Pharyngeal injuries can cause deep cervical abscesses in the retropharyngeal space and severe life-threatening complications, such as acute mediastinitis via the prevertebral space [4, 5]. Other life-threatening complications may occur depending on the location and depth of the injury. The introduction of a foreign body posteriorly into the pharynx risks intracranial injury and caution is also required in diagnosing internal carotid or jugular vein injury if the object is introduced laterally [6].
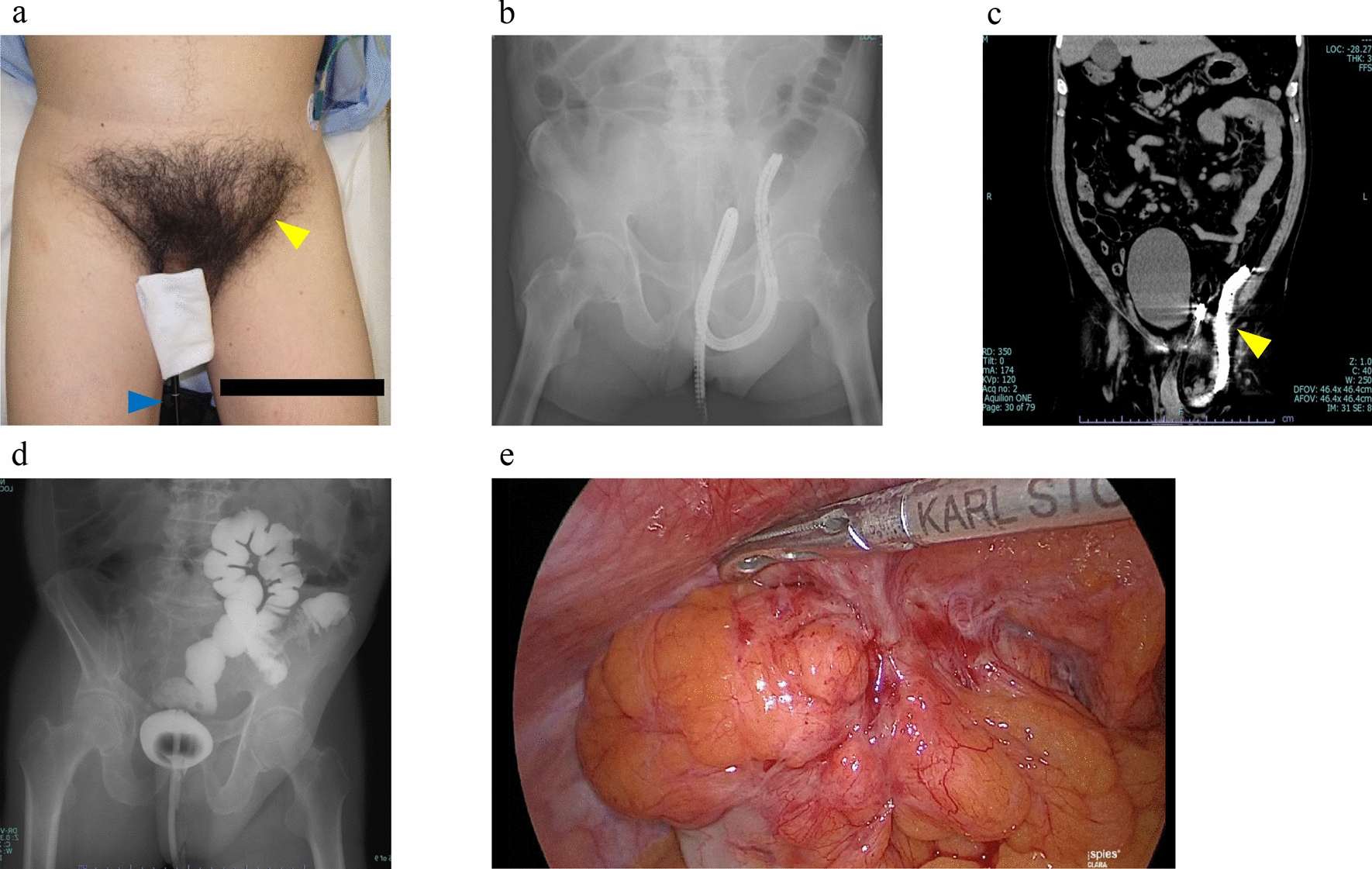
The unique feature of this case is that the patient fell while playing with a marker pen in the mouth, which perforated the pyriform sinus in the hypopharynx, communicating with the posterior pharyngeal space. The perforation site was not clearly identified on initial examination but was eventually identified by pharyngoesophagography. Moreover, the lesion extended into the mediastinum, requiring temporary mechanical ventilation, and was eventually managed by cervical drainage and antibiotic therapy.
The morphological characteristics of the oropharyngeal region in infants and children indicate that the mid-pharyngeal region between the oral cavity and the esophagus is significantly shorter than in adults, which increases the risk of foreign bodies entering the pharynx from the oral cavity. In addition, the pharynx in children is straighter than that in adults. When evaluating oral trauma, it is critical to consider these morphologic features to recognize the increased likelihood of rod-shaped foreign bodies passing through the oropharynx and reaching the pyriform sinus, potentially causing injury [7, 8]. The retropharyngeal space extends from the 6th cervical vertebra to the 3rd thoracic vertebra, and the posterior space continues to the diaphragm. Therefore, perforation of the pharynx can lead to contamination of the mediastinum and eventually reach the upper surface of the diaphragm, causing acute mediastinitis and mediastinal abscess.
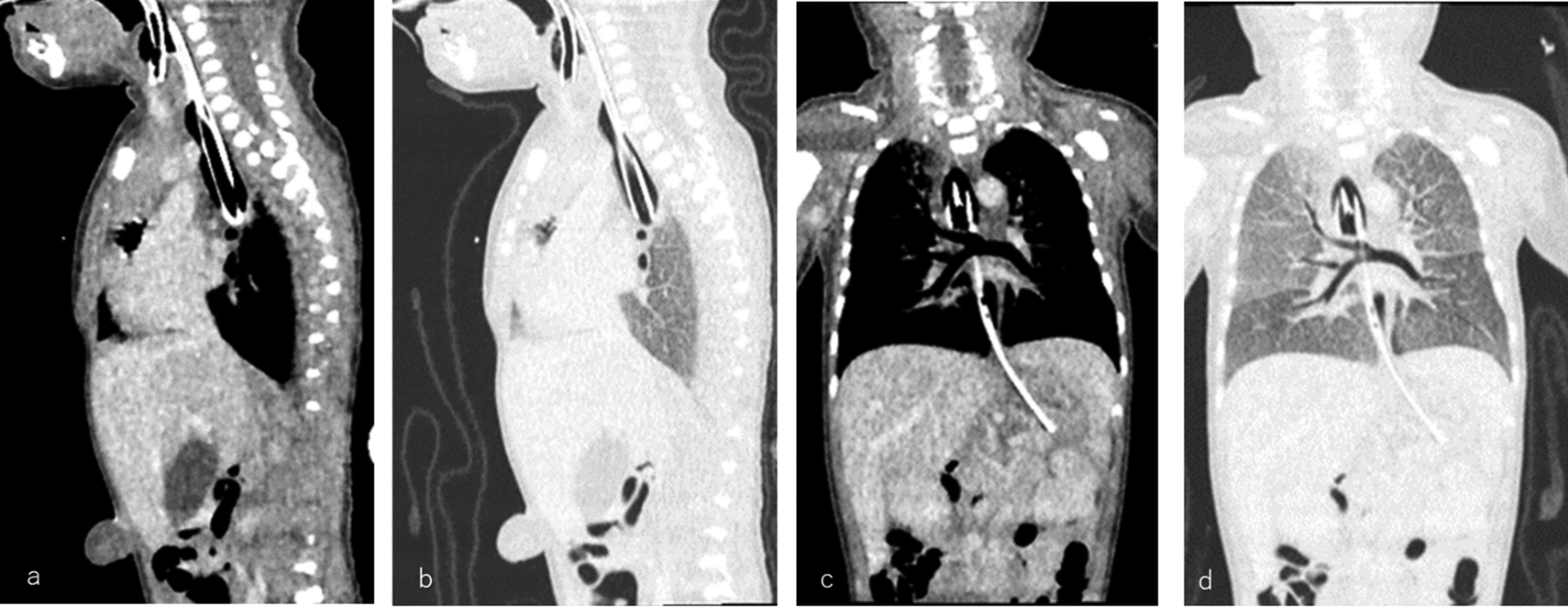
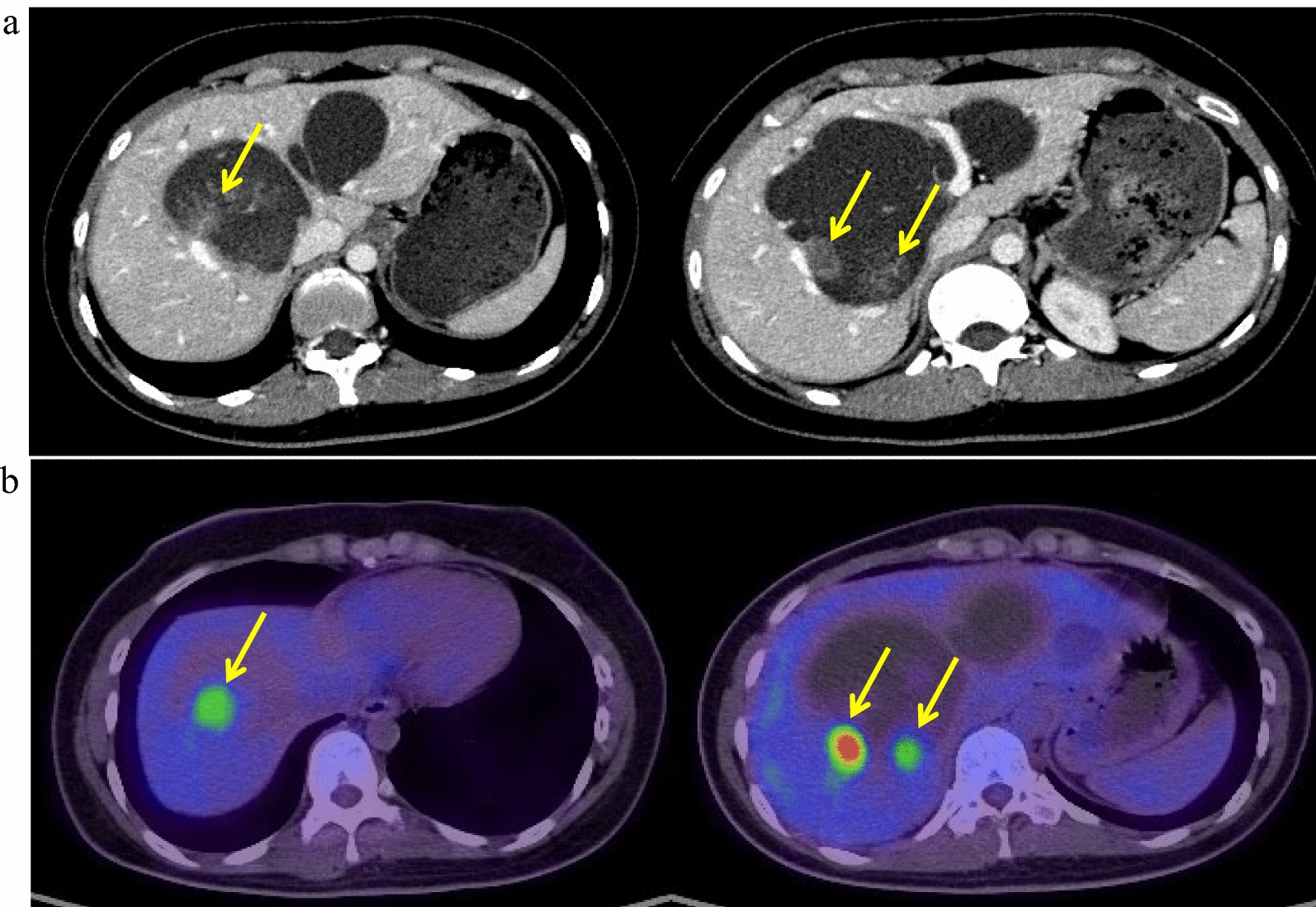
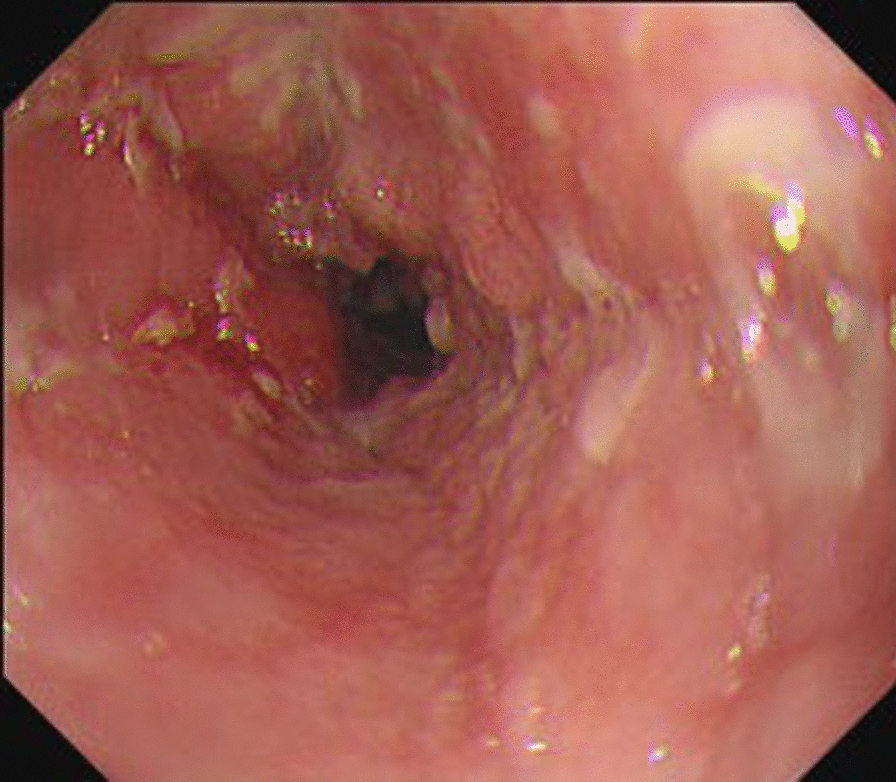
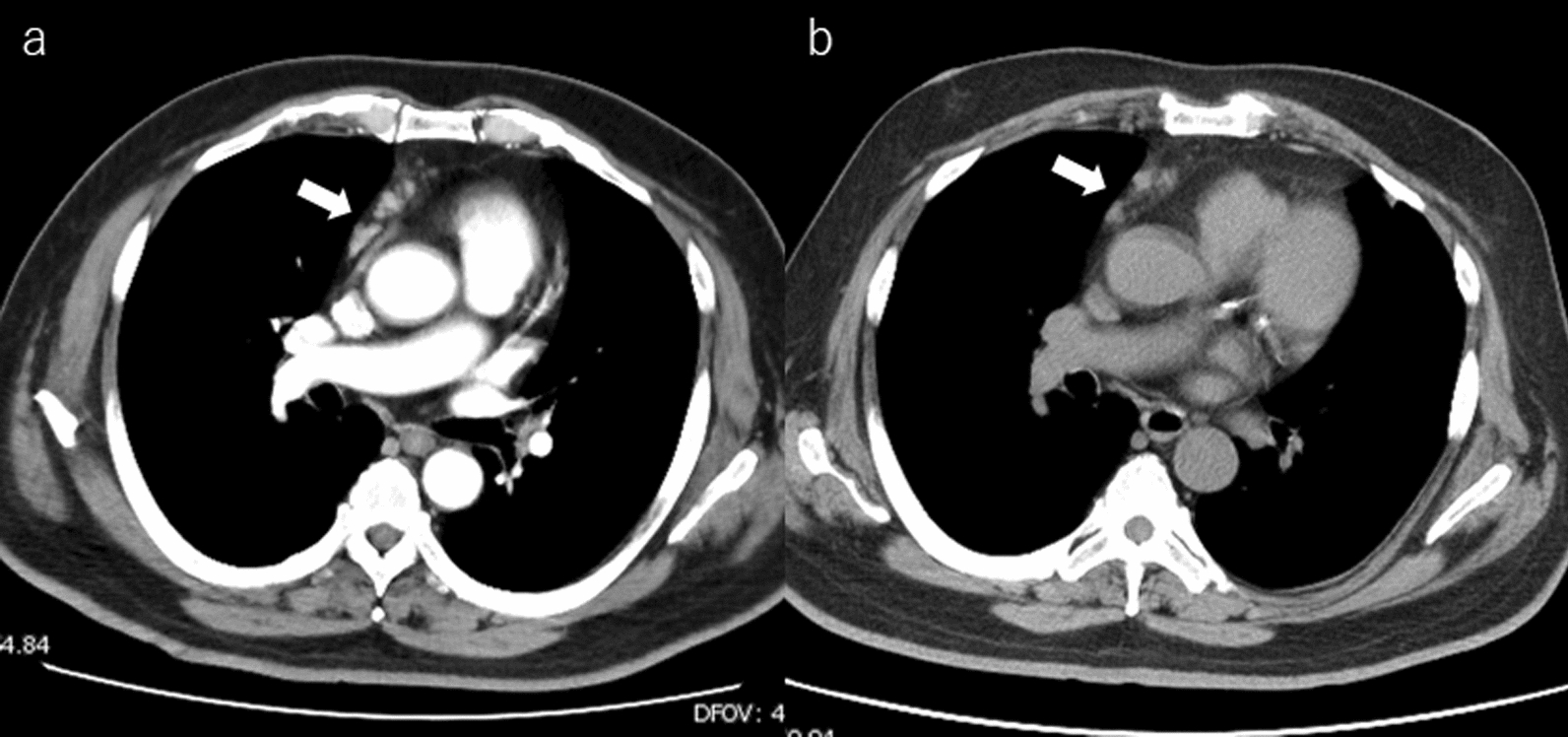
In the case presented, bleeding had ceased at the presentation time, and the laryngoscopy revealed no apparent signs of perforation. However, a CT scan revealed extensive pneumomediastinum from the cervical region. These findings led to early intensive care for the patient. Although the oral cavity and posterior pharyngeal wall can often be visualized, identifying deep injuries in the pyriform sinus can be challenging with laryngoscopy. When deep and severe mediastinitis develops, nonspecific symptoms often manifest within hours, including high fever, cough, chest pain, and dysphagia, followed by progressive dyspnea. In this case, the mucosa of the wound acted as a check valve, and the pneumomediastinum gradually widened due to crying. In cases of discrepancies between the laryngoscopy findings and the patient's symptoms, prompt pharyngoesophagography is necessary [9].
The following management strategy was considered in this case. The patient was intubated and placed under deep sedation for ventilatory management. Although mechanical ventilation is not always necessary in a pneumomediastinum due to pharyngeal trauma, it was deemed necessary in this case, because the lesion was significantly enlarged and at high risk of further expansion.
Antibiotic therapy with or without surgical drainage is the primary treatment [2, 3]. Acute suppurative mediastinitis resulting from pharyngeal injury often involves mixed aerobic and anaerobic bacterial infections, requiring broad-spectrum antibiotic selection. As abscess formation progresses, effective drainage and antibiotic administration become critical. In the present case, the abscesses were localized in the upper posterior mediastinum and deep cervical space and could be drained from the cervical area. In addition, reports explicitly recommend continuous suction with the drain [10], and we also applied continuous suction during the acute phase. However, when antibiotic therapy and surgical drainage fail to improve the condition, using fascial flaps to cover the perforated area can be considered a life-saving intervention. There are several options for fascial flap use [11], and the most appropriate method is chosen on a case-by-case basis. Despite the anticipated large injury site, outpatient enteral nutrition management via a nasogastric tube was deemed feasible. The patient's overall condition was stable, and since reliable drainage management and enteral nutrition could be achieved in the outpatient setting, further invasive surgical intervention was deemed unnecessary.
Raising parental awareness of the risk of complications associated with pharyngeal injuries is critical, and medical professionals should be aware that early recognition and prompt intervention can improve patient outcomes [2, 5, 6]. These incidents are notably reported in children aged 1–2 years, especially as they begin to walk independently. Infants are naturally curious and often explore their environment by putting objects in their mouths. Although products for younger children display warnings about throat-stabbing dangers, there is still insufficient awareness of the potentially fatal consequences of foreign body ingestion.
Pharyngeal trauma should be considered a possibility of abuse if it occurs at an unnatural age or if other physical abnormalities are present. In cases of abuse, there may be a delay in seeking medical attention [12]. It is crucial to consider the possibility of abuse if there is a significant delay between the injury and seeking medical attention.


Comments (0)