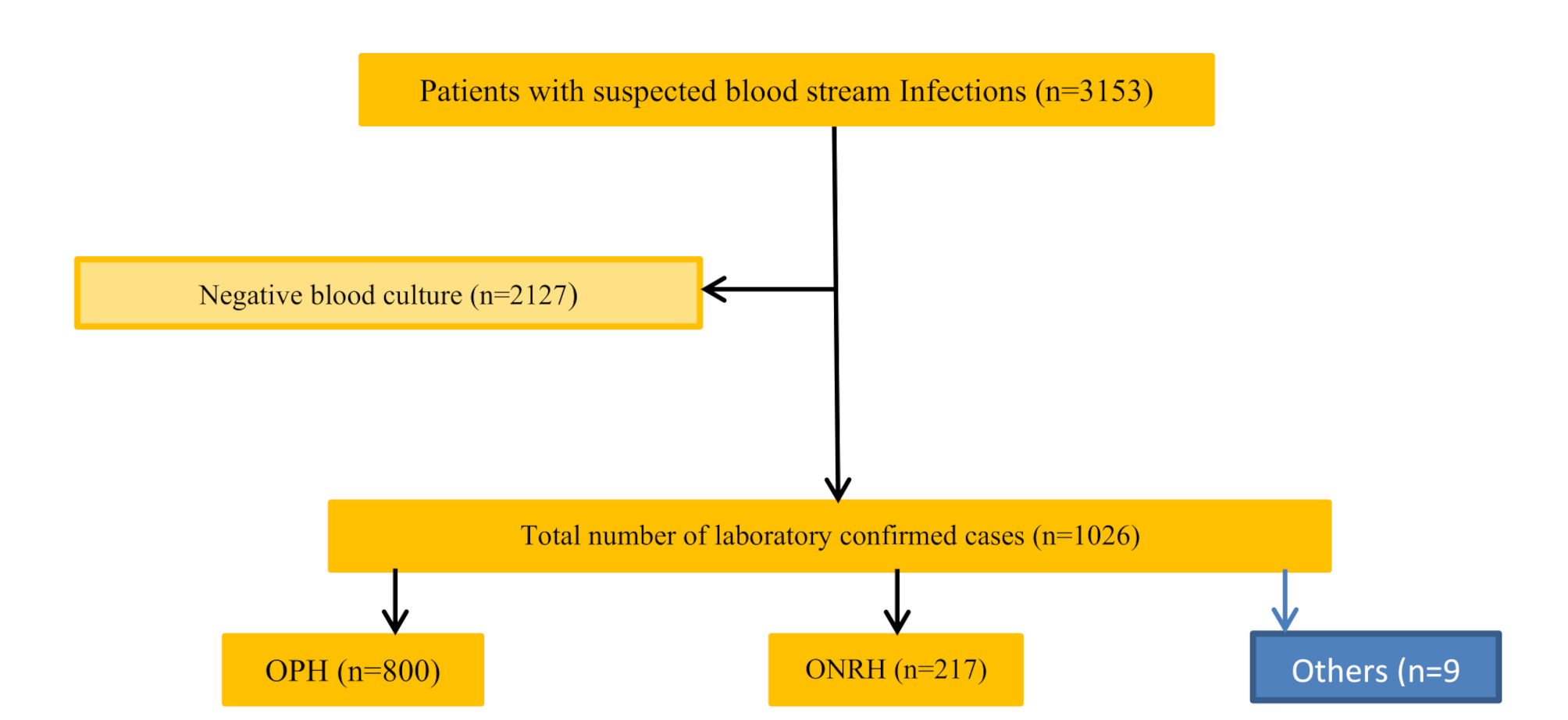




Accumulating evidence has shown that levels of inflammatory biomarkers, including WBC, CRP, NE%, ESR, PCT, IL-6, and IL-10, were significantly higher in patients with bacterial infection than those with non-bacterial infection [15]. However, scant research has addressed the utility of these inflammatory biomarkers in distinguishing between different types of infections, such as bloodstream infections BSI and LBI, as well as classifying pathogenic bacteria into Gram-positive (G+) or Gram-negative (G-) strains. To address this knowledge gap, we conducted a cohort study where patients were segregated into BSI and LBI groups. Within the BSI group, clinical data were collected from a total of 2021 patients. After rigorous screening based on predefined inclusion and exclusion criteria, 542 patients with mono-bacterial infections were enrolled, comprising 331 cases of Gram-negative bacterial infections, 174 cases of Gram-positive bacterial infections, 13 cases of anaerobic bacterial infections, and 24 cases of fungal infections. Due to the limited occurrence of anaerobic and fungal infections in our study, we focused our analysis solely on the 331 cases of Gram-negative and 174 cases of Gram-positive bacterial infections in the BSI group (Fig. 1A). The strain composition isolated from blood cultures is depicted in Table 1, indicating that among Gram-negative infections, Escherichia coli (n = 181, 54.68%) and Klebsiella pneumoniae (n = 67, 20.24%) were the two dominant bacterial species. Among Gram-positive bacteria, the major strains were Staphylococcus aureus (n = 69, 39.66%), Enterococcus spp. (including Enterococcus faecalis and Enterococcus faecium, n = 38, 21.84%), and Streptococcus spp. (n = 34, 19.54%). In the LBI group, clinical data from 1023 patients were meticulously recorded and subjected to thorough screening using predefined inclusion and exclusion criteria (Fig. 1B). Ultimately, 102 patients were included in this study. Notably, there were no significant statistical differences in age, gender, primary diagnosis, or inpatient departments between the BSI and LBI groups. Concerning clinical symptoms, the incidence of fever and chills was higher in the BSI group compared to the LBI group, although there was no statistically significant difference in the incidence of shock between the two groups (Table S1).
Table 1 Microbiological characteristics in patients with BSIValue of diagnostic and predictive capacities of CRP, PCT, IL-6, IL-10, ESR, and NE% in identifying BSIAs shown in Table S2, the BSI group exhibited significantly higher levels of CRP, PCT, IL-6, ESR, WBC, and NE% compared to the LBI group (p < 0.0001). Additionally, the IL-10 levels in the BSI group were higher than those in the LBI group (p = 0.008). Conversely, BSI patients had lower serum levels of PLT compared to LBI patients (p = 0.0254). These findings underscore the crucial roles of these biomarkers in distinguishing between BSI and LBI.
Subsequently, ROC analysis was employed to assess the efficacy of these biomarkers in differentiating BSI from LBI. As depicted in Fig. S1, PCT, CRP, IL-6, IL-10, NE%, and ESR demonstrated excellent diagnostic potential for BSI, while WBC and PLT exhibited relatively weaker diagnostic power. Optimal cut-off value analysis indicated that ESR, PCT, IL-6, and IL-10 exhibited high sensitivity and specificity in diagnosing BSI (Table S3). Remarkably, ESR, previously considered a non-specific biomarker for BSI [23], proved to be a prominent diagnostic indicator in our study, with an AUC of 0.9249, along with high specificity (91.18%) and sensitivity (76.39%). All together these results demonstrate that CRP, PCT, IL-6, IL-10, ESR, and NE% are valuable biomarkers for diagnosing BSI.
PCT, IL-6, and IL-10 are valuable biomarkers to distinguish GP-BSI from GN-BSIBSI pose an immense global burden, with an alarmingly high mortality rate and significant medical expenses. Timely administration of appropriate antibiotic therapies can substantially improve the survival rate and prognosis of BSI patients. However, the inappropriate and irrational use of antibiotics can lead to unfavorable outcomes, such as the emergence of multidrug-resistant organisms. Hence, the accurate identification of potential pathogens is crucial to facilitate early and targeted antibiotic therapies for BSI patients. In this study, we sought to investigate the roles of specific biomarkers, including CRP, PCT, IL-6, IL-10, ESR, WBC, NE%, and PLT, in determining the classifications of BSI pathogens. First of all ,we categorized patients with BSI into two groups based on the Gram staining characteristics of the pathogenic bacteria, namely GP-BSI and GN-BSI. Analysis of demographic characteristics revealed no significant statistical differences in terms of gender, age, primary diagnosis, and inpatient departments (internal medicine, surgery, and ICU) between these two groups (Table 2). Regarding clinical symptoms, the incidence of fever and chills was significantly higher in the GN-BSI group compared to the GP-BSI group, whereas there was no significant difference in the incidence of shock between the two groups (Table 2).
Table 2 Baseline characteristics of patients with BSIAs presented in Table 3, serum levels of PCT, IL-6, IL-10, and CRP were significantly elevated in the GN-BSI group compared to the GP-BSI group, while no significant statistical difference was observed in serum levels of ESR, WBC, NE%, and PLT between these two groups. ROC analysis (Fig. 2; Table 4) demonstrated that PCT, IL-6, and IL-10 (AUC > 0.7) were effective biomarkers for distinguishing GP-BSI from GN-BSI, whereas CRP, ESR, WBC, NE%, and PLT exhibited lower efficiency in diagnosing GP-BSI (AUC < 0.60). Optimal cut-off value analysis revealed that PCT, IL-6, and IL-10 showed high diagnostic power for GP-BSI (p < 0.0001, sensitivity > 74%, specificity > 63%), while CRP had lower diagnostic efficiency (p = 0.0064, sensitivity 55.34%, specificity 62.07%) compared to PCT, IL-6, and IL-10 but displayed higher diagnostic efficacy compared to other biomarkers (WBC, NE%, PLT, and ESR) in diagnosing GP-BSI.
Table 3 Inflammatory biomarker serum levels in patients with GN-BSI and GP-BSIFig. 2
The receiver operating characteristic curves analysis applied to test discriminative performance of inflammatory biomarkers to predict GP-BSI, (A) CRP, PCT, IL-6, and IL-10. (B) WBC, NE%, PLT and ESR
Table 4 Performances of inflammatory biomarkers in GP-BSI identificationFurthermore, we analyzed the diagnostic power of PCT, IL-6, IL-10, and CRP in identifying specific bacterial species. As illustrated in Table S4, in the GN-BSI group, no statistically significant difference was found in the serum levels of PCT, IL-6, IL-10, and CRP among infections caused by Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, Enterobacter cloacae complex, and Proteus mirabilis. Similarly, in the GP-BSI group, no statistically significant difference was observed in serum levels of PCT, IL-6, IL-10, and CRP among infections caused by Staphylococcus aureus, Staphylococcus hominis, Enterococcus faecalis, Enterococcus faecium, and Streptococcus spp (Table S5). Thus, it is evident that PCT, IL-6, and IL-10 play critical roles in diagnosing BSI and identifying pathogen classifications (G+/G-), but have limited ability to differentiate specific bacterial species.
CRP, PCT, and IL-10 possess diagnostic value in the detection of VREMultidrug-resistant organisms (MDROs), including carbapenem-resistant Enterobacteriaceae (CRE), carbapenem-resistant Pseudomonas aeruginosa (CRPA), vancomycin-resistant Enterococcus (VRE), and methicillin-resistant Staphylococcus aureus (MRSA), have become a major public health concern due to their resistance to treatment, leading to treatment failure, poor prognosis, and increased mortality rates. Early identification of MDROs is essential to curb their spread. In this study, we assessed the diagnostic performance of CRP, PCT, IL-6, and IL-10 in detecting CRE, CRPA, VRE, and MRSA (as shown in Fig. S2 and summarized in Table 5). Regrettably, these inflammatory biomarkers demonstrated restricted diagnostic effectiveness for CRE, CRPA, and MRSA, with AUC values around 0.6. Nevertheless, when it came to VRE detection, CRP, PCT, and IL-10 exhibited encouraging diagnostic significance, with AUC values of 0.73, 0.75, and 0.75, respectively, as detailed in Table 5. Conversely, IL-6 did not display significant diagnostic significance for VRE, with an AUC value of 0.57. To summarize, CRP, PCT, and IL-10 are valuable diagnostic markers for identifying VRE, while their diagnostic efficacy for other MDROs is relatively limited.
Table 5 Comparison of serum levels of inflammatory biomarkers and AUC between MDRO and NMDROPCT, IL-6, and IL-10 are useful markers for distinguishing pathogen classifications in BSI mouse modelsClinical data can be influenced by various factors, such as disease progression, individual differences, environmental factors, and medical interventions. To exclude the impact of these uncertain factors and validate the accuracy of our results obtained from the retrospective clinical study, we utilized two BSI mouse models (GP-BSI and GN-BSI models) in the second phase of our research. These models were established by tail vein injection with a standard strain of ATCC25923 Staphylococcus aureus (Gram-positive bacteria) and a standard strain of ATCC25922 Escherichia coli (Gram-negative bacteria), respectively. Serum were collected at different time points after bacteria injection to assess serum levels of CRP, PCT, IL-6, and IL-10 in these mouse models. As depicted in Fig. 3, serum CRP levels in both models exhibited a significant increase within the first 3 h after injection of Staphylococcus aureus and Escherichia coli compared to the control, with no significant difference observed between these two groups at this time point. From the third to the twelfth hour after bacteria injection, serum CRP levels in the GP-BSI model were significantly higher than those in the GN-BSI model. However, after 24 h of bacteria infection, the serum CRP level peaked in the GN-BSI group, surpassing that in the GP-BSI group. These results indicate that serum CRP levels vary at different time points during BSI, with a rapid response to Gram-positive bacteria infection. This suggests that CRP is expessed immediately after Gram-positive bacteria infection and plays a critical role in the early stage of such infections (Fig. 3A).
Fig. 3
Inflammatory biomarkers expression levels in BSI models at different time points (1 h, 3 h, 6 h, 12 h, 24th, 48 h). (A) Analysis of the expression level of CRP. (B) Analysis of the expression level of PCT, (C) Analysis of the expression level of IL-6, (D) Analysis of the expression level of IL-10
Interestingly, unlike CRP, serum levels of PCT, IL-6, and IL-10 in the GN-BSI group were consistently higher than those in the GP-BSI group at all time points during 48 h post-infection (Fig. 3B-D). Particularly, IL-6 and IL-10 in the GN-BSI group were significantly higher than those in the GP-BSI group within the first 24 h post-infection. Moreover, serum IL-6 and IL-10 in the GN-BSI group sharply increased within 6 h post-infection, reaching peak levels around 6 h, and then gradually decreased to their original levels within 48 h. These findings demonstrate that PCT, IL-6, and IL-10 are more effective than CRP in differentiating GN-BSI from GP-BSI.
Comments (0)