Obstructive sleep apnea is associated with depressed myocardial mechanoenergetics
Methods
In this cohort study, we included a total of 382 eligible participants without cardiovascular disease in a tertiary outpatient clinic between January 2013 and January 2015. We recorded demographic, clinical, polysomnographic and echocardiographic variables of the patients. In addition, myocardial mechanoenergetic efficiency (MEE) and MEEi were calculated by an echocardiography-derived validated measurement.
Results
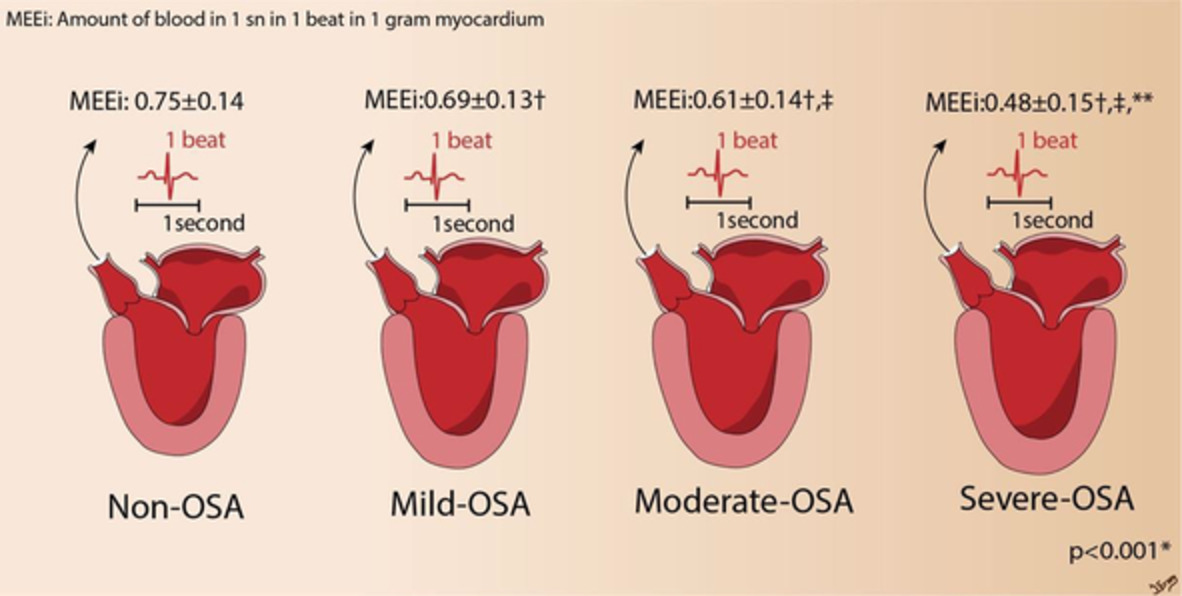
The mean (±SD) age of the participants was 48.47 ± 12.13, and male/female ratio was 287/95. Comparing with non-OSA, MEEi was significantly lower in OSA patients at all stages (0.35 ± 0.08 vs. 0.42 ± 0.05; p < .001). MEEi was negatively correlated with hypertension (r = −0.518, p < .001), body mass index (r = −0.382, p < .001), AHI (r = −0.656, p < .001), total apne (r = −0.525, p < .001), hypopnea (r = −0.415, p < .001), systolic pulmonary pressure (r = −0.318, p < .001), relative wall thickness (RWT; r = −0.415, p < .001), and positive correlated with left ventricular ejection fraction (r = 0.586, p < .001). According to multiple linear regression analysis AHI (β = −0.625, p < .001), total apnea (β = −0.402, p = .001), hypopnea (β = −0.395, p = .001), LV ejection fraction (β = 0.478, p < .001) and RWT (β = −0.279, p < .001) have an independent relationship with MEEi.
Conclusions
MEEi was lower in OSA patients. A reduced MEEi may reflect a disturbance in energy use of the myocardium. Consequently, our results may provide insight into the mechanisms leading to structural cardiac diseases in OSA patients.

Comments (0)