In the course of food allergies, including hen's egg white protein allergy, typical gastrointestinal symptoms such as nausea, abdominal pain, and diarrhea are observed. These can be accompanied by complaints such as itchy skin, hives, conjunctivitis, oral mucositis, and rhinitis. Atypical symptoms, including headaches or difficulty concentrating, have also been recorded. In the course of severe forms of food allergy, anaphylactic shock may occur, posing an immediate threat to the patient's health and life [1, 8]. Sensitization to egg allergens mainly refers to sensitization to hen's egg white proteins (ovomucoid [Gal d1], which retains its allergenic activity despite heat treatment (with the exception of the baking process), ovoalbumin [Gal d2], which, along with ovotransferrin (Gal d3), is partially resistant to digestion and thermolabile, and lysozyme [Gal d4]). In contrast to the pediatric population, the allergy to hen's egg white in adults is considered to be persistent in nature while primary sensitization to hen's egg white is extremely rare [21].
Differential diagnosis of food allergies, including sensitization to hen's egg allergens
From the clinical point of view, it is important to properly identify the allergen so as to avoid it in the future and to appropriately treat any allergic reactions following accidental exposure. Due to the multitude of triggers and rich symptomatology, the diagnostics of food allergies, including sensitization to hen's egg white allergens, is a difficult and arduous process. The key elements in the diagnostics of hen's egg allergy include clinical history, skin tests, lab tests (sIgE/IgG4, BAT; CD63 and CD203c expression tests, component diagnosis, particularly in recurrent anaphylactic reactions) and/or elimination diets [1]. Double-blind placebo-controlled food challenge tests remain the gold standard. For safety reasons, however, these should only be administered within specialized centers under close medical supervision. Challenge tests are classified as either open or blinded challenges (single- and double-blind placebo-controlled challenges). Double-blind placebo-controlled food challenge (DBPCFC) is the gold standard in the diagnostics of food allergies. Thanks to its high sensitivity and specificity, it plays a key role in demonstrating cause-and-effect relationships between ingested food and clinical symptoms. Unlike open and elimination trials, the DBPCFC facilitates exclusion of the potential involvement of psychogenic factors. The test consists in randomized administration of the increasing doses of the verum, or the food suspected of causing disease symptoms, and of identical-looking and tasting placebo. However, when deciding on carrying out a challenge test, it is important that limitations of this are taken into account as being due to the possibility of developing anaphylaxis or another severe reaction, the possibility of false-negative and false-positive results, and the costs associated with performing the test in a hospital setting [22].
Practical implications of nasal allergen challenge
In our work, we present the results of a pioneering and unique study demonstrating the possibilities related to the use of NFC in the diagnostics of food allergies, with the possibility for objectivization of the course of the challenge offering a characteristic and important alternative to the food challenge test. To date, few research data were available on this subject in international literature [9,10,11,12].
According to the consensus statement of the EAACI Position paper on the standardization of nasal allergen challenges, indications for NAC in the diagnostics of allergies include demonstration of allergy to airborne allergens in the course of persistent, chronic, occupational, and local rhinitis, differential diagnosis of ocular symptoms, determination of causal relationship between the allergen and the symptoms, especially in the case of difficulties in interpretation of skin patch tests and sIgE levels, determination of indications for immunotherapy, determination of allergens directly responsible for the symptoms for the establishment of the composition of allergen vaccine, and monitoring of the efficacy of specific immunotherapy. Of particular note is a new indication related to the diagnostics and the possibilities for the use of NAC in food allergies [14]. Among the methods for diagnosing allergic diseases, NACs are characterized by high sensitivity and specificity rates. Positive challenge results are obtained in the group of patients with strongly positive skin prick test/sIgE determination results for conjunctival and NAC [23].
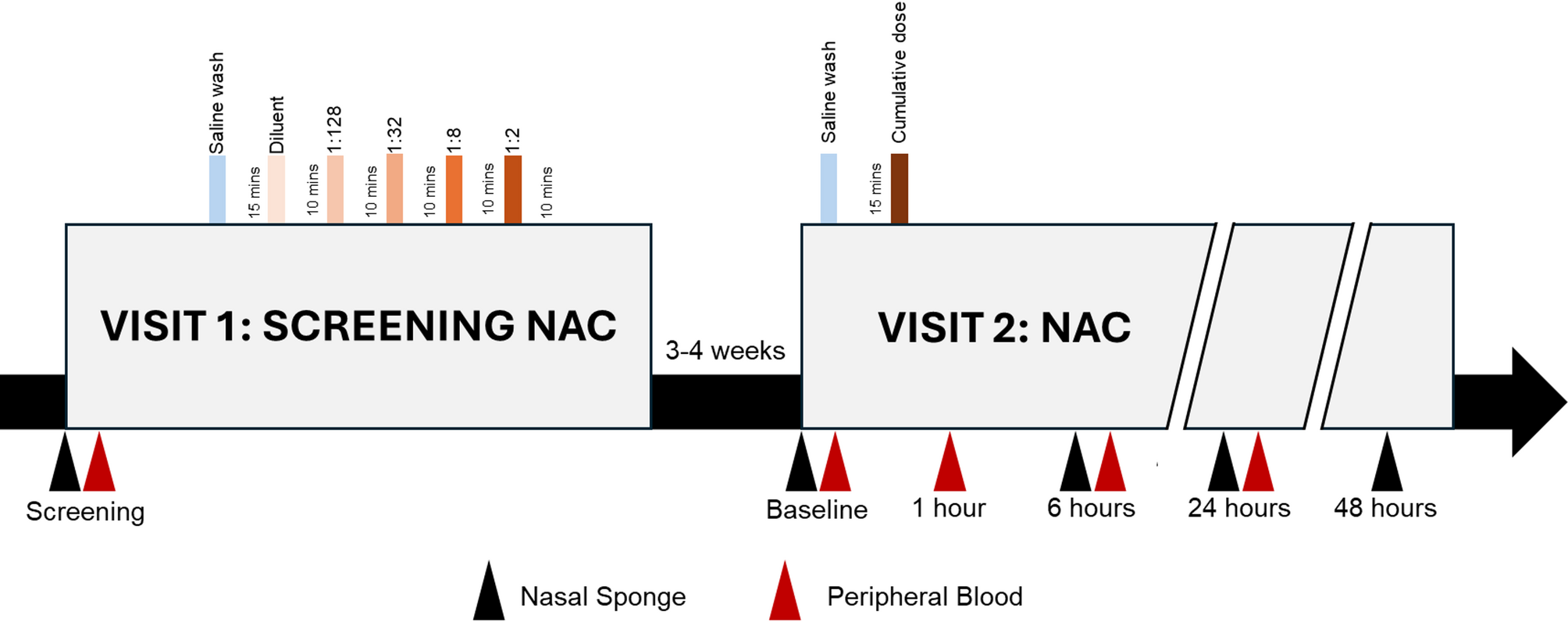
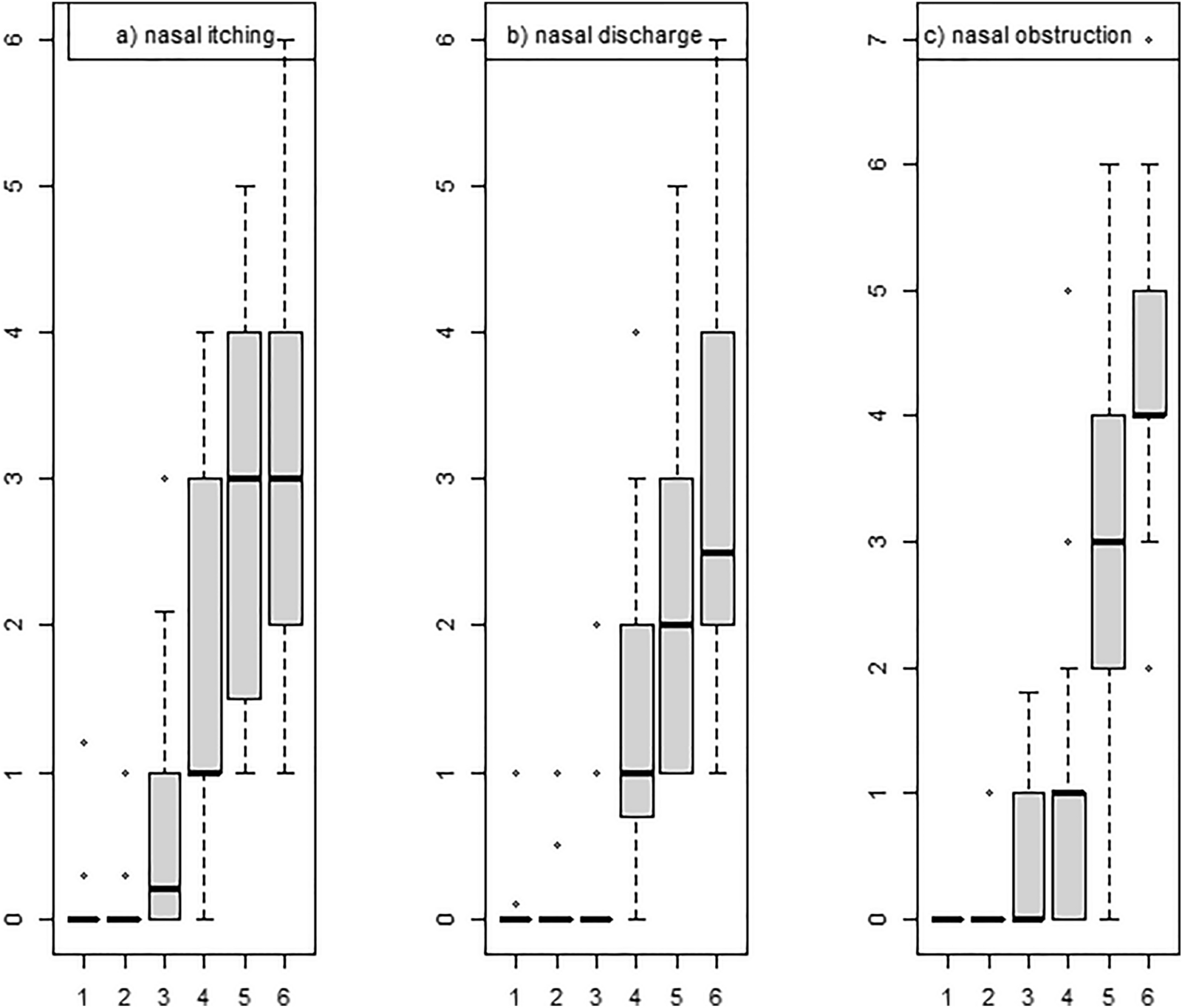
By implementing the NAC principle in NFC, convenient conditions can be established for the objectivization of the diagnostic method. The course of NFC is typical for NAC and involves observation of nasal symptoms such as nasal itching, nasal discharge, and nasal obstruction in the early and late phases of the allergic reaction. The implemented test design, including the scales used to assess subjective complaints and the objective techniques, facilitates the assessment of the degree of the response of nasal mucosa to local allergen application. The NFC is in its nature a titration test and, appropriately to the allergen being tested, the degree of response is assessed using objective techniques and subjective scales at 15-min intervals. The selection of objective methods for the assessment of nasal patency in NFC may vary, consisting mainly of acoustic rhinometry [12] and computed thermography [9, 10]. A study by Gelis et al. involving NFC with seafood allergens revealed significantly significant decreases in nasal cavity cross sections. Similarly, Clark et al. demonstrated temperature differences within the nasal cavity area during the early phase of the allergic reaction following intranasal provocation with peanut allergens [10, 12]. Both studies revealed outstandingly positive outcomes of the challenge tests, warranting the possible use of this test method in the diagnostics of FA. In our study, optical rhinometry, directly illustrating quantitative changes in nasal patency as expressed by means of optical density, was used to assess objective changes in nasal patency. Unlike other techniques, such as acoustic rhinometry or rhinomanometry, OR does not require complex mathematical operations since the device delivers the final result as the change in patency of nasal cavity expressed in ΔE; in our case, the difference was 0.34 OD. Thus, one may conclude that the mucosal response in this particular case was 34%. In addition, the course of the early phase of the NFC was typical for NAC and was characterized by a slight increase in sIgE levels in the lavage fluid, showing the involvement of an IgE-dependent response in NFC. Most reports documenting the clinical significance of sIgE/tryptase levels in nasal lavage fluid relate to local rhinitis and occupational airway allergy [24,25,26,27].
Only the titratable nature of NFC was described in current art [10, 12], and the acquisition of lyophilizate for testing is carried out under laboratory conditions thus being restricted for scientific purposes. Our study, with a moderately positive response being recorded to the topically applied egg white allergen, contributes to the establishment of an appropriate environment for further research in the future, particularly in the area of allergen form and dose standardization so as to objectivize the cut-off for positive challenge tests. Importantly, the changes observed in the course of NFC are limited to the nasal cavity with only occasional systemic manifestations, thus confirming the method's high safety profile in contrast to oral food samples. Absolute contraindications [12] and appropriate preparation for the test, including an elimination diet just as in the case of oral food challenge, are important criteria to be taken into account when qualifying patients for NFC [20].
Limitation of study
A specific limitation of the present study is related to the ability to assess the safety of the test due to the existing contraindications, including, as previously mentioned, the exclusion of patients with a history of anaphylactic shock [13, 14, 16]. A significant limitation of the study is the need to exclude patients diagnosed with allergic rhinitis from the study group. Another major limitation of the study consisted in the lack of a reference point for the nasal mucosal response to the oral hen's egg white allergen challenge test as carried out on the study group.





Comments (0)