
Remember me
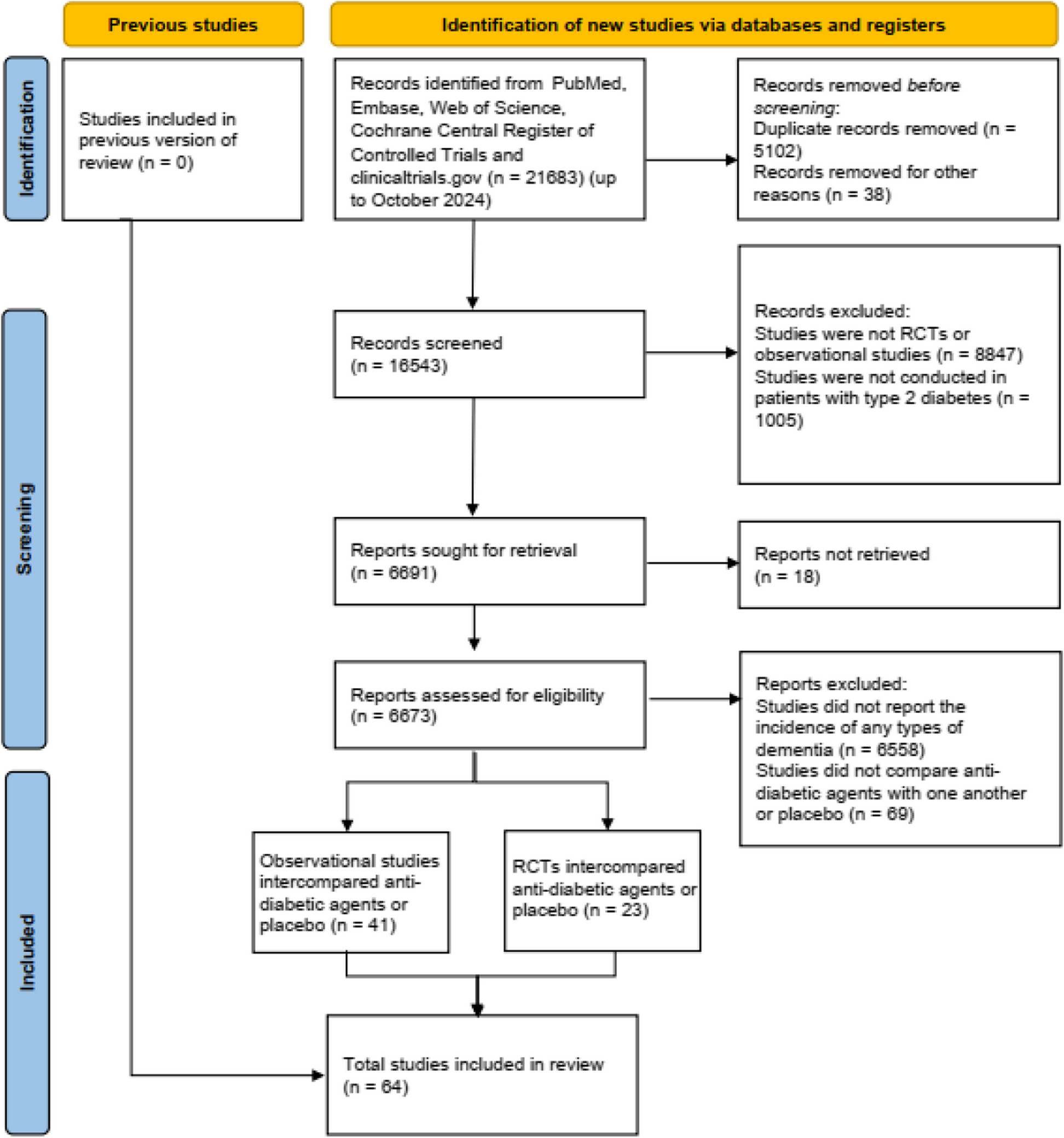
All subjects included in the present analysis were participants, from the MAPT and MAPT-PLUS studies, that were tested for amyloid blood biomarkers (Fig. 1). MAPT was a multicenter (13 memory centres in France and Monaco), randomized, placebo-controlled, 3-year trial whose objective was to assess effect of MI and omega 3 on cognitive performance. MAPT-PLUS was a 2-year observational and optional extension of MAPT after completion of the interventional program [1]. The objective of MAPT-PLUS was to evaluate the long-term cognitive effect of MAPT preventive strategies. This additional follow-up was systematically offered to MAPT participants during the end-of-study visit.
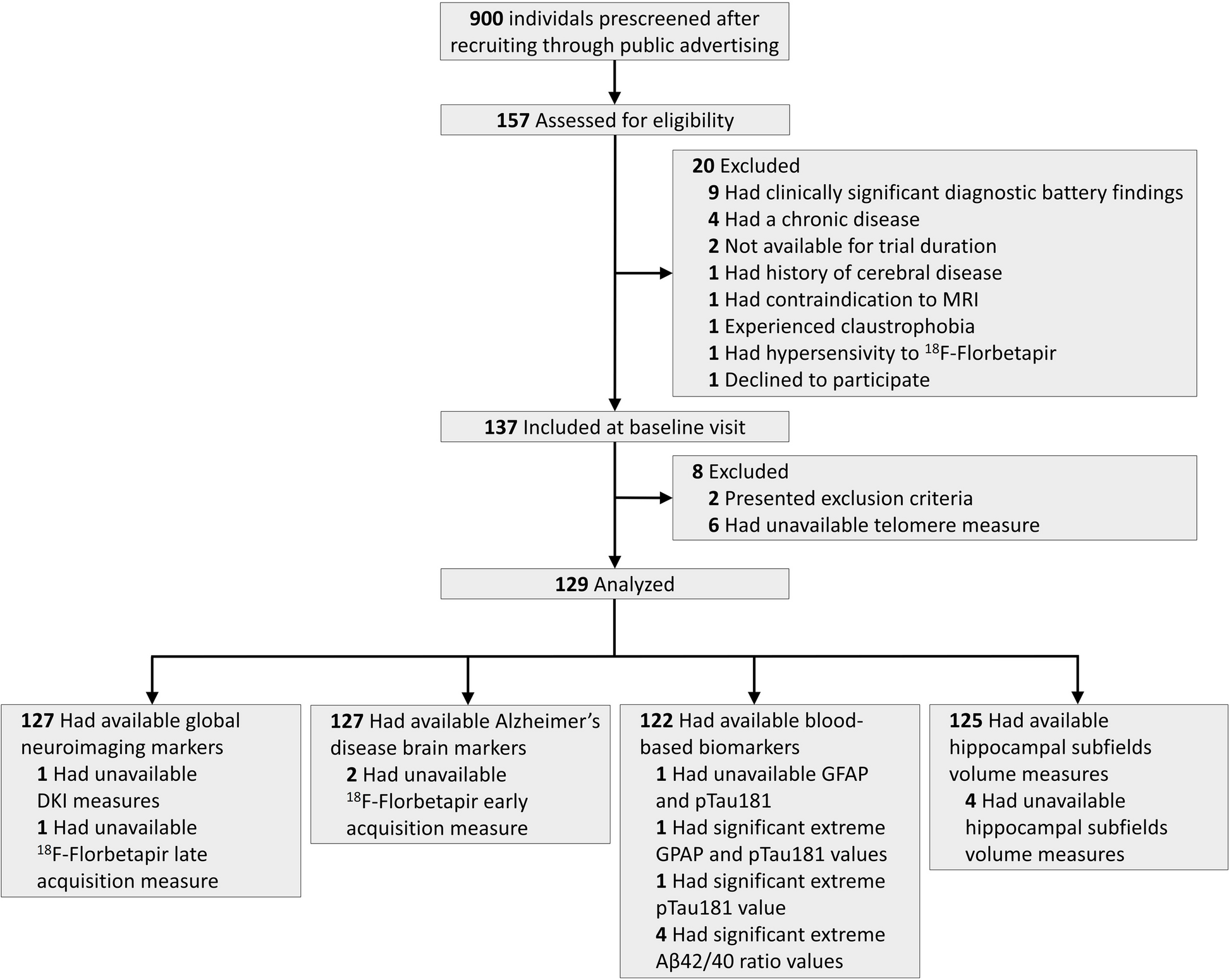
Fig. 1
Place of the amyloid plasma analysis in relation to MAPT and ancillary studies. MAPT multidomain Alzheimer’s preventive trial
Based on MAPT inclusion criteria, subjects included in the present analysis were non-demented, 70 years old and over, and fulfilled one of the following three criteria: spontaneous memory complaint, limitation in one instrumental activity of daily living, or slow gait speed [2].
Randomization and maskingIn MAPT, participants were randomly assigned (1:1:1:1) to the MI plus omega 3, MI plus placebo, omega 3 alone, or placebo alone group. A computer-generated randomization procedure was used with block sizes of eight and stratification by center. A clinical research assistant used a centralized interactive voice response system to identify which group to allocate the participant and which lot number to administer [2]. All participants and research staff including neuropsychologists were blinded to omega 3 or placebo assignment and to amyloid blood status.
ProceduresParticipants took two capsules of either the placebo or omega 3 daily. The active supplement used was V0137, an oil mixture containing natural fish oil with a minimum of 65% docosahexaenoic acid (400 mg) and a maximum of 15% eicosapentaenoic acid (no more than 112.5 mg). As described previously, MI program consisted of 12 2-h group sessions focusing on three domains (cognitive stimulation, demonstrations of physical activity, and nutritional advice) and a preventive consultation for the management of cardiovascular risks at baseline, 12 and 24 months [2]. This interventional program lasted 3 years, and 2-year observational follow-up was added in MAPT-PLUS.
Clinical visits in MAPT and MAPT-PLUS were scheduled every 6 or 12 months to assess physical and functional conditions and adherence [1]. Cognitive assessment included the Free and Cued Selective Reminding Test (FCSRT) [13], the Controlled Oral Word Association Test and Category Naming Test (CNT) [14], the Digit Symbol Substitution Subtest of the Wechsler Adult Intelligence Scale–Revised [15], the Trail-Making Tests [16], the Mini-mental State Examination [17], and the Clinical Dementia Rating scale (CDR) [18]. Physical evaluation included the Short Physical Performance Battery (SPPB) [19] and Fried frailty criteria [20]. Autonomy in daily living activities was evaluated by the Alzheimer’s disease Cooperative Study-Activities of Daily Living Prevention Instrument (ADCS-ADL) [21]. One blood sample of 15 ml (10 ml in an EDTA vacutainer and a pair of × 2.5 ml in PAXgene RNA tubes) was collected yearly for the biobank. These samples were transferred directly at ambient temperature to the Cellular Biology and Cytology Laboratory at each site. The two PAXgene RNA tubes were frozen at −20° directly. The EDTA tube was centrifuged then aliquoted; the serum and the pellet were collected in two 5-ml dry tubes, then frozen at −20°. A biobank scientific committee has identified amyloid blood biomarkers as a research priority.
Plasma Aβ42/Aβ40 immunoprecipitation/mass spectrometry assay methodsPlasma samples of 0.46 ml were assessed to test plasma Aβ42 and Aβ40 levels by immunoprecipitation mass spectrometry as previously described [9, 22]. Aβ levels were analyzed and calculated by integrated peak area ratios to known concentrations of the internal standards using the Skyline software package [23].
Aβ42/Aβ40 cutoff (≤ 0.0107) has been defined, by Randall Bateman laboratory at Washington University School of Medicine in Saint-Louis, to discriminate as accurately as possible negative and positive amyloid participants in comparison to PET [24]. Indeed, many subjects included in the present analysis (n = 233) were participants from MAPT-AV45 with amyloid PET (Fig. 1). In the MAPT-AV45 study, the positivity threshold for amyloid PET was set at SUVr > 1.17 [4].
AdherenceFor omega 3 supplementation and placebo, subjects were considered as adherent if they returned less than 25% of the prescribed capsules. For MI program, participants were considered as adherent if they attended at least 75% of the group sessions (if applicable) [2].
Primary outcome and objectivesThe primary outcome measure was the change in cognitive composite score after a 1, 3, and 5-year follow-up. We used a composite of four measures, close to the PACC (Preclinical Alzheimer Cognitive Composite), well established to show sensitivity to decline in early stages of AD [25]. The MAPT cognitive composite score has been already described previously [2, 4, 26]. This cognitive composite score was calculated by combining FCSRT, CNT, Digit Symbol Substitution Subtest, and MMSE orientation scores.
The main objectives were to assess according to amyloid blood status: (1) the cognitive effect of MAPT interventions at 12 and 36 months and (2) the long-term impact at 60 months after 2-year interruption of these interventions.
Statistical analysisAnalysis was completed in the intention-to-treat (ITT, n = 483) and per-protocol (n = 457) populations. The ITT population consisted of all randomly assigned participants who completed a cognitive composite score at baseline and a minimum of one post-baseline visit. Per-protocol population excluded all major protocol violations at baseline and during follow-up [2]. Efficacy in subgroups according to amyloid blood status was assessed by post-hoc analysis.
We used the same statistical method as for the work carried out to determine the cognitive effect of MAPT interventions according to PET amyloid status [4]. Linear mixed-model repeated-measures analyses were used including baseline, 6, 12, 24, 36, 48, and 60-month follow-up data to assess between-group differences in the change in cognitive composite score from baseline to 12, 36, and 60 months. Time was used as a continuous variable, with a cubic trajectory, because the terms time2 and time3 were significant. For each linear mixed model, we included subject-specific random effects to consider the intra-subject correlation: a random intercept to consider the heterogeneity of the composite score at baseline and a random slope to consider the heterogeneity of the slopes between subjects. In the unadjusted linear mixed models, we included these fixed effects: intervention group by their amyloid blood status (8 categories), time, and interaction between group and time [4]. Then, to test the difference of the effect of the intervention between the negative and positive amyloid blood groups, we used the estimates of the interaction term parameters with the ESTIMATE command from the SAS MIXED procedure.
All the models were completed with and without adjustments for gender, age, educational level, CDR global score, and APOE ε4 genotype. All p values were presented before and after adjustment for multiple comparisons (using the Hochberg procedure) and the statistical significance was set at a P value < 0.05. All confidence intervals were two-sided with a 95% confidence level. All statistical analyses were achieved using SAS software version 9.4 (SAS Institute Inc, Cary, NC).
Standard protocol approvals, registrations, and patient consentsThe MAPT protocol is listed in a public-access clinical trial database (www.clinicaltrials.gov, no. NCT01513252). Written informed consent was given by all participants. A new informed consent form was signed by participants who volunteer for MAPT-PLUS during the end-of-study visit.
Data availabilityThe datasets generated and/or analyzed during this study are not publicly available. However, clinical data can be shared upon request following completion of the MAPT/DSA Data Access Application form (for further information contact the Data Sharing Alzheimer group: Info.u1027-dsa@inserm.fr).
Comments (0)