1. IntroductionThe formation of biofilm is a major pathogenic mechanism that results in antibiotic tolerant infections. This is particularly true for patients with medical implants such as catheters [
1], cardiac pacemakers [
2], prosthetic joints [
3], dentures [
4] prosthetic heart valves [
5], implanted lenses [
6], cerebrospinal fluid shunts [
7], intrauterine devices [
8], breast implants [
9], biliary tract stents [
10], vascular prostheses [
11], penile prosthesis [
12], left ventricular assist devices (LVADs) [
13], trauma hardware [
14] and voice prostheses [
15]. Foreign bodies provide a suitable environment for attachment and growth of biofilm that leads to reduced sensitivity to antimicrobial agents as well as the host’s own immune response. As such, approximately 50% of nosocomial infections are associated with indwelling devices [
16]. Biofilm infections can also form on tissue surfaces unrelated to foreign bodies, such as in patients with cystic fibrosis and COPD [
17,
18], native valve endocarditis [
19], chronic sinusitis [
20], and chronic (diabetic) wound infections [
21].Once formed, treatment strategies vary, but it is generally agreed that in biofilm-related implant infections, definitive treatment will usually involve surgical removal and replacement of the implant. Depending on the type of implant and risk of surgery for the patient, pharmacological treatment alone may be warranted [
22]. Yet, the minimum inhibitory concentration for biofilms (MICB) and minimum bactericidal concentration (MBC) of antimicrobial therapy needed to penetrate a biofilm can be difficult to achieve in vivo due to toxicities and side effects incurred at such high drug concentrations [
23]. Early biofilms can be treated with an antibiotic regimen alone but can be hard to detect due to the lower sensitivity of routine microbiological examinations for these localized aggregates of bacteria; oftentimes multiple biopsies or proper sonication of the suspected infected area are required to detect the pathogen. These barriers to diagnosis are one reason biofilm is not caught in time for antibiotics alone to be effective [
19].In the United States, revision arthroplasty of an infected joint requires a two-stage revision: removal of the infected apparatus and debridement of infected tissue, and temporary joint fixation for 6–12 weeks while antibiotic treatment is completed. Surgery is then needed to implant a new prosthetic joint. This method, while effective in removing biofilm, has proved to be costly and arduous, oftentimes with a failure rate of up to 22% [
24,
25]. Most risk factors for failure are those which would not be modifiable for patients, eliciting the need to improve current treatment protocols and options [
26]. Multiple surgeries in conjunction with prolonged antibiotic regimens increase the cost of therapy for affected patients [
27]. The total projected cost of treating prosthetic joint infections (PJIs) annually in 2030 in the United States will be about $1.85 billion, including $753.4 million for total hip arthroplasty and $1.1 billion for total knee arthroplasty [
28].While the topic of biofilm prevention and removal is one of importance in many areas of clinical medicine, this review will largely cover its place in the treatment of PJI through physical or non-pharmacological methods. Such methods have a long history of use in industrial settings and commonly utilize heat, light, sound, or electromagnetic energy. These methods can potentially be translated to treatment of biofilms on implants within the human body, but so far have remained in developmental stages for treatments of PJI. A recent review summarized novel biological and physiochemical methods of synergistic anti-adhesion composition and antibacterial agents [
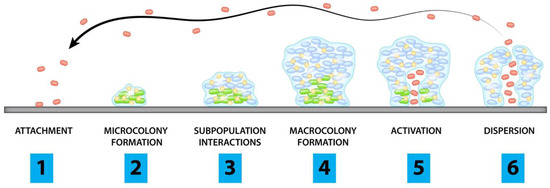
29]. This review will focus on novel methods of the physical strategies for biofilm disruption and provides a unified summary of the progress that has been made and the challenges that remain. 2. Pathogenesis of BiofilmsIn response to a hostile environment, bacteria (and sometimes fungi) form a structure consisting of cells adherent to each other and the foreign surface, surrounded by a self-produced extracellular matrix. This occurs in stages: initially, the planktonic form of the microbial cells will attach to a surface and form microcolonies. They will then form a young biofilm, which differentiates into a structured mature biofilm and will eventually disperse once activated when under stressful conditions (
Figure 1) [
30].
Stages of biofilm formation:
Planktonic cells attach to surface of concern
Cells begin to form microcolonies
Interactions between subpopulations form microstructures and protective layers
Biofilm matures and forms microcolonies
Channels form and allow for accumulation of cells
Planktonic cells are released from microcolonies
Red dots represent individual planktonic cells while green dots represent biofilm embedded bacteria with blue dots showing protective microstructures
In order to begin adhesion, bacteria secrete extracellular polymeric substances (EPS) consisting of extracellular DNA, proteins, lipids, amyloid fibrils, and polysaccharides such as the polysaccharide intercellular adhesin (PIA) known as poly-B(1-6)-N-acetylglucosamine (PNAG) in Staphylococcus spp. [
31]. As bacteria form microcolonies, a hydrogel layer forms that creates a protective barrier between the community and the extracellular environment. The mature biofilm stage is reached as bacteria continue to accumulate into layers of macrocolonies surrounded by channels that help to distribute nutrients and signaling molecules [
32] throughout the structure.Bacteria use quorum sensing (QS) to coordinate gene expression according to their density which functions to regulate the production of virulence factors and create systemic infection. For example, in S. aureus, the Spx protein (global regulator of stress response genes) induces expression of the locus (icaR) which negatively regulates the locus for polysaccharide intercellular adhesin (PIA) and icaA (whose product is an N-acetylglucosaminyltransferase that synthesizes PIA oligomers), whereas the Rbf protein (protein regulator of biofilm formation) inhibits icaR, allowing for expression of icaADBC, a locus that regulates PIA expression [
33]. In studies of other bacterial species, inhibition of QS receptors such as LasR and Rh1R has provided bacterial hosts with protective effects from biofilm-producing bacteria and reduced QS related virulence during biofilm treatment. Inhibition of the Rh1R target protected human lung epithelial cells from quorum sensing mediated killing by Pseudomonas aeruginosa due to treatment with meta-bromo-thiolactone [
34]. RNAIII-inhibiting peptide treatment in rats has been found to strongly prevent methicillin resistant S. aureus graft infections, indicating the contribution of QS in biofilm formation [
35].Several mechanisms contribute to the antimicrobial resistance of biofilms including low metabolism of antimicrobial agents by cells in the biofilm matrix, presence of persistent dormant cells, and small, highly resistant variant colonies. Stress adaptive responses of the bacterial cells in the biofilm may lead to delayed drug penetration or slow cell growth, to changes in the chemical microenvironment within the biofilm, and to up-regulation of drug resistance genes [
36]. Though many strategies related to overcoming biofilm drug resistance mechanisms from a pharmaceutical standpoint have been studied, methods utilizing physical energy have been proposed as alternative solutions. Some have shown promise in either destroying biofilms directly or modifying them to allow for improved effectiveness of pharmaceutical agents. 4. Intrinsic Methods
Approaches to intrinsic biofilm prevention can be grouped into a number of strategies that make use of implant modification to prevent or limit biofilm formation. These strategies include co-implantation of an antibiotic reservoir, nanolayer coating of the implant and varying the implant material. These approaches can further be combined such as by varying both material and nanocoating of an implant or by incorporating antibiotics within or in combination with a nanocoating.
Multiple factors, such as surface roughness, may encourage or discourage colonization [
24]. For instance, if the roughness profile approaches the size of an individual bacterium (1 µm) it can encourage colonization, while surface pores close to the size of osteoblasts can inhibit colonization. Implant surface porosity can influence fluid flow at the implant surface while high surface hydrophobicity and low surface free energy can also inhibit colonization.The use of different materials during the revision process presents an opportunity to combat biofilm. Historically, bone cement has typically included antimicrobials as additives to discourage biofilm formation. However, the number of strains of S. aureus and S. epidermidis resistant to the normally utilized gentamicin and tobramycin is rising. In one study, resistance to gentamicin was 41% and tobramycin 66% [
37]. Additionally, implanting a reservoir of antibiotic-loaded bone cement (polymethylmethacrylate, PMMA) is not conclusively proven to ward off infection and can instead create drug-resistant bacteria through prolonged presence of sub-therapeutic concentrations of antibiotic in intra-articular spaces [
38]. However, due largely to retrospective case reviews, new material-based strategies are being devised. These include increasing porosity and improving elution profiles of PMMA through modification of its mixing process, using binding agents to increase elution, and using newer antibiotics with longer half-life [
24].Alternative biomaterials to PMMA constitute a possible avenue of exploration but have so far yielded no promising clinical data. Calcium sulfate-loaded, radiopaque beads demonstrated equivalent or better elution characteristics than PMMA, and when impregnated with tobramycin and/or vancomycin were able to reduce S. aureus biofilm formation, though they did not reduce biofilms that had already formed [
39,
40]. Unfortunately, clinical studies using calcium sulfate beads have detailed hypersensitivity reactions in response to the beads, which are not approved for use in the US [
24]. Bioactive glass and biocomposites, such as Septacin, a polyanhydride loaded with gentamicin, are considered as biodegradable alternatives [
41]. However, these resorbable materials have in general are not validated in clinical studies and cannot keep pace with the growth of surrounding bone, limiting the length of time they provide protection.A simulation of copper and multi-walled carbon nanotubes by Seo et al. [
42] showed some success based on stochastic response that predicted the efficiency of synthesizing nanostructures against Methylobacterium spp. The nanostructures increased antimicrobial activity against biofilm in this simulation without increasing toxicity to human cells by damaging the cell wall, causing secondary oxidation of ROS, and releasing copper ions.Nanoparticles are also a potential source of novel coatings that can be used to prevent biofilm formation. In a study by Gulati et al., titanium nanotube (TNT) arrays loaded with gentamicin were adsorbed to titanium wire by electrochemical anodization. The TNT arrays exhibited a two-phase release of gentamicin, with an initial burst release (37% of weight) followed by a slow release with zero order kinetics over 11 days (Gulati et al. [
43]. While the release dynamics of the TNT arrays were observed alone, these nanostructures could potentially be studied within the format of a bone fixative tool or as part of a bone implant assembly. This method shows some promise as an alternative to conventional implants with an added drug eluting component that could prevent biofilm formation and infection.Silver nanoparticle coatings are one of the most commonly used non-antibiotic antibacterial coatings due to the tendency of silver to leach from the coating and diffuse into bacterial cells resulting in damage to enzymes [
44,
45,
46,
47,
48,
49,
50,
51]. This nanomaterial has been implemented in a number of ways, including incorporation into hydroxyapatite and chitosan to promote osseointegration, and combined with titanium dioxide to make an anticorrosive material coatings [
24]. However, most of these methods are yet to be tested clinically, so potential systemic effects remain unconfirmed [
45].In a study by Zaatreh et al. [
52], the viability of a rapidly degrading layer of magnesium on titanium was tested in a co-culture model of S. epidermidis and human osteoblasts (hOBs) to verify the antimicrobial and biocompatible properties of the magnesium. When compared to bare titanium Ti6Al4V discs, samples coated with pure magnesium showed an increase in viable hOBs by ~20,000 cells/mL following 7 days of culture. Samples also demonstrated significant bactericidal effect as shown in the reduction of biofilm population by four orders of magnitude after seven days. This study demonstrated the interaction between the implant surface, human tissue, and biofilm and provided an important next step in the development of a potential implant coating that could help prevent and fight biofilm in the short term.Other coatings have also provided a potential method to prevent or treat biofilm formation, and several approaches including polymers, hydrogels, cyclodextrin, and hydroxyapatite have been tested as drug delivery methods to infection sites [
24]. The use of affinity polymers such as cyclodextrin were explored in hernia meshes, vascular grafts, and stents; their utility in orthopedics is better demonstrated when functionalized to hydroxyapatite with extended-release capabilities and osteoblastic cytocompatibility when loaded with tobramycin, rifampicin, gentamicin, ciprofloxacin, vancomycin, or some combination of these antibiotics [
53,
54,
55].Researchers have also explored polymers that can be refilled with chosen antibiotics rather than preloading a polymer with antibiotics prior to surgical placement [
56]. Cyphert et al. designed a polymerized cyclodextrin (pCD) incorporating specific drug affinity that can be placed at the time of surgery and later injected with antibiotics as needed should the patient develop infection. The pCD has hydrophobic inner pockets that take advantage of the affinity interaction with the drug to form a reversible inclusion complex and allow for in situ antibiotic refill and release. In this in vitro experiment, Cyphert et al. utilized rifampicin and minocycline which have relatively high binding energies with β-cyclodextrin and were able to maintain a steady concentration gradient from an agarose tissue phantom into implanted polymer disks. Rifampicin and minocycline were previously shown to be released gradually from a polymerized cyclodextrin that maintains its mechanical integrity under physiological conditions [
57]. In the presence of S. aureus immature and mature biofilms, the pCD disks were able to be filled with rifampicin and minocycline and showed no statistical difference in affinity and filling when compared to control disks without biofilm formation. Moreover, as rifampicin filling time was increased, after two days the majority of bacteria in a mature biofilm had been eradicated [
56]. In the future, this polymer could be formulated as a device coating or formed into nanoparticles to provide a local drug sink that can overcome the delivery issues that reduce the effectiveness of systemic antibiotics in biofilm treatment efforts. Though earlier work has already demonstrated that pre-filled polymers loaded with vancomycin can adequately treat mesh infection in rodents and MRSA hernia defect infections in pigs [
58,
59], the refillable functions of this polymer have the attraction of individualizing antibiotic treatment to just those who present with infection and can be specific to the bacteria infecting the implant. An area of future study may include the affinity polymer’s ability to be refilled with vancomycin, gentamicin, and other drugs typically utilized to target the tolerant bacteria that so often make up biofilms in PJI. Additionally, though this method is being developed to target hernia mesh infections, its utility for treatment of joint implants in situ will also require additional exploration to determine the ability to reload the polymer once set into a joint environment as well as the polymer’s interaction with the surrounding tissue.Min et al. [
60] proposed a novel method in their development of an implant coated with gentamicin and bone morphogenetic protein 2 (BMP-2) in layers using nanofabrication technology to create conformal nanoscale coatings in a layer-by-layer (LbL) fashion. This LbL assembly facilitated high drug loading while its nanometer to micron scale features allowed for fine tune of multidrug release kinetics at biologically relevant times. This design created a biofilm free environment that encouraged bone growth and repair. The authors demonstrated the capability for antimicrobials to be released over several weeks, while the BMP-2 in underlying layers was sustained longer term, resulting in better bone formation. This specially coated implant was then tested in osteomyelitis-induced mouse models and analyzed by micro-CT. Results revealed that the implants integrated well into bone and showed quantifiable differences in intra-osseous bacterial survival and bone remodeling [
60]. Clinical implementation of this technique would allow for a one stage revision rather than the current gold standard of two stage revision, reducing time and costs associated with the lengthy procedure. The success of this implant coating in mouse models may suggest its potential for success in similar layering of artificial heart valves and vascular grafts and could potentially form the basis for a wide variety of coatings in clinical applications.Another option for coatings is the novel approach taken by Williams et al. [
61] in formulating a silicone (polydimethylsiloxane or PDMS) polymer with an active release antimicrobial agent called cationic steroid antimicrobial 13 (CSA-13). CSA-13 is a synthetic analog of naturally occurring antimicrobial peptides. Because it is not a peptide, it is not a target for proteases. The positively charged components of CSA-13 interacted with negatively charged components of bacterial cell membranes, causing membrane disruption and the release of cytoplasmic components [
62]. CSA-13 was found to have superior performance over antibiotics and antimicrobial peptides, a longer shelf life and lower cost of production with a broad spectrum of activity and nonspecific method of attack on bacterial cell membranes [
61]. Further studies in sheep models with simulated Type IIIB open fractures and mature biofilm inocula demonstrated that CSA-13 reduced the number of bacteria in biofilms to a level that could be addressed by the host immune system. CSA-13 was also found to elute into surrounding tissues and fluids to prevent biofilm-associated osteomyelitis [
61,
63]. Further sheep modeling in which animals received porous coated titanium implants in the right femoral condyle demonstrated that subjects that received the CSA-13 coated implant prior to a 5 × 108 CFU inoculum of MRSA had no evidence of bacterial infection. In addition, bone growth at the end of 12 weeks was consistent with control subjects that received a non-coated implant and no MRSA inoculum [
64]. Williams et al. [
65] then utilized their CSA-13 coating against Pseudomonas aeruginosa and found an 8 log10 reduction in CFU in less than 24 h in a flow cell system. Because these methods focused on treatment of biofilm as opposed to planktonic bacteria, they were not limited by specific MIC guidelines largely developed based on antimicrobial concentrations for planktonic bacteria that would not necessarily translate to biofilm efficacy. In this case, a potentially intrinsic method has shown to be possible not only in preventing biofilm infection, but also in actively treating existing biofilms. Unfortunately, CSA-13 technologies were abandoned with no clinical data, yet N8 Medical licensed other compounds within the same class are being incorporated into Cerashield™ endotracheal tubes and Health Canada granted emergency request use in mechanically ventilated COVID-19 patients.Williams et al. synthesized a separate class of antibiofilm compounds called CZs (nomenclature based on a company name; Curza) with dual potential to disperse, kill bacteria, and destroy biofilms. Early work shows that CZs can likewise be incorporated into thin film, active release coatings to treat and prevent biofilm implant-related [
66,
67]. These coating types constitute a significant development in the treatment of biofilm on implants.A multi-disciplinary biomedical engineering approach was taken by Ehrlich et al. [
68] to construct a “smart” novel implant that would prevent biofilm formation. Their approach employed newer technologies that could exploit quorum sensing and had built in antibiotic release. Here, “surveillance” of quorum sensing would in effect “eavesdrop” on the bacteria as they produce intercellular signaling molecules that coordinate metabolic switching and toxin production related to local bacterial burden. In this approach, a microelectromechanical system (MEMS) biosensor sends a signal to a pair of integral gated receptors in response to changes in viscosity resulting from increased concentrations of glucose that occur due to activation of quorum sensing by the bacteria as signified by the production of these intercellular molecules. The receptors then release inhibitory compounds and antibiotics at very high local concentrations. The biosensor and drug reservoir would be connected to a telemetry system accessible to both patient and physician enabling readings of existing conditions on the implant surface. Additionally, the study explored the use of the bioelectric effect in treating PJI with the exposure of biofilm to AC or DC current in the presence of antibiotics. This “smart” implant design shows much potential, yet it is largely untested and would require the support of a manufacturer willing to undergo the prototyping process to develop it for practical use. However, interest in this novel system may be indicative of future design trends that harness the microenvironment inherent to the implant interface itself to prevent the formation of biofilms. Conclusions for Intrinsic MethodsA summary of intrinsic methods is provided in
Table 1. Questions remain about the implementation of intrinsic methods for biofilm prevention and control. For implants with new coatings, there remains the possibility of damage to neighboring host cells as well as endotoxin release that can follow the death of large amounts of bacteria [
62]. Yet, we recognize infection is likewise cytotoxic; a balance must be achieved. We found that in most novel intrinsic biofilm treatments, strategies focused on aspects inherent to successful device implantation–not only must the implant succeed in preventing or treating infection, but it must also allow osseointegration so that it does not detach from the bone over time. In addition, while active coatings are targeted to work on acute infections, passive antimicrobial properties of the implant must last for its lifetime, usually about 20 years for most implants, and so have an increased need for efficacy in treating delayed or chronic infections. There remains a theoretic concern that for any coating that releases an antimicrobial substance that sub-inhibitory concentrations of any given agent could in fact, increase resistance. This poses challenges for developing intrinsic systems that can deliver an antimicrobial compound at adequate concentrations for long periods of time. There may be some role for intrinsic properties of an implant being used to prevent acute infections in the immediate post-surgical period, but this would then necessitate a method that could treat delayed or chronic infection. Novel methods have been proposed that address each of these needs. Yet, while many of them make use of pharmacological and physical methods for both prevention and treatment, there are limited methods available clinically for other uses such as catheters and ET tubes in Canada and Europe; however, no methods have been proven clinically in the US for PJI [
69,
70]. Thus, we do not yet know the feasibility of implementing these strategies in the clinic, nor the cost of using these new approaches versus cost of current treatment strategies; nor do we know the true longevity of the antimicrobial properties of the implant. However, these emerging technologies may be viable future options to explore and expand on to meet the continuing challenges that PJI biofilms present.



Comments (0)