1. IntroductionNon-small-cell lung cancer (NSCLC) is the most common cause of cancer-related mortality worldwide, and the most prevalent cell type of this cancer is adenocarcinoma [
1]. Brain metastasis is common in advanced NSCLC. Approximately 10–20% of patients have brain metastasis at initial diagnosis of NSCLC, and about 20–40% develop brain metastasis during treatment [
2]. The standard treatment for NSCLC patients with brain metastasis is chemotherapy combined with intracranial intervention, for example, craniotomy or radiotherapy, beforehand [
3]. However, not all NSCLC patients with brain metastasis are suitable for surgery due to factors such as poor performance status, tumor occurrence in an inoperable site, and multiple brain metastases [
4]. Although the rate of incidence of surgical complications is not high as previously thought, careful, shared decision-making about surgery is still necessary. Some NSCLC patients with brain metastasis are treated with radiotherapy, but previous reports show poor prognoses and a median survival of about 6 months [
5]. In addition, NSCLC patients with brain metastasis may show poor responsiveness to chemotherapy, including poor response rates (27–69%) and a short duration of overall survival (OS) (7.4–10 months) [
6,
7,
8]. In the era of precision medicine, the development of epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) has changed clinical practice. The rate of incidence of the EGFR mutation in NSCLC patients is approximately 40–60% among Asian and 10% among Western patients [
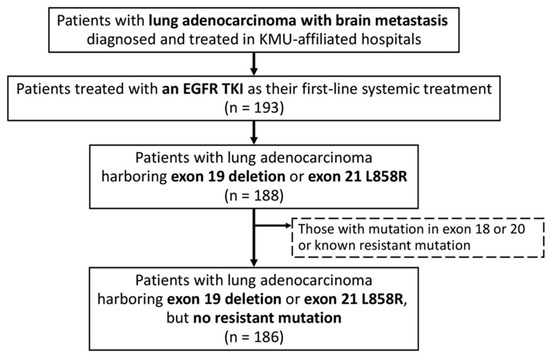
9]. In recent years, randomized trials have further shown that patients with NSCLC harboring susceptible EGFR mutations, such as the exon 21 L858R point mutation and exon 19 deletion, have longer progression-free survival (PFS) when they are treated with EGFR TKIs rather than standard chemotherapy [
10,
11,
12,
13,
14,
15,
16]. Previous studies have also reported encouraging results for EGFR TKI treatment of patients with EGFR mutations and brain metastasis [
10,
13,
14,
15,
17,
18,
19].EGFR TKIs have different in vitro sensitivities, plasma drug concentrations, clinical responses, and rates of penetration into the cerebrospinal fluid from the plasma [
20,
21,
22,
23,
24]. According to previous studies which compared the treatment outcomes of different EGFR TKIs for EGFR-mutant NSCLC patients with brain metastasis, different first-line EGFR TKIs achieved similar treatment outcome [
25]. However, the clinical efficacy of different EGFR-TKI-only treatments for patients with brain metastasis is still unknown. In addition, EGFR TKIs combined with brain surgery or radiotherapy to treat metastatic brain tumors is still a popular strategy for patients with EGFR mutations and brain metastasis. However, memory impairment is inevitable in NSCLC patients with brain metastasis after whole-brain radiotherapy [
26]. The role of surgery or radiotherapy in treating patients with susceptible EGFR mutations and brain metastasis is still unclear. We conducted this retrospective study with real-world data from three hospitals to determine the optimal treatment strategy for EGFR-mutant NSCLC patients with brain metastasis. 4. Discussion
This study made several important findings. First, the patients who received intracranial intervention and those who did not showed a similar response to the initial treatment; these groups were also similar in PFS and OS. Second, patients responded in a similar way to gefitinib, erlotinib, afatinib, and osimertinib as the initial treatment. Third, afatinib and osimertinib were independent prognostic factors of a better PFS, while male sex and bone metastasis were independent prognostic factors of a poorer PFS. The independent prognostic factors of a poorer OS were male sex and extracranial metastasis. Finally, GPA versions 2017 and 2022 appropriately stratified patients with different OS, while patients with higher GPA scores had significantly longer OS.
Brain metastasis is associated with poor prognosis of NSCLC patients [
34]. Systemic therapy combined with surgery or radiotherapy is the standard treatment. A previous retrospective study of 296 patients evaluated the benefits of craniotomy for patients with NSCLC and brain metastases. Most of the patients had ≤3 brain lesions, and about 90% of the patients received whole-brain radiotherapy for their brain metastasis. However, the overall survival of the relatively few patients (less than 10%) who underwent craniotomy was significantly longer. Regardless of EGFR mutation status, craniotomy remains a strong prognostic factor of better survival. Some patients may develop complications after craniotomy, the most serious being intracranial hemorrhage, which could cause mortality [
35]. In our study, 27% of the patients underwent craniotomy for brain metastasis, but their PFS and OS were similar to those of patients who did not have these interventions.Radiotherapy for brain lesions is the standard of care for brain metastasis in patients who are not suitable for craniotomy. In a previous retrospective study, which compared the efficacy of first-line EGFR TKIs in combination with radiotherapy vs. EGFR TKI only for patients with EGFR-mutant lung adenocarcinoma with brain metastasis, treatment of symptomatic brain metastasis with the combined therapy achieved a higher response rate and significant improvement in iPFS than did EGFR TKI alone [
36]. However, in patients with asymptomatic brain metastasis, the combined EGFR TKI and radiotherapy treatment and EGFR-TKI-only treatment achieved similar iPFS, but the former may result in memory or cognition impairment months later [
36]. Another study that evaluated patients with metastatic brain cancer receiving whole-brain radiotherapy showed significant memory impairment after brain radiotherapy. These results suggest that memory impairment may be an early marker of cognitive impairment in patients with brain metastasis who undergo brain radiotherapy [
26]. In the present study, 33% of the patients received radiotherapy, which, in almost all cases, was whole-brain radiotherapy. We found that the rate of response to systemic treatment, PFS, and OS of patients receiving radiotherapy were similar to those of patients who did not receive radiotherapy. The intracranial intervention had no statistically significant impact on the survival of the patients with EGFR mutations who received only EGFR TKIs as the first-line therapy.Although NSCLC progression depends on driver mutations, it is also affected by the extracellular matrix interaction which is mediated by integrins [
37,
38]. Integrins are cell adhesions and play a key role in the regulation of the process of tumor angiogenesis, which consists of basement membrane degradation and endothelial cell migration, proliferation, and stabilization [
39,
40]. EGFR regulates integrin activation and cell adhesion, providing control over cellular responses to the environment [
41]. Deciphering the molecular mechanisms underlying EGFR and extracellular matrix interactions might provide a better understanding of disease pathobiology and aid in developing therapeutic strategies. According to previous studies, EGFR TKIs are still the standard first-line treatment for EGFR-mutant NSCLC patients. Gefitinib, a first-generation EGFR TKI, has been reported to have low efficacy in treating brain metastasis and poor rates of penetration of the cerebrospinal fluid from the plasma [
42]. In contrast, erlotinib, another first-generation EGFR TKI, is effective in treating brain metastasis, is able to cross the blood–brain barrier, and shows a relatively high concentration in the cerebrospinal fluid [
43]. Therefore, physicians frequently prescribe erlotinib instead of gefitinib for patients with brain metastasis. Furthermore, the LUX-Lung 3 and LUX-Lung 6 trials showed that afatinib is effective against metastatic brain tumors and yields significantly improved treatment outcomes [
13,
14]. The FLAURA trial demonstrated that, compared to first-generation TKIs, osimertinib causes a statistically significant improvement in the treatment outcomes of patients with brain metastasis [
15,
16]. In the subgroup analysis of the central nervous system response in the FLAURA study, osimertinib had significantly better central nervous system efficacy, and patients had a lower intracranial progression rate compared to those who received first-generation EGFR TKIS [
44]. The results of the BLOOM study also showed an excellent treatment effect of osimertinib in patients with leptomeningeal carcinomatosis [
24]. Chen et al. compared first- and second-generation EGFR TKIs for the treatment of brain metastasis and found no significant differences in PFS, OS, or iPFS in real-world practice between patients who received different generations of EGFR TKIs [
25]. In our study, we compared the efficacy between first-, second- and third-generation EGFR TKIs for the treatment of mutant-EGFR lung cancer with brain metastasis. All four EGFR TKIs had similar response rates, but significantly different PFS. Their clinical efficacy was similar in patients without intracranial intervention for brain metastasis. The OS of patients taking different EGFR TKIs was also different. Patients treated with osimertinib had the longest OS compared to those treated with gefitinib, erlotinib, or afatinib. In addition, the OS of patients treated with afatinib was longer than that of patients receiving first-generation EGFR TKIs.Older age, poor performance status, and extracranial metastasis are regarded as independent factors of poor prognosis of patients with brain metastasis [
45]. Chen et al. found that NSCLC patients with uncommon mutations, multiple brain metastases, and concomitant liver metastases tended to have a shorter OS [
25]. In our study, multivariable analyses with backward variable selection confirmed that afatinib and osimertinib are independent prognostic factors of better PFS, while male sex and bone metastasis are independent prognostic factors of poorer PFS. Independent prognostic factors of poorer OS included male sex and extracranial metastasis.GPA has previously been used in decision-making to treat NSCLC patients with brain metastasis [
31]. The DS-GPA has been upgraded to the lung-molGPA, which includes the EGFR and ALK mutation status and PD-L1 expression [
33]. The lung-molGPA has six factors, with total scores ranging from 0 to 4. Cheng et al. examined the effects of lung-molGPA and different treatment strategies on survival of EGFR-mutant NSCLC patients with brain metastasis; a lung-molGPA of ≥3 was associated with improved OS [
46]. In our study, GPA versions 2017 and 2022 appropriately stratified patients with different OS, while patients with higher GPA scores (≥2.5 by version 2017 and ≥3 by version 2022) had significantly longer OS.
Our study has several limitations. First, the number of patients receiving osimertinib was relatively small compared to the number receiving other EGFR TKIs under Taiwan’s National Health Insurance system rules. Taiwan’s National Health Insurance (NHI) is a government-run, single-payer program introduced in 1995 that now covers more than 99% of all Taiwanese citizens. Only gefitinib, erlotinib, and afatinib were allowed by Taiwan’s NHI before 2020. Osimertinib was relatively expensive, and only some patients could afford osimertinib. Osimertinib has been allowed for lung adenocarcinoma with brain metastasis in the deletion 19 subgroup by Taiwan’s NHI since April 2022. This is the reason why only small numbers of patients with lung cancer with brain metastasis were treated with osimertinib in our study. Second, the choice of EGFR TKI for the patient may depend on clinicians’ decisions, which may be influenced by previous studies. In our study, the erlotinib group had significantly more patients than the other groups. Third, the type of radiotherapy for brain tumors in our study was almost always whole-brain radiotherapy. Only a few patients received stereotactic radiosurgery for brain metastasis. Furthermore, iPFS was difficult to evaluate in our study because of its retrospective nature and the check-up interval of the brain image not being clearly defined, which may influence the accuracy of the evaluation of iPFS.




Comments (0)