

 Figure 3.
Surveillance guidelines for mucinous pancreatic cysts (Adapted from the 2018 ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts). a Size-based surveillance guidelines only apply in the absence of high-risk features (see
Figure 3.
Surveillance guidelines for mucinous pancreatic cysts (Adapted from the 2018 ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts). a Size-based surveillance guidelines only apply in the absence of high-risk features (see 

Remember me
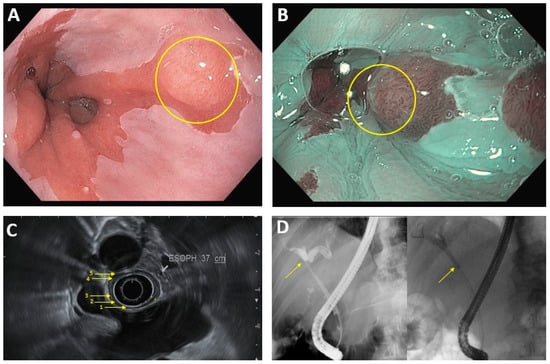







Figure 1. Common endoscopic modalities. (A): Conventional HD endoscopy showing Barrett’s esophagus with lesion (circled). (B): Image in 1A under NBI. Area of abnormal vascular and mucosal patterns (circled) is concerning for malignancy. (C): EUS of the esophagus. Arrows denote 5 alternating hyperechoic/hypoechoic layers: (1) mucosal surface, (2) muscularis mucosa, (3) submucosa, (4) muscularis propia, (5) serosa. (D): ERCP in hilar cholangiocarcinoma. Left image: dilation of intrahepatic bile ducts because of complete blockage of the common hepatic duct (arrow). Right image: improved flow of bile/contrast after deployment of plastic biliary stent across the malignant obstruction.
Figure 1. Common endoscopic modalities. (A): Conventional HD endoscopy showing Barrett’s esophagus with lesion (circled). (B): Image in 1A under NBI. Area of abnormal vascular and mucosal patterns (circled) is concerning for malignancy. (C): EUS of the esophagus. Arrows denote 5 alternating hyperechoic/hypoechoic layers: (1) mucosal surface, (2) muscularis mucosa, (3) submucosa, (4) muscularis propia, (5) serosa. (D): ERCP in hilar cholangiocarcinoma. Left image: dilation of intrahepatic bile ducts because of complete blockage of the common hepatic duct (arrow). Right image: improved flow of bile/contrast after deployment of plastic biliary stent across the malignant obstruction.
Figure 2. Surveillance guidelines for Barrett’s esophagus. a “Treated” assumes complete eradication of intestinal metaplasia (CEIM). b Treatment is recommended in all cases of high-grade dysplasia.
Figure 4. (A): Endoscopic mucosal resection (EMR) by band and snare technique: (I) Initial 1 cm, slightly raised esophageal lesion with surrounding Barrett’s esophagus. (II) Abnormal mucosal area is being capture completely into the cap with a cuff of normal surrounding mucosa. (III) Snare deployed around the band and resected using blended current. (IV) Resection base after cautery of underlying vessels. (B): Endoscopic Submucosal Dissection (ESD): (I) Initial large, well-demarcated lesion of the stomach. Lesions of the border are usually marked in the beginning and methylene bue or other lifting agents are injected to elevate the lesion (not performed here). (II) The lesion is resected with a needle-knife using electrocautery, starting at the previously demarcated margins. (III) Base of the lesion that has been fully resected. (IV) 3 cm resected lesion.
Figure 4. (A): Endoscopic mucosal resection (EMR) by band and snare technique: (I) Initial 1 cm, slightly raised esophageal lesion with surrounding Barrett’s esophagus. (II) Abnormal mucosal area is being capture completely into the cap with a cuff of normal surrounding mucosa. (III) Snare deployed around the band and resected using blended current. (IV) Resection base after cautery of underlying vessels. (B): Endoscopic Submucosal Dissection (ESD): (I) Initial large, well-demarcated lesion of the stomach. Lesions of the border are usually marked in the beginning and methylene bue or other lifting agents are injected to elevate the lesion (not performed here). (II) The lesion is resected with a needle-knife using electrocautery, starting at the previously demarcated margins. (III) Base of the lesion that has been fully resected. (IV) 3 cm resected lesion.
Table 1. Screening Guidelines for pre-malignant upper GI lesions.
Table 1. Screening Guidelines for pre-malignant upper GI lesions.
Screening/Surveillance GuidelinesHigh Risk FeaturesScreening or Surveillance ModalitiesBarrett’s esophagus (BE)Men w/ chronic GERD (>5 years) occurring > once/week and ≥2 risk factors (ACG 2022)(1) Age > 50Transnasal endoscopy (screening only):
-good sensitivity (91%) and specificity (96%)
-cheaper than EGD
-cannot perform interventions
Cytosponge (screening only):
-cheaper than EGD
-cannot perform interventions
-Newer technique; not widely used in the United States
Surveillance every 3–5 years in patients with GIM and high-risk features (AGA 2018)
(1) Incomplete intestinal metaplasiaCysts with high-risk features should undergo EUS-FNA to evaluate histology.
Cysts without high-risk features should undergo surveillance (ACG 2018).
(1) Cyst size ≥ 2 cmEUS
-Used in high-risk cases and when imaging is non-diagnostic
No definitive surveillance guidelines for patients without FAP.
Components of Spigelman class:Table 2. Categories of Pancreatic Cysts.
Table 2. Categories of Pancreatic Cysts.
Cyst CategoryImaging AppearanceTable 3. Upper GI cancer Staging and Treatment.
Table 3. Upper GI cancer Staging and Treatment.
Staging ModalitiesEndoscopic Treatment OptionsLuminal Upper GI cancer aEUS:CT:
-Used for M-staging
-Lower sensitivity and specificity for N-staging, when compared to EUS
Surgical resection vs systemic therapy for larger and more advanced tumors
Extraluminal upper GI cancer bEUS:Laparoscopy:
-Most accurate diagnostic modality for gallbladder cancer and cholangiocarcinoma
Cross-sectional imaging:
-Modality of choice for diagnosing intrahepatic cholangiocarcinoma and evaluating resectability in pancreatic cancer
-Used for M-staging
Comments (0)