
Remember me
The data for the main goal of the study are based on a community-based prospective cohort of older adults (n = 9940) followed up for 17 years (the ESTHER study). ESTHER participants were recruited in 2000–2002 through general practitioners (GPs). The eligibility criteria were age between 50 and 75 years, sufficient knowledge of the German language, residence in the German state of Saarland, and willingness to attend a general health examination performed by GPs. To not impair the generalizability of the study, no specific exclusion criterium based upon cognitive functioning was applied [18, 19]. Blood samples collected at baseline were stored at − -80 °C. Follow-up measurements were conducted 2, 5, 8, 11, 14, and 17 years after baseline. All participants filled in a health questionnaire and GPs provided medical records.
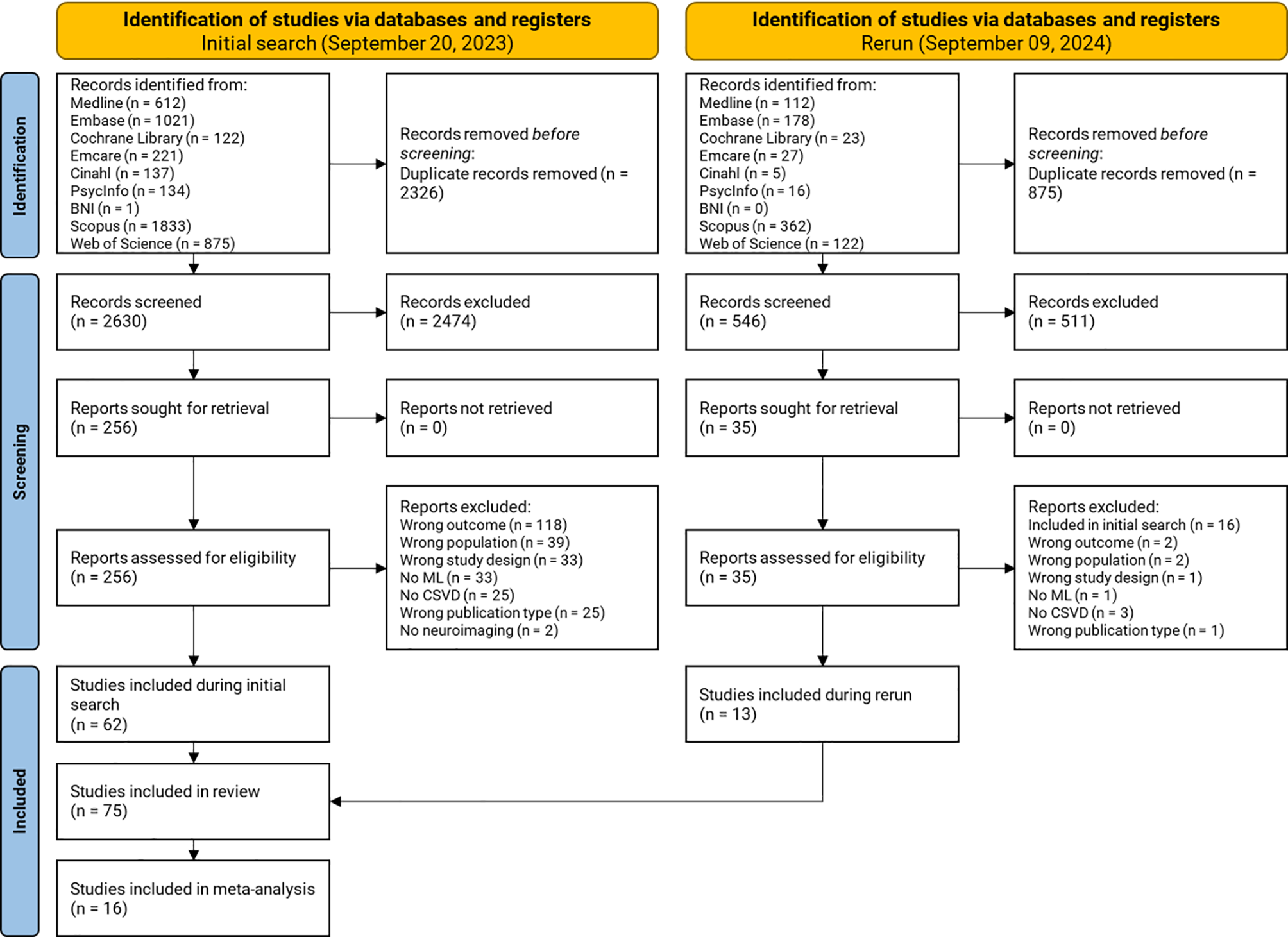
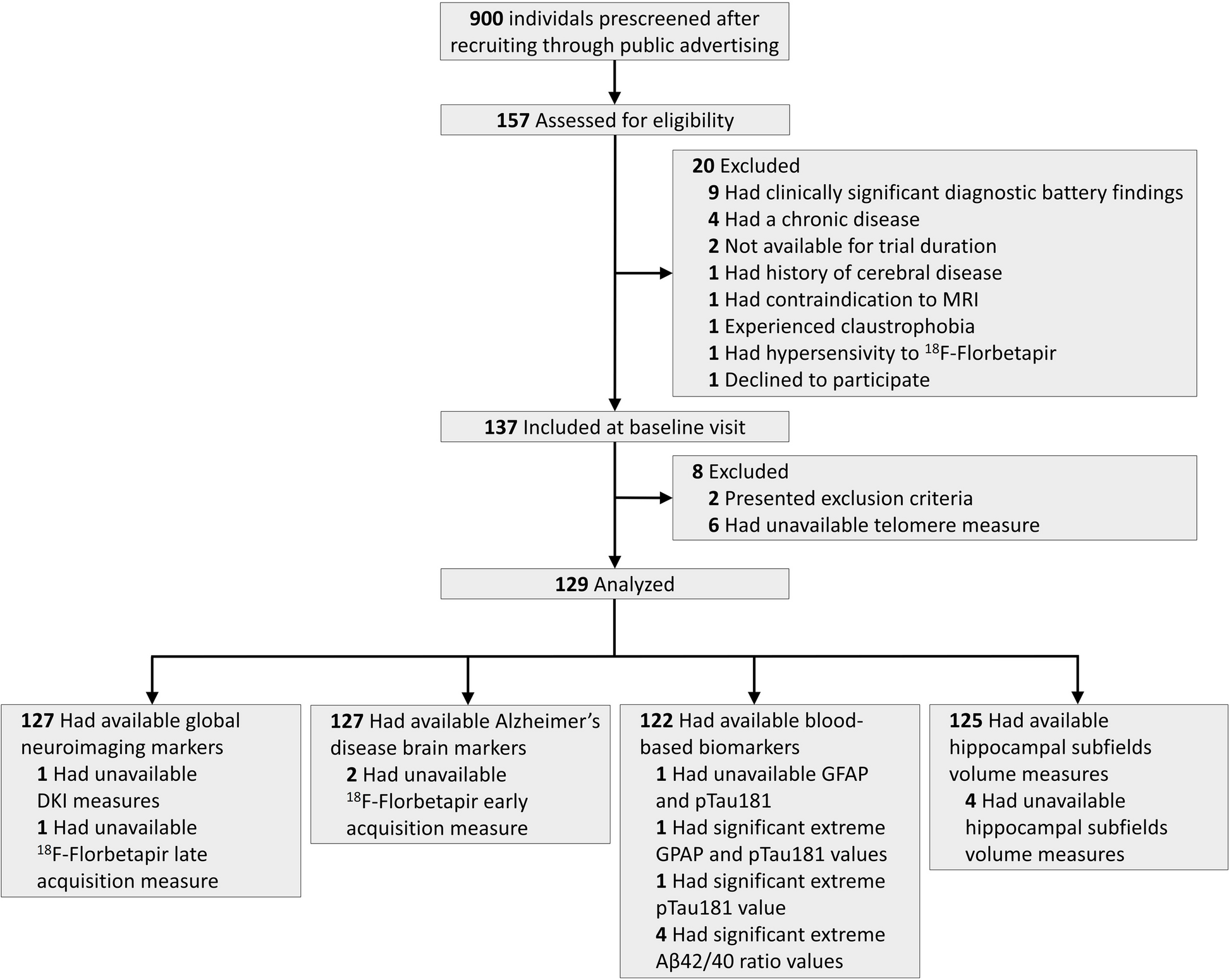
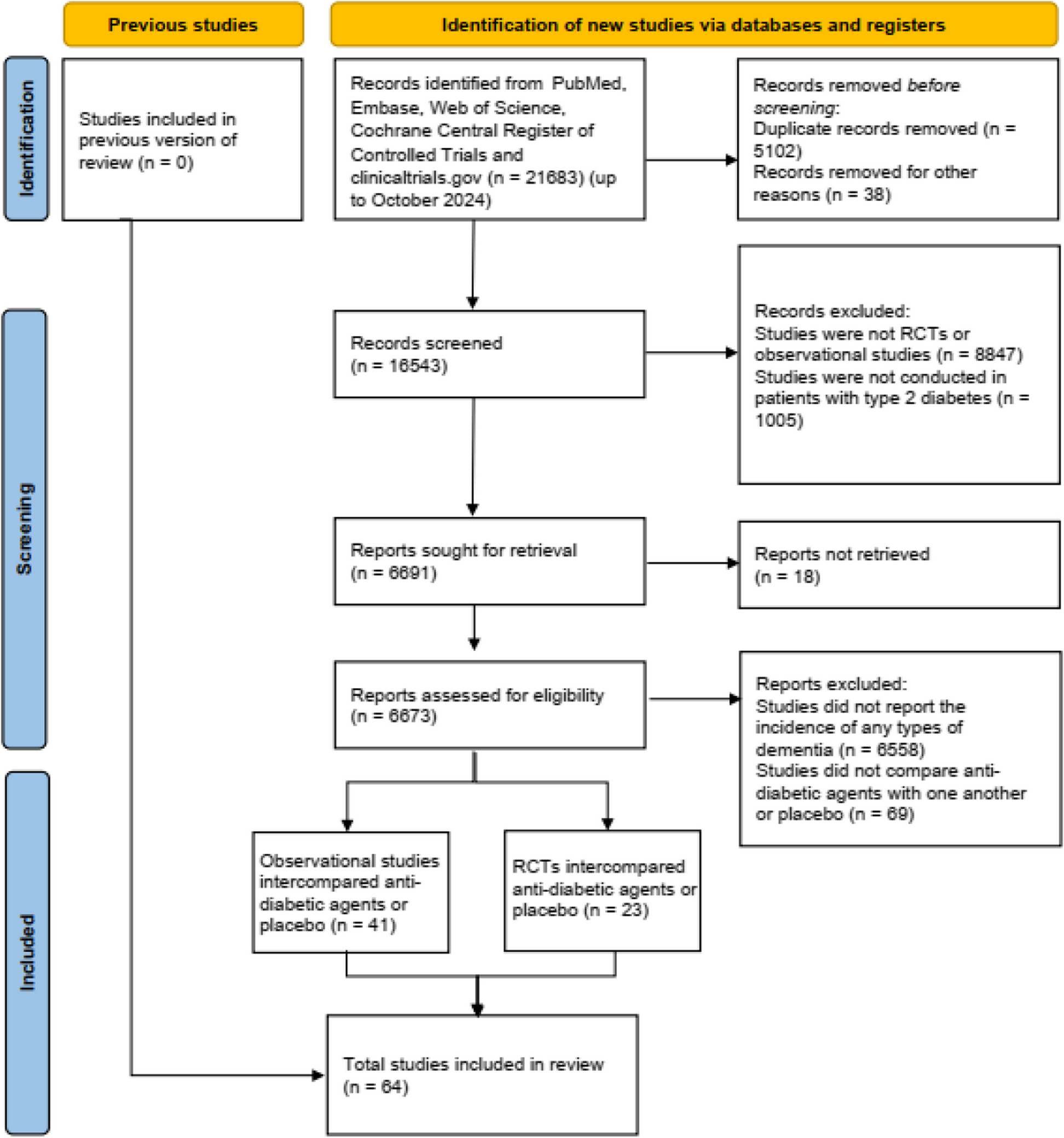
During the 14- and 17-year follow-up, the GPs of all ESTHER study participants, including those of participants who had dropped out of the study or had died, were contacted and were asked to provide information relating to a diagnosis of dementia since enrollment and to send the corresponding medical records, if available. In total, GPs of n = 6357 participants provided usable dementia diagnosis information (Fig. 1). For the purpose of this study, participants with incomplete information relating to SCC (n = 421) and with a dementia diagnosis between recruitment and 2-year follow-up measurement were excluded. Specifically, in order to minimize the possibility of undiagnosed dementia at baseline, we excluded all participants with a diagnosis of dementia dated up to 3 years after recruitment (n = 10), so that n = 5926 ESTHER participants remained for the analyses relating to the outcome all-cause dementia. For the outcome relating to the risk of a first depressive episode in the absence of dementia participants with an incident diagnosis of dementia over all follow-up measurements were additionally excluded (n = 451) , because these analyses aimed to disentangle depression from all-cause dementia. Furthermore, participants with incident depression between baseline and the 2-year follow-up (n = 114), with a lifetime history of depression (n = 790), and with missing information on incident depression (n = 1) were also excluded, reducing the final sample to n = 4570 for the outcome depression in the absence of dementia.
Fig. 1
Flow chart of the ESTHER study
Clinic-based dataThe data relating to the secondary aim of the study dealing with the comparability of the informative value of SCC in community and clinical settings are cross-sectional, and they were collected within the memory clinic embedded in the Alzheimer Treatment and Research Center (ATFZ) at the Department of Psychiatry and Psychotherapy of the University Hospital of Munich (LMU) between August 2020 and November 2022. The eligibility criteria were age ≥ 60 years, a voluntary appointment with the memory clinic in order to receive dementia diagnostics, and the capacity to give informed consent. The exclusion criteria were illiteracy, insufficient knowledge of the German language, and inability to fill in health questionnaires due to cognitive deterioration.
All patients contacting the memory clinic for dementia diagnostics and fulfilling the inclusion criteria were included in this study. During the recruitment time, all ATFZ patients, in addition to receiving standardized procedures for dementia diagnostics, were asked to complete a comprehensive health questionnaire, which was sent via mail, including exactly the same subjective cognitive questions included in the health questionnaire administered to the ESTHER participants. In total, n = 430 patients ≥ 60 years were recruited.
Assessment of dementiaDementia diagnoses in the ESTHER cohort were made in community settings with heterogeneous diagnostic procedures, and the most common diagnoses were Alzheimer’s dementia (n = 165) and vascular dementia (n = 200). However, according to the available medical records, cerebrovascular pathologies (especially vascular encephalopathy, cerebral infarction, microangiopathy) were highly prevalent among dementia cases, including those cases reported as Alzheimer’s dementia. As explained in more detail in a previous work [20], we hence assume that in the ESTHER cohort, independently of the specific dementia type reported as the primary diagnosis, mixed pathologies were most likely to be present in the great majority of dementia cases, and we therefore grouped all dementia diagnoses in one category called “all-cause dementia.”
In the memory clinic, dementia diagnostic procedures included neuropsychological assessment based on the Consortium to Establish a Registry for Alzheimer’s disease – neuropsychological assessment battery plus (CERAD-plus); neurological, physical, and psychiatric examinations; blood tests; electroencephalogram; brain structural MRI scans; and, if appropriate, a lumbar puncture for markers of neurodegeneration. Dementia diagnoses included Alzheimer’s disease, vascular dementia, mixed dementia, Lewy body dementia, Parkinson’s disease dementia, and unspecified dementia. In order to enhance comparability with the ESTHER sample, we grouped all dementia forms reported in the memory clinic in one category (dementia yes/no).
Assessment of depressionBoth in the ESTHER study and in the memory clinic sample, diagnoses of depression were principally made according to the International Classification of Diseases (ICD-10), because this is the official classification for the encoding of medical diagnoses in Germany.
In the ESTHER study, diagnoses of depression were made in community settings by different medical doctors according to the ICD-10 classification, and they were mostly based on clinical observations involving heterogeneous procedures. The outcome depression indicated the first depressive episode occurring during the follow-up duration of the ESTHER study. Specifically, it indicated a medical diagnosis collected at the 2-, 5, 8-,11-, 14-, and 17-year follow-up among participants without a lifetime history of depression. The medical diagnoses were self-reported and collected through health questionnaires administered to participants.
In the memory clinic sample, diagnoses of depression were made following standardized psychiatric and neurological examinations. The 15-item Geriatric Depression Scale (GDS) was routinely administered as a possible support to clinical observations with a value ≥ 5 indicating depressive symptoms. Among participants of the memory clinic, the diagnosis of depression points either to a first depressive episode or to recurrent depression.
Assessment of SCCIn the self-administered health questionnaire of the ESTHER study at baseline, the following question relating to short-term memory was asked: “Do you have difficulty remembering things that have happened in the recent past (hours to a few days? yes/no).” In the 2-year follow-up, this memory question was replaced by three more specific cognitive questions: “Please, mark if the following statements apply to you just sometimes, always, or never. (1) Lately, I confuse names, phone numbers, or dates; (2) Lately, I misplace things; (3) Lately, I forget names and numbers.” All three cognitive questions were coded with a score ranging from 0 to 2 (0 = never, 1 = sometimes, 2 = always) so that the total score ranged from 0 to 6 with 0 indicating no complaints at all and 6 indicating very frequent complaints in all cognitive questions. To increase the reliability of the self-reported complaints, a combination of the baseline question relating to the short-term memory and of the 2-year follow-up total score was used. The cognitive groups were categorized as follows: (1) no SCC—participants with 0 points in the total score and no short-term memory difficulties (reference group); (2) occasional SCC—participants with > 0 and ≤ 2 points in the total score independently of short-term memory difficulties; and (3) persistent SCC—participants with ≥ 3 points in the total cognitive score and short-term memory difficulties.
The self-administered health questionnaire of the memory clinic included exactly the same three cognitive questions as those included in the ESTHER questionnaire described above. The question relating to the short-term memory was either reported directly to the study doctor or in the health questionnaire, and it was reported at the same time point as the three cognitive questions. The scoring system was the same as the one used for the ESTHER cohort.
Laboratory measurementsBlood biomarkers of neurodegenerative diseasesConcentrations of GFAP, NfL, and p-tau181 in the blood were measured in a subgroup of the ESTHER cohort in a nested case–control design consisting of 261 all-cause dementia cases and 507 controls [20]. The measurements were performed in a single batch in lithium-heparin plasma of baseline samples at the Center for Protein Diagnostics (PRODI) of the Ruhr-University Bochum (Germany) using the single molecule array (SIMOA) Neurology 4-Plex E Advantage Kit and pTau-181 Advantage V2 Kit (Quanterix, USA) on a HD-X Analyzer as per the manufacturer’s instructions [21]. Measurements of amyloid beta could not be used due to its low levels in lithium-heparin plasma [22]. After excluding participants with missing information relating to SCC (n = 61) and dementia development up to 3 years from recruitment (n = 5), n = 702 participants remained for analyses with biomarkers (Fig. 1).
APOE ε4 genotypingAPOE ε4 genotype was determined based on allelic combinations of single nucleotide polymorphisms (SNP) rs7412 and rs429358 using TaqMan SNP genotyping assays. Genotypes were analyzed in an endpoint allelic discrimination read using a PRISM 7000 Sequence detection system (Applied Biosystems) [20].
Other variablesBoth in the population and in the memory clinic setting, sociodemographic and health variables were included in the participants’ questionnaire and partially collected or validated through available medical records. In the clinic setting, such data were additionally collected by study doctors during the anamnesis.
Statistical analysesDescriptive statistics were used to show the baseline characteristics of the cohorts.
Multivariable logistic regression models were run to assess associations of SCC, APOE ε4, and markers of neurodegenerative diseases alone or in combination with risk of all-cause dementia and risk of depression in the absence of dementia. Logistic regression models were adjusted for age (continuous), sex, educational level, lifetime history of stroke, myocardial infarction, diabetes, lifetime history of depression, and APOE ε4 (except in models including APOE as the independent variable of interest). In the clinic-based sample, the reference category for the logistic regression models included both the absence of SCC and occasional SCC because patients with no SCC were too few. The models performed with clinical data were adjusted for age (continuous), sex, and educational level (continuous). Biomarker values were divided in the respective study populations into quartiles (Q), and the highest quartile (Q4) was compared with the other three quartiles (Q1–3), which served as the reference group. Participants carrying the APOE ε4 allele (ε2ε4, ε3ε4, ε4ε4) were classified as APOE ε4 + and those not carrying the ε4 allele (ε2ε2, ε3ε2, ε3ε3) as APOE ε4 − . The results were presented as odds ratios (OR) and 95% confidence intervals (CI). For the cross-sectional data collected in the memory clinic setting, we performed additional sensitivity analyses excluding participants with mild cognitive impairment (MCI). The statistical software SAS, version 9.4, Cary, NC, USA, was used for all data.
Comments (0)