
Remember me
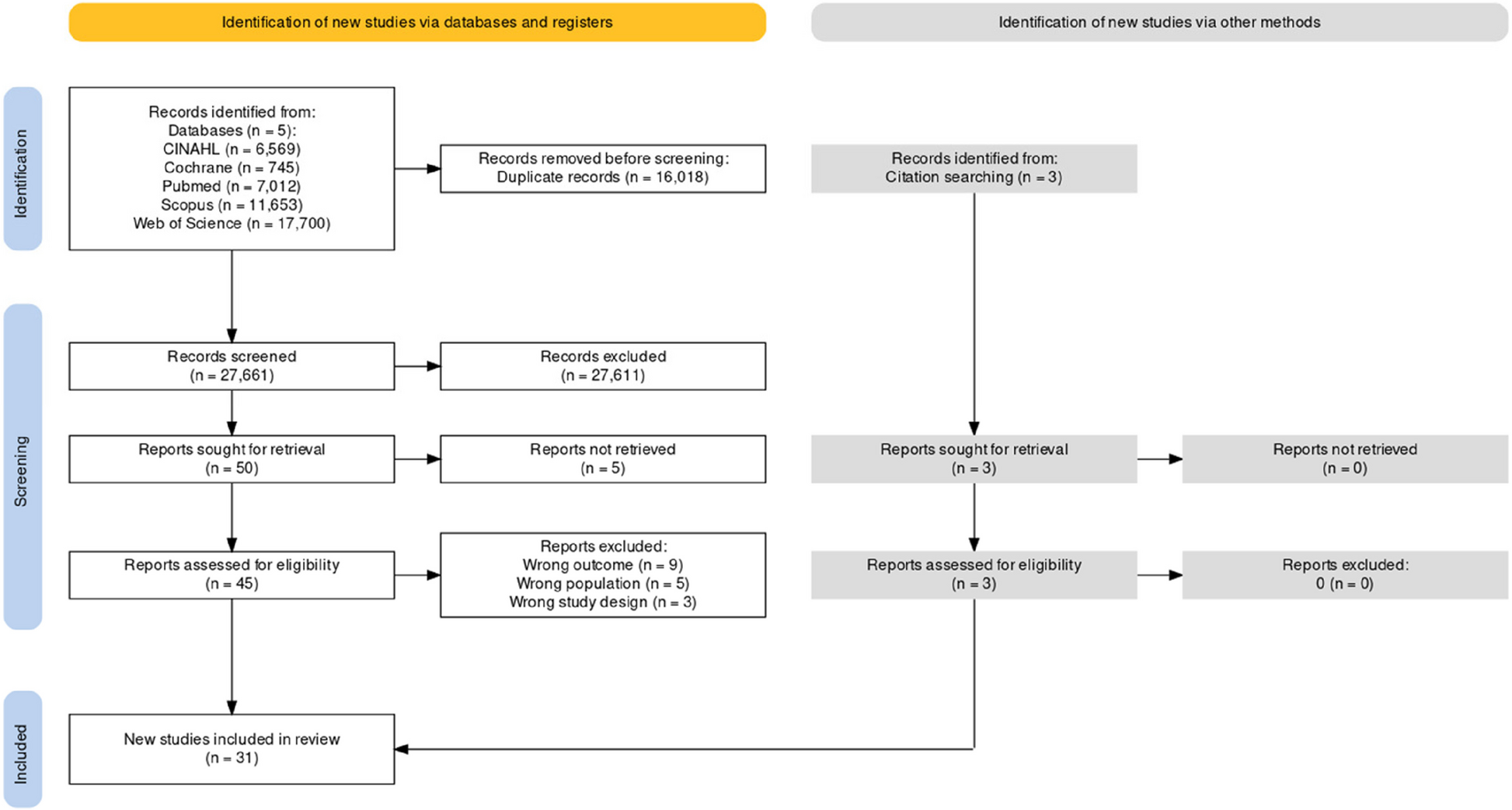
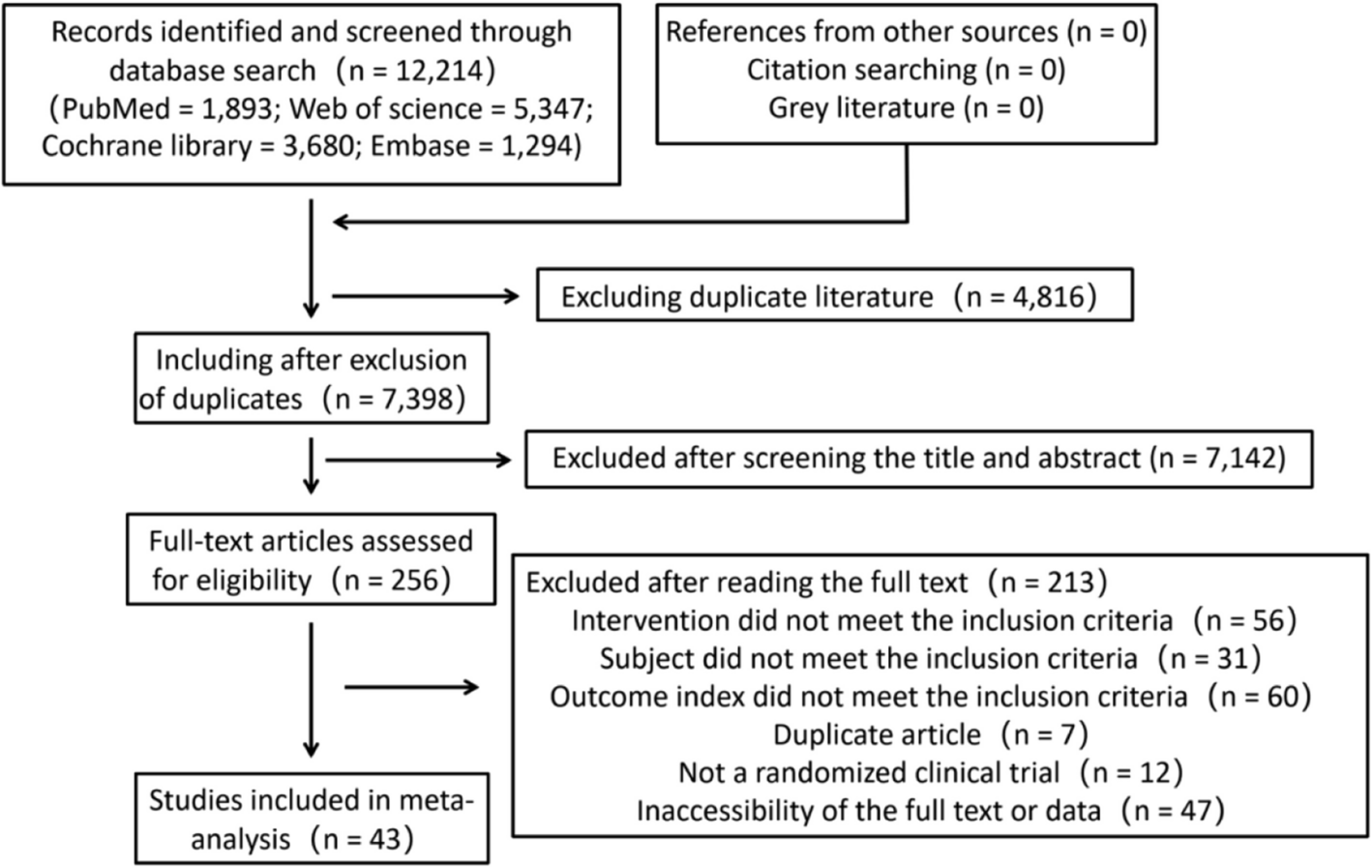
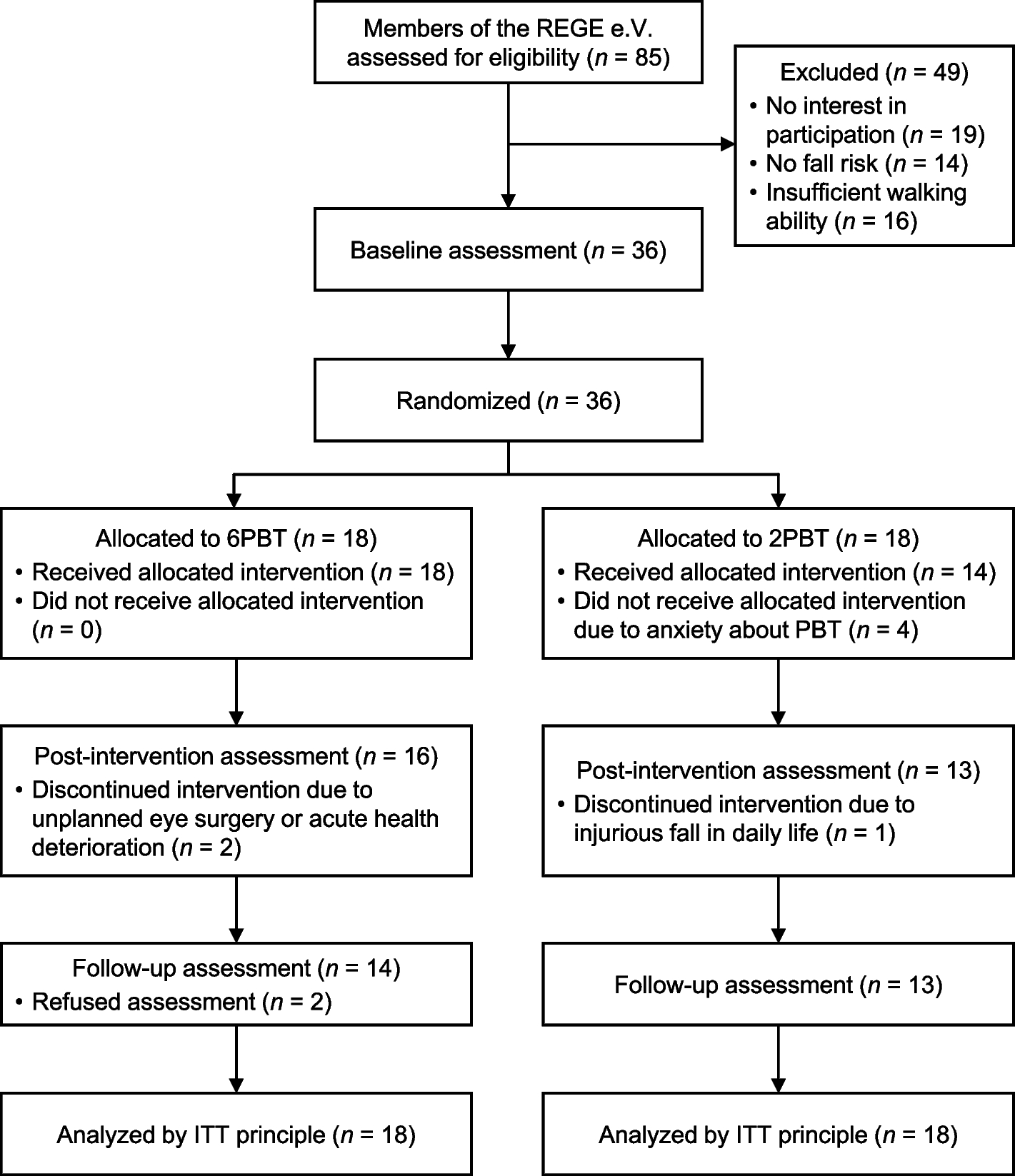




The search yielded 921 records. Using citation tracking, 14 additional publications were added to the search. Duplicates were removed and the remaining titles and abstracts were screened against the defined criteria, leaving 73 records for full-text review. 51 articles that did not meet the inclusion criteria were excluded during the full-text review, so the review includes a total of 22 studies. The reasons for study exclusion are explained in the PRISMA flow diagram (Fig. 1).
Fig. 1 Study characteristic
Study characteristicThe 22 studies have been published between 1981 [20] and 2022 [21, 22], whereby most studies were published after 2010 (n = 11). Prior to 2010, studies were conducted only in Finland (n = 1), France (n = 1), the UK (n = 4), and the USA (n = 5), the newer studies were done in Australia (n = 1), Germany (n = 7), Switzerland (n = 1), UK (n = 1), and USA (n = 1). Most of the studies (n = 15) were conducted with a quantitative design. Studies with qualitative design (n = 3) and case reports (n = 4) were carried out in Germany, Switzerland, and the USA. A total of 6311 individuals have been included in the studies, although not all persons were affected by a long lie. 2805 people were unable to get up from the floor and 1121 people were affected by a long lie, whereby the researchers had different definitions and thresholds of a long lie, so it cannot be assumed that the people spent the same amount of time on the ground (Table 2). Of the seven studies conducted in Germany, a rather small number of 102 participants were examined, whereby the study from Schwickert et al. [23] is not included, because they only reported falls and it is not apparent how many people were involved in the falls (n = 34 falls with delayed recovery). The researchers of the study conducted in Switzerland interviewed experts on the treatment of long lies [24].
Table 2 Summary of relevant studies (N = 22)Study qualityTwo independent reviewers have conducted the study quality appraisal following the Standard Quality Assessment Criteria by Kmet et al. [20]. The score sheet for qualitative studies consists of ten items, and the one for quantitative studies has fourteen items. As each investigator could rate the items with a maximum of two points, the single items could score with a maximum of four points (2 reviewers × 2 points).
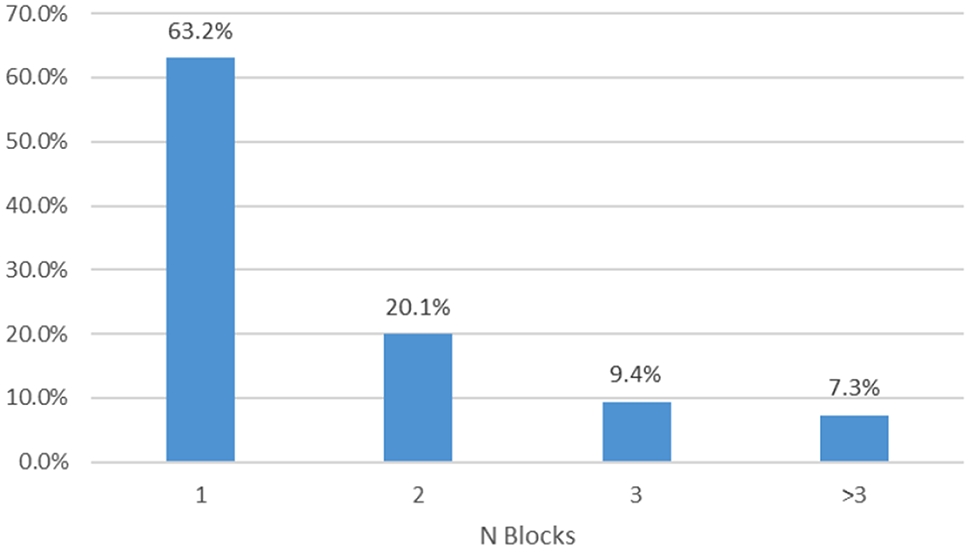
The quantitative studies rate better with a mean score of 81.3% than the qualitative studies with a mean score of 50% (Fig. 2). The qualitative studies are rated lower because the four case descriptions in particular only described their methodological procedure inadequately, which means that the item data collection is rated 0.9 and the item´s data analysis and verification of data is 0.7 each. The quantitative studies are limited especially because the sample size is not appropriate (2.6) and there is a missing variance in the reporting of results (2.6). Furthermore, all quantitative studies do not use randomizing or blinding interventions (an overview of all items can be found in Additional file 1: Appendix 2 and 3).
Fig. 2
Quality assessments results for qualitative and quantitative studies according to the Standard Quality Assessment Criteria [19]. The qualitative studies could reach a maximum score of 40 points (2 reviewers × 10 items × 2 points), the quantitative studies of 44 points (2 reviewers × 14 items × 2 points – (2 reviewers × 3 items × 2 points)). The results are presented as a percentage of the maximum scores
Use of the term long lieThe term “long lie” is most frequently used in the context of emergency care in seven studies [21, 22, 24, 26, 29, 31, 33]. The studies primarily focused on the acute treatment of a long lie, for which they surveyed the characteristic attributes of the incidence. The characteristics of long lie were also studied in the context of nursing [34], geriatrics [23], and public health [36, 39]. In addition to the characteristics, the prevalence of long lie was surveyed. This subject was pointed out in studies conducted by authors in the disciplines of nursing [28], rehabilitative medicine [27], and public health [30]. Often, long lies have been measured as a secondary outcome to identify the consequences of a fall [20, 40, 41]. Furthermore, authors in studies in public health examined the ambulance service [37, 38], and researchers in psychotherapy focused on two studies the stand-up strategies of persons in the context of fall management [25, 35].
In total, authors in two studies in the field of nursing [28, 34], two studies in the discipline of geriatrics [20, 23], three studies in rehabilitative medicine [27, 32, 40], and six studies in public health [30, 36,37,38,39, 41] described a long lie.
Characteristics of the term long lieCauses and associated factorsThe risk of suffering a long lie increases significantly with age [25,26,27,28,29,30, 38,39,40]. Older adults who are affected are more often women [21, 27, 30, 35, 37], persons younger than 65 are mostly men [21, 29, 30], usually socially isolated [29, 31] and more often found dead [30, 31].
Older adults suffered falls [19,20,21, 23,24,25,26,27,28, 30, 32,33,34,35,36,37,38,39,40,41], but it has been the frailty of the individuals that affected their inability to get up after the fall [22,23,24,25,26,27,28, 30, 33,34,35,36, 39]. Older adults are characterized mainly by balance and mobility problems [27, 28, 36, 39], they have generally a longer disease duration with poor health [27, 29], and are dependent on others for help with activities of daily living [39]. Two studies have also indicated that the affected persons often suffer from a cognitive or mental illness [28, 29]. Schwickert et al. found that persons who take longer than 25 s to recover after a fall are often unable to get up by themselves [23].
Besides the fall, a long lie can also be initiated by immobilization caused by serious acute or chronic injuries [21, 24, 29, 30, 36, 39], neurological events with loss of consciousness [21, 24], infection with increased body temperature [21, 36], domestic trauma [21], low serum potassium concentration [36], intoxication [21, 24, 30], or suicide attempts [30].
In addition to the biological and social causes, the duration of the long lie depends on whether the persons have active social relationships [29,30,31] and how much time a day they spend alone in their own rooms [30, 39].
ConsequencesAuthors in three studies reported in detail which acute biological consequences occur after a long lie [21, 29, 30]. These symptoms are confirmed by further studies. Hypothermia [21, 22, 24,
Comments (0)