Participants
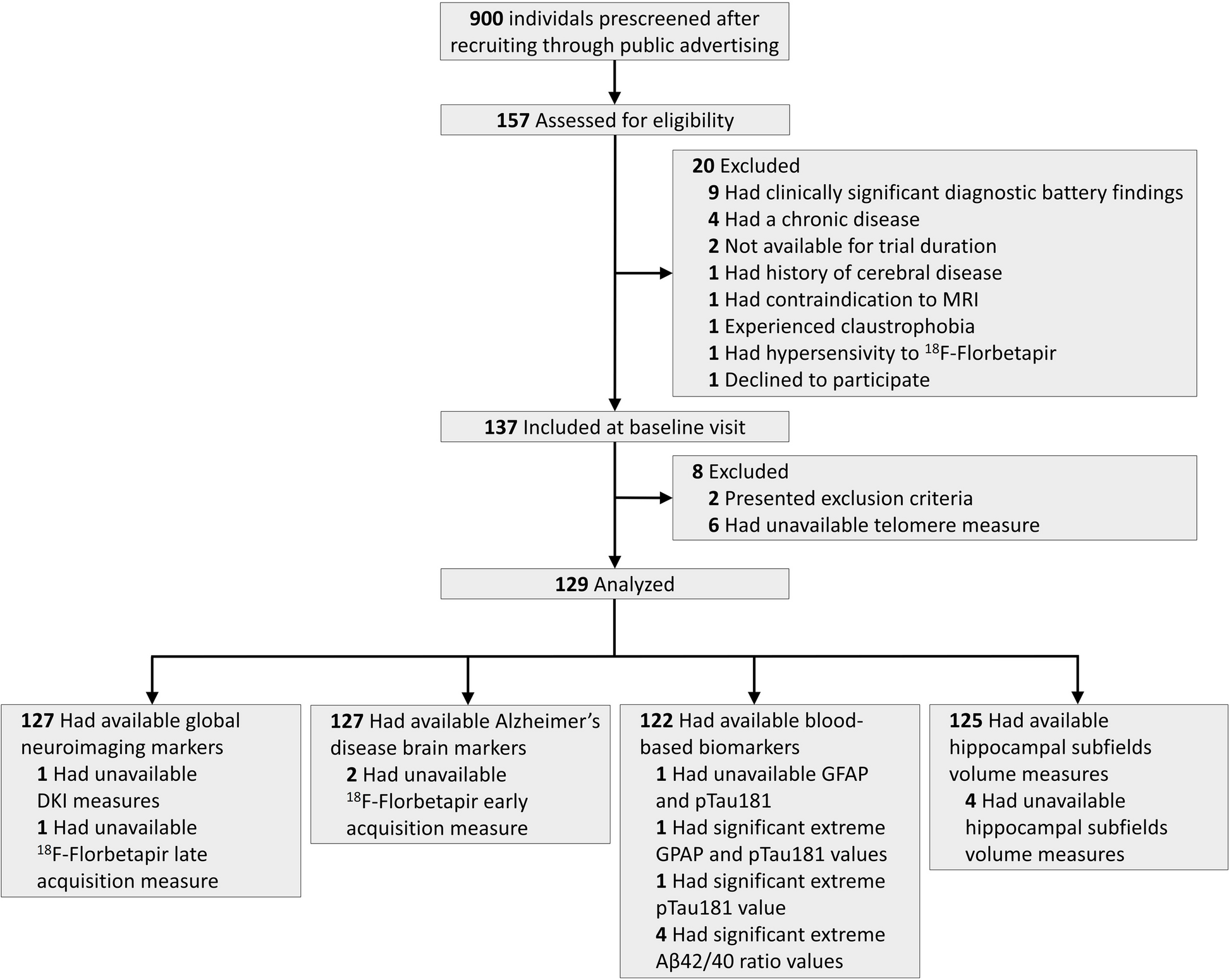
This study included 158 native Chinese participants, all from an ongoing longitudinal study that collected comprehensive brain imaging and neurocognitive test data in an elderly community-dwelling sample, the Beijing Aging Brain Rejuvenation Initiative (BABRI) [9], which comprises a large database of 9532 records. The participant inclusion criteria were as follows: (1) more than 6 years of education; (2) aged between 50 and 80 years old; (3) right-handed; (4) scored no less than 24 on the Mini-Mental Status Examination (MMSE), Chinese version; (5) no history of nephritis, coronary disease, gastrointestinal disease, tumors, psychiatric illness, or dementia; (6) no contraindications to MRI; (7) availability of complete neuropsychological tests for MCI assessment. The Ethics Committee and Institutional Review Board of Beijing Normal University’s Imaging Centre for Brain Research approved this study (ICBIR_A_0041_002.02), and all participants provided written informed consent. The MRI data from his/her first visit for each participant were selected for the current analysis together with the neuropsychological test measures. The flowchart of participant selection is shown in Supplemental Fig. 1.
Neuropsychological testing
Each participant completed a series of neuropsychological tests, including the MMSE [10] and five other tests of cognitive domains: (1) memory, delay, and total part of the Auditory Verbal Learning Test (AVLT) [11] and the Rey-Osterrieth Complex Figure (R-O) test-recall [12]; (2) visual ability, the Rey-Osterrieth Complex Figure (R-O) test-copy and the Clock-Drawing Test (CDT) [13]; (3) language, the Category Verbal Fluency Test (CVFT) [14] and the Boston Naming Test (BNT) [15]; (4) attention, the Symbol Digit Modalities Test (SDMT) [16] and Part A of the Trail-Making Test (TMTA) [17]; (5) execution, time index of Part C of the Stroop Test [18] and Part B of the Trail-Making Test (TMTB).
The diagnosis of MCI was made following Petersen’s criteria [19] and was performed by expert neurologist Z.J.Z. with 27 years of experience in clinical neurology and Y.J.C., a researcher with 12 years of research experience in the field, both blinded to the results of MRI. The validation of the diagnosis was performed by D.C. at the time of subject inclusion. The accuracy of the diagnosis was ensured by evaluating each cognitive domain with 2–3 cognitive tests. Impairment in a specific domain was determined if the participant had at least two cognitive test scores that were more than 1.5 standard deviations below the age- and education-adjusted norm. Specifically, aMCI was diagnosed based on memory impairment, while naMCI was diagnosed based on intact memory and the impairment of at least one other cognitive domain (i.e., visual ability, language, attention, and/or executive function). Drawing upon the aforementioned criteria, we classified the baseline data of 5990 individuals with assessable MCI into the following categories: 4822 individuals exhibited normal cognitive function elderly, 480 were diagnosed with single-domain aMCI, 480 with naMCI, and 208 with multi-domain aMCI (MCI with memory impairment and impairment in one or more additional cognitive domains). Furthermore, within the dataset containing baseline MRI records from 953 individuals, we identified 24 cases of multi-domain aMCI (see Supplemental Fig. 1). The participants included in our final analysis of this current study were aMCI group which consisted of participants with single-domain impairment only, while the naMCI group included participants with single- or multi-domain impairments, aimed at better distinguishing between MCI with and without memory impairment. The normal control group included participants who demonstrated no impairment on all the above cognitive tests, no subjective cognitive complaint, and were matched on demographic variables and numbers with the other groups. The final sample consisted of 50 normal control individuals, 56 aMCI individuals, and 52 naMCI individuals. DTI data from 6 aMCI and 1 naMCI subject were excluded due to quality issues.
Image data acquisition
Structural magnetic resonance imaging data were collected by a Siemens Trio 3.0 Tesla scanner (Trio; Siemens, Erlangen, Germany) in the Imaging Center for Brain Research at Beijing Normal University. Participants laid supine with their head snugly fixed in place by straps and foam pads to minimize head movement. T1-weighted, sagittal 3D magnetization-prepared rapid gradient echo sequences were acquired of the entire brain [sagittal slices = 176, repetition time (TR) = 1900 ms, echo time (TE) = 3.44 ms, slice thickness = 1 mm, flip angle = 9°, inversion time = 900 ms, field of view (FOV) = 256 × 256 mm2, acquisition matrix = 256 × 256]. Each participant underwent two sets of DTI sequences with the following scan parameters: TR = 9500 ms; TE = 92 ms; 30 diffusion-weighted directions with a b-value of 1000 s/mm2, and a single image with a b-value of 0 s/mm2; slice thickness = 2 mm; no inter-slice gap; 70 axial slices; matrix size = 128 × 128; field of view (FOV) = 256 × 256 mm2; and voxel size = 2 × 2 × 2 mm3.
Image data processing
T1 imaging data was pre-processed using Statistical Parametric Mapping 12 (SPM12: www.fil.ion.ucl.ac.uk/spm) via MATLAB R2012b (MathWorks Inc., MA). The CAT toolbox within SPM12 was utilized to perform voxel-based morphometry analysis [20]. The images were skull-stripped and bias-corrected and segmented into gray matter, white matter, or cerebrospinal fluid maps which were normalized with the DARTEL algorithm and smoothed with an 8-mm full-width half-maximum Gaussian kernel. Total intracranial volume (TIV) was computed for each participant by summing the volumes of gray matter, white matter, and cerebrospinal fluid and used as a covariate in the subsequent analysis.
The DTI data were pre-processed using the Pipeline for Analyzing braiN Diffusion imAges (PANDA: www.nitrc.org/projects/panda/) through MATLAB. The data was coregistered to the b0 image using an affine transformation to correct the eddy-current induced distortions and simple head-motion artifacts. Then, the diffusion gradient directions were adjusted, and tensor matrix and diffusion tensor metrics were calculated, with the main focus being fractional anisotropy (FA). A seed-based approach was used for deterministic fiber tracking, with fibers crossing the seed point being included without directional restrictions. The stopping criteria were an FA value of at least 0.2 and a bending angle not exceeding 45° within a voxel.
Statistical analysis
The voxel-wise gray matter volumes were compared among aMCI, naMCI and control groups using SPM12 after adjusting for age, sex, years of education, and TIV. The significance level was set at a voxel-level p < 0.001 with a cluster-level p < 0.05 (GRF-corrected). The volumes of significant gray matter clusters were compared between groups, and cluster masks were used in the subsequent white matter analyses.
Comparison of the structural connectivity among groups was based on inseparable local brain volume. The deterministic fiber tracking in each individual DTI space was passed through the seeds from the gray matter analysis. In addition, to explore the change pattern of different directions and distances of fiber bundles, we segmented the tracked fibers with the center point of gray matter region along the three orthogonal directions in the 3D space (X, Y, Z in MNI coordinates) separately on the average value of each participant. The number of fiber bundles and each segment among groups were compared with the significance level at p < 0.05 with FDR-corrected over segments.
Correlations between neuroimaging indices and cognitive test scores (corrected for age, gender and education) were computed, with a significant level at p < .05 to make these changes of neuroimaging indexes be meaningful and interpretable. Moreover, mediation analyses were performed with gray matter volume and white matter fiber bundle number, both serving as an independent variable and a mediator, and cognitive test scores as the dependent variable. The analyses were performed using bootstrap method to determine which of the local regions’ volume or connectivity is more directly relevant to cognitive functions across all populations in this study.
Data availability statement
Data and code used in this study can be provided upon request to the authors after establishing a formal data sharing agreement.

Comments (0)