
Remember me
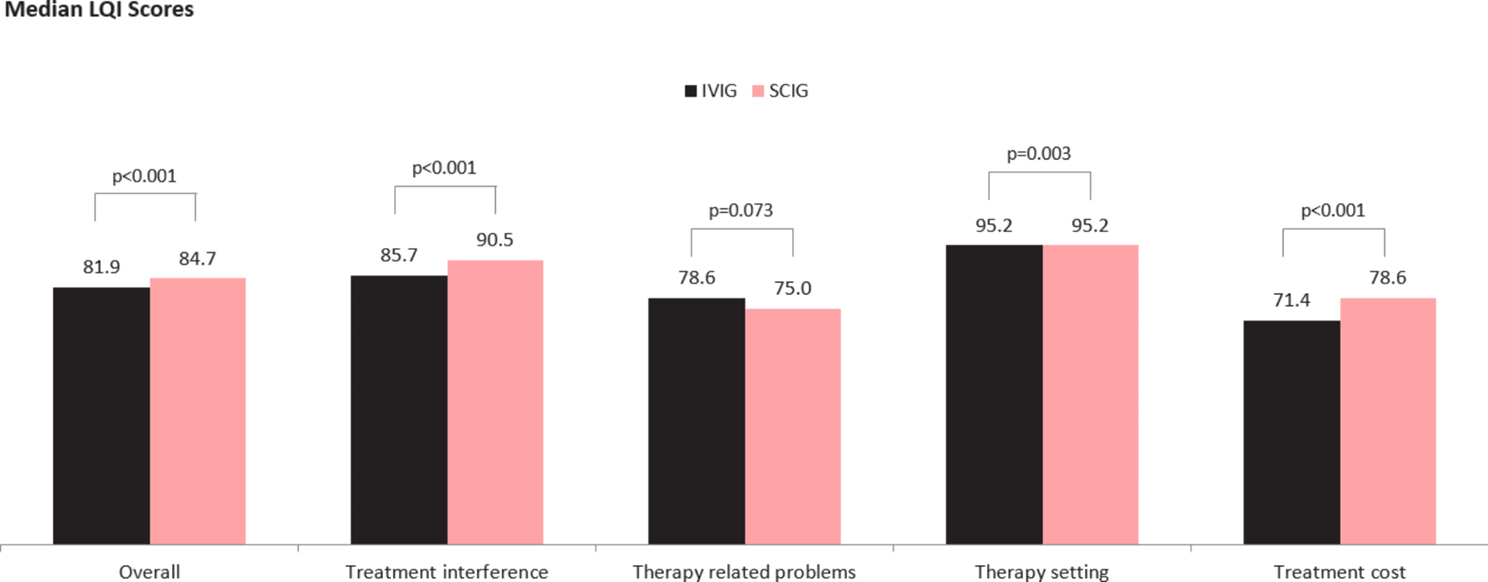







Table 1 summarizes the provincial guidelines on IG use in Canada. It includes information such as the version in use, year of release, organization committee, number of indications, availability of a dose calculator, presence of a home infusion program for SCIG, and the materials included in each guideline. The guidelines vary regarding the number of indications covered and the materials included. Except for Quebec, all provincial guidelines include an online dose calculator and a home infusion program for SCIG. Online IVIG dose calculators are available and use the same calculation as shown in the footnote of Table 1. The dose calculators are intended to be used when determining the dose of IVIG for clinically obese patients. The SCIG home infusion program is a valuable support system designed to assist patients undergoing SCIG therapy. It offers in-person training for patients, training partners, and caregivers, streamlines product ordering, and provides continuous case-management services [22]. The program is either administered and funded by provincial health services [22, 23] or pharmaceutical companies [24, 25].
Table 1 Summary of provincial guidelines on IG product use in CanadaThe recommendation categories also vary across the provinces (Table 2). The categories include "recommended"/"approved/recommended"/"do (accepted, effective)"/"indicated conditions" as Level 1, "not recommended for routine use"/"possible treatment option"/"possibly indicated conditions" as Level 2, "not recommended"/"do not do" as Level 3, and "insufficient data"/"do not know" as Level 4 in different provincial guidelines. In Table 3, we reported the number of indications in each medical specialty (dermatology, hematology, immunology, infectious disease, transplant medicine, neurology, and rheumatology) for each province and the percentage of indications that fall into each recommendation category. Overall, most indications for IG use in Ontario, Prairies, Atlantic, and Québec fall into the two categories with high uncertainty, Level 2 or Level 4, accounting for 43%, 38%, 59%, and 55%, respectively. British Columbia has the highest percentage of Level 1 "recommended" at 64% due to their two-level recommendation strategy, which includes only Level 1 and Level 3.
Table 2 Provincial IG guideline recommendation categoriesTable 3 Guideline comparison summary tableFigure 1 displays a forest plot from a meta-analysis that evaluates the recommendations for IVIG use across provincial guidelines, stratified by medical specialties. When ranked by the percentage of indications for which IVIG was recommended, the order from highest to lowest was immunology (72%), infectious disease (61%), hematology (50%), rheumatology (47%), transplant medicine (38%), dermatology (32%), and neurology (30%). However, significant heterogeneity measured by I2 was observed in the guidelines within the medical specialties. Among the 7 specialties, 5 specialties had an I2 greater than 50%: rheumatology (82%), transplant medicine (81%), immunology (78%), infectious disease (64%), and hematology (59%). Across all medical indications for all guidelines, the pooled percentage of the "recommended" indications was 47% (95% CI 38%, 59%), with a high overall heterogeneity of I2 = 73%.
Fig. 1
Forest plot for the proportions of the "recommended" medical indications under each medical specialty per provincial guidelines. #RCD: Number of "recommended" medical indications. Each red square represents the proportion of medical indications that fall in each provincial guideline's "recommended" category. The extending lines represent the 95% confidence intervals of the proportions. The black diamonds represent the pooled proportions calculated from the random-effects models for each medical specialty and all specialties
Scoping review of current literatureFigure 2 represents the study selection process. Our citation search yielded 1548 articles, of which 29 were eligible for review, including 22 journal articles and 7 conference abstracts (Table 4).
Fig. 2
PRISMA flow diagram for scoping review study selection
Table 4 Summary of included studiesIVIG utilization and trendThree studies investigated IVIG utilization, though in different contexts. Murphy et al. [17] focused on trends in IVIG use and the impact of provincial use mitigation strategies in a tertiary care center, Jutras et al. [26] investigated IVIG indications in a pediatric intensive care unit, and Hsia et al. [27] assessed the utilization of IVIG in patients with ITP and attempted to forecast future demand. These studies highlighted the rising trend in IVIG use. Murphy et al. [19] also revealed a slowed increase after implementing provincial use mitigation strategies. Both studies by Murphy and Jutras emphasized the limitations in the existing interventions and guidelines to control IVIG use, with the latter explicitly noting a high prevalence of off-label IVIG administration [26]. These findings suggest the need for reinforcement strategies, a better understanding of guideline adherence factors, and an exploration of alternative explanations for changes in IVIG use.
Audit of IVIG useShih et al. [9] and Liu et al. [28] examined IVIG use in different settings in Ontario. Shih et al. conducted a retrospective multicentre audit to understand the factors associated with increased IVIG use, while Liu et al. performed a hospital chart review of patients receiving IVIG for ITP. Both studies identified challenges in ensuring appropriate IVIG use. Shih et al. found low compliance with the Ontario IVIG Utilization Management Strategy and deficiencies in the completion of the IVIG Request Form, while Liu et al. observed that the use of IVIG for ITP was generally appropriate and carefully evaluated even in cases where the current provincial recommendations were not met. The studies concluded with recommendations for improving IVIG use, including a comprehensive, evidence-based active surveillance process and the development of clinical guidelines for IVIG use to ensure an appropriate and cost-effective treatment [9, 28].
More recently, Tran et al. [29] audited IG replacement therapy for SID at three hospitals in British Columbia. They evaluated the appropriateness of IG treatments against the Australian BloodSTAR Guidelines as a robust benchmark and showed that almost half (48%) of the study population had inappropriate IG replacement therapy. The most common reason was a lack of proper follow-up IgG levels at 6 or 12 months. Their data indicated a need for stringent guidelines to guide ordering practices [29]. Also, Shabani-Rad et al. [30] have developed and recommended a structured IVIG utilization program and comprehensive database in Alberta to manage and monitor IVIG utilization effectively. In collaboration with clinical disciplines, their review of registered patients labelled 85% of cases as appropriate.
Chronic IG therapy: from IVIG to SCIGBourque et al. [31], Alcantara et al. [32], and Suleman et al. [33] conducted retrospective cohort studies examining the use of SCIG in the treatment of myasthenia gravis (MG) and immune-mediated neurological disorders. Bourque et al. explored the use of SCIG in chronic inpatient MG management, observing a stable or improved MGFA (Myasthenia Gravis Foundation of America) clinical classification after SCIG initiation, with significant improvements in Myasthenia Gravis Activities of Daily Living (MG-ADL) profile and Myasthenia Gravis Quality-of-life (MG-QOL) [31]. Alcantara et al. studied the long-term effects of chronic immunoglobulin maintenance therapy (IVIG and/or SCIG) in MG treatment in-hospital, finding significant reductions in the number of immunosuppressive medications, prednisone and pyridostigmine doses with chronic IG treatment [32]. Finally, Suleman et al. examined the SCIG home infusion program for immune-mediated neurological disorders and reported high success rates in transitioning patients from IVIG to SCIG [33].
Cost saving analysis: from IVIG to SCIGTwo papers investigated the potential economic benefits of switching patients with PID/SID from IVIG to home-based SCIG therapy. Gerth et al. [34] used simulation modelling to estimate the impact on nursing time and cost savings. Switching a significant portion of patients from IVIG to SCIG could save 223.3 nurse FTEs (CAD$ 23.2 million in labour costs), potentially alleviating nurse shortages in Canada. Fu et al. [35] compared hospital and physician costs for patients receiving SCIG versus IVIG and found significantly lower average total costs for the SCIG group from the hospital's and physician's perspectives than the IVIG group.
Similarly, a comparative cost analysis by Ritchie et al. [36] between SCIG administration at home and IVIG in clinical settings showed that the self-administration of SCIG would save an average of $5386 per patient annually. Their results indicated that if 50% of patients who only received clinic-administered IVIG switched to self-administered SCIG during their study period, that would have saved $19.4 million for the Canadian healthcare system [36].
Patient satisfaction with IG therapyA survey study by Reid and Pires [37] on the experiences of patients and their preferences for IG treatment and their willingness to switch to a home-based program offered the home-based program as a potentially preferred option for patients with immune deficiency. Although patients mostly preferred IVIG over SCIG then, the loss of time and travel costs associated with hospital-based programs were considerable factors favouring home-based programs. Later on, Sholapur et al. [38] and Sultan et al. [39] investigated patient satisfaction with IVIG and SCIG treatments, respectively. Sholapur et al. evaluated IVIG's effectiveness and patient satisfaction as a treatment for ITP and found IVIG treatment to be perceived as inconvenient but satisfactory in terms of tolerability for ITP management [38]. Sultan et al. assessed the quality of life, treatment beliefs, and satisfaction among children with PID treated with SCIG. They reported that SCIG treatment was well-received by children and improved their quality of life. However, they also highlighted potential adverse effects, such as injection site reactions, which could affect treatment satisfaction [39].
In a recent report, Zhou et al. [40] studied patient satisfaction with IVIG treatment and their perceptions of SCIG for Inflammatory Myositis. They showed that while most patients were satisfied with the effectiveness of IVIG treatment, many found it inconvenient mainly due to its side effects. However, their willingness to switch to SCIG was low, possibly due to unfamiliarity with the treatment. Mallick et al. [41] surveyed the treatment satisfaction of adults receiving IVIG or SCIG for PID or SID. The patients receiving SCIG had spent significantly less infusion preparation time, actual infusion time, and post-infusion clean-up time per infusion than IVIG users. The SCIG recipients reported better treatment satisfaction than IVIG patients regarding perceived effectiveness. Patients who transitioned from IVIG to SCIG were overall satisfied with the experience, with many respondents reporting improved health-related quality of life, productivity, physical and mental health, and greater treatment satisfaction and compliance.
Efficacy and safety of SCIGSeveral studies evaluated the efficacy and safety of SCIG treatment. The study by Streu et al. [42] confirmed that SCIG treatment in patients with chronic lymphocytic leukemia (CLL) was not only effective but also resulted in significant cost savings, improved quality of life and treatment satisfaction. Similarly, in patients with MG exacerbation, a multicenter clinical trial in Alberta on the efficacy, safety and feasibility of 20% SCIG (Hizentra) indicated that SCIG was effective in treating mild to moderate exacerbations [43, 44]. Despite its large volume, SCIG appeared well tolerated at the standard IVIg dose with mild and rare local or systemic side effects [43].
Other studies focused on immune deficiencies in general. Walter et al. [45] showed that SCIG push (the administration of SCIG using butterfly needles and a syringe) to adults with PID was both effective (It significantly increased the serum IgG levels and effectively prevented infections compared to before treatment started) and well accepted by patients. A recent study by Keith et al. [46] evaluated the safety and patient satisfaction with 20% SCIG solution (Ig20Gly) in PID or SID patients after switching from other SCIG products. The patients under treatment with Ig20Gly maintained protective IgG levels against infections at 6 and 12 months after treatment initiation. Most adverse effects were generally mild to moderate and mainly included headaches or infusion-site reactions, and all patients expressed an interest in continuing Ig20Gly treatment [46]. Similarly, the research by Kobayashi et al. [47] suggested that Cutaquig (a 16.5% SCIG preparation) maintained efficacy and had mild and transient local and systemic adverse reaction rates in PID patients over four years of follow-up. Additionally, Brownlee et al. [48] also showed that Cutaquig could be an alternative treatment option for patients who could not tolerate the side effects of 20% SCIG products. They also reported no serious or severe adverse events while providing therapeutic levels of serum IgG in immunodeficient patients. Nonetheless, both IVIG and SCIG treatments in patients with SID are effective by reducing the number of infections and emergency department visits and improving patient perception of health compared to before treatment, as demonstrated by Abadeh et al. [49].
Alternative therapies for IVIGConsidering the cost and supply challenges related to IVIG and the associated side effects, including headache, aseptic meningitis, and allergic reactions, alternative treatment options have been considered for some of their medical indications. We found one study that compared the efficacy and safety of eltrombopag (a thrombopoietin receptor agonist indicated for chronic ITP) with those of IVIG. IVIG is commonly used to increase the platelet count before surgery for patients with ITP because it can induce a rapid and transient rise in the platelet count [50]. A study by Arnold et al. [50] showed that eltrombopag was non-inferior to IVIG for achieving and maintaining platelet count during the 7 day perioperative period. However, rare cases of serious side effects (pulmonary embolism and rebound thrombocytopenia) in the eltrombopag group suggested that the medication could be used as an alternative to IVIG for perioperative management of ITP, but with recommended attention to the risk of thrombosis and platelet count fluctuations. A follow-up study of patient-level data from the same trial was performed by Kaur et al. [51] to analyze the cost-effectiveness of the treatment from a Canadian public healthcare payer's perspective. The cost-effectiveness analysis indicated that eltrombopag was both more effective and less costly than IVIG, and perioperative eltrombopag saved an average of $413 Canadian per patient over the study period. Yet, a cost-minimization analysis by Furlan et al. [52] to compare IVIG with plasma exchange, two equally effective alternatives for treating patients with MG exacerbation, demonstrated that differences in cost-minimizing for treatments depend on different stakeholders' perspectives.
Comments (0)