
Remember me





Stroke, a cerebral vascular disease, is divided into ischemic and hemorrhagic stroke.1-3 Statistically, the overall incidence of first-ever stroke and mortality rate was 345.1 and 159.2 per 100 000 person-years in China.4 Acute ischemic stroke (AIS), the most common type, is mainly attributable to diverse risk factors, such as hypertension, diabetes, hypercholesterolemia, and smoking.5, 6 AIS may lead to disability due to ischemia-induced injury and the death of neuronal cells.7, 8 Although advancement in the identification of risk factors and intravascular interventional therapy improves the survival rate of patients,9, 10 the prognosis of patients with AIS is still unsatisfactory, with a high relapse rate of 14.8% within 5 years.11 Therefore, finding more potential predictors for early identification of AIS in patients with a high risk of relapse and enhancing management to improve their prognosis is crucial.
Long non-coding RNAs (lncRNAs) are involved in different cellular and biological processes12, 13; thus, they play important roles in diverse complex diseases, including neurological diseases.14-16 Several lncRNAs have been reported to exert protective roles, such as lncRNA metastasis associated with lung adenocarcinoma transcript 1 (MALAT1), N1LR, and Maclpil.16-18 Recently, it has been shown that lncRNA zinc finger antisense 1 (ZFAS1) alleviates neuronal inflammation and injury in AIS. For example, the overexpression of lncRNA ZFAS1 attenuates oxygen and glucose deprivation-mediated injury in an AIS cell model.19 Additionally, lncRNA ZFAS1 alleviates neuronal damage through suppressing inflammation, oxidative stress, apoptosis, and nitric oxide level in an AIS animal model.20 Regarding its clinical role in AIS, lncRNA ZFAS1 could be used as a noninvasive biomarker for the diagnosis of large-artery atherosclerosis stroke patients.21 However, the relationship of lncRNA ZFAS1 with disease risk, inflammation, disease severity, and prognosis of patients with AIS remains unclear.
Therefore, the present study assessed circulating lncRNA ZFAS1 expression in AIS patients, then aimed to illustrate the relationship of lncRNA ZFAS1 with neurological impairment, inflammation, recurrence-free survival (RFS), and overall survival (OS) of patients with AIS.
2 METHODS 2.1 ParticipantsFrom January 2015 to August 2018, 241 patients with first-episode AIS were consecutively recruited as the study population and 120 patients at high risk of stroke as controls. The recruitment criteria for AIS patients included: (a) diagnosis of AIS based on clinical manifestation and imaging examination; (b) at least 18 years of age; (c) admitted to the hospital within 12 h after the episode of symptoms; and (d) patients or their guardians agreed to participation in the study. The exclusion criteria were as follows: (a) concomitant hematological malignancies or cerebral tumor; (b) use of immunosuppressant within 1 month before enrollment; (c) severe infection within 1 month; and (d) pregnant or breast-feeding women. The controls were screened from populations at high risk of stroke, but without a history of stroke, and they were required to have two or more stroke risk factors, including smoking, hypertension, hyperlipidemia, hyperuricemia, diabetes mellitus, and chronic kidney disease. Additionally, at enrollment, the age of controls was limited in a range of 50–80 years, and the sex ratio was set to 3:2 (male:female), which was aimed at matching the age and gender of controls to the recruited AIS patients. The exclusion criteria for AIS patients were also applicable to the controls. The present study was approved by the Ethics Committee of the First Affiliated Hospital of Hebei North University.
2.2 Clinical feature recording and blood samplingDemographic information and comorbidities of the participants were documented after recruitment. The National Institutes of Health Stroke Scale (NIHSS) was employed to evaluate neurological impairment in AIS patients within 24 h (the higher the NIHSS score, the more severe the nerve damage). Peripheral blood (PB) was drawn from all participants on the day of enrollment. The PB samples from patients with AIS were divided into two parts: one was used to isolate the PB mononuclear cells (PBMCs) using density gradient centrifugation in the presence of polysucrose (Ficoll)-Urografin solution, and the other was centrifuged at 1000 g for 10 min to separate serum samples. For the controls, PBMCs were separated from PB using the same procedures. The samples were stored in liquid nitrogen following separation.
2.3 LncRNA ZFAS1 determinationThe PBMCs were subjected to quantitative analysis of lncRNA ZFAS1 expression using real-time reverse transcription-quantitative polymerase chain reaction (RT-qPCR). The PureZOL RNA isolation reagent (Catelog#732-6890, Bio-Rad, Hercules, CA, USA) was used for total RNA extraction. The iScript cDNA Synthesis Kit (Catelog#170-8890, Bio-Rad, Hercules, CA, USA) was used for complementary DNA (cDNA) synthesis. Then, RT-qPCR was performed using the ABI Applied Biosystems 7500 PCR System (Nanjing Junwei Biotechnology Co., LTD, Nanjing, Jiangsu, China) with the QuantiNova SYBR Green PCR Kit (Catelog#208054, Qiagen, Duesseldorf, Nordrhein-Westfalen, Germany), where the parameters were set as follows: PCR initial activation step for 2 min at 95 ºC; two-step cycling: denaturation for 5 sec at 95 °C, and combined annealing/extension for 10 sec at 60 °C. Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) used as an internal reference. The primers applied in the qPCR were constructed according to the previous study.20 The relative expression of lncRNA ZFAS1 was calculated using 2−ΔΔCt methodology.22
2.4 Inflammatory cytokine measurementEnzyme-linked immunosorbent assay (ELISA) with the quantitative sandwich enzyme immunoassay technique was employed to measure the inflammatory cytokines present in the serum of AIS patients, including tumor necrosis factor-alpha (TNF-α), interleukin-1 beta (IL-1β), and IL-6. The Human TNF-α Quantikine ELISA (Catalog#DTA00D), Human IL-1β Quantikine ELISA (Catalog#DLB50), and Human IL-6 Quantikine ELISA (Catalog#D6050) Kits were purchased from R&D Systems (Minneapolis, MN, USA). The assay was performed according to the manufacturer's instructions.
2.5 Follow-upFor the surveillance of stroke recurrence, all AIS patients were advised to undergo reexamination every 3 to 6 months or as clinically indicated. Follow-up examinations for patients were scheduled for a total of 36 months, and the last follow-up was conducted on August 31, 2021. RFS was calculated from the first hospitalization to the first stroke recurrence or death. OS was calculated from the first hospitalization to death. Patients who were lost to follow-up were processed as censored data.
2.6 Statistical analysisAnalysis of differences between groups was performed using the Chi-square test, Student's t-test, or Wilcoxon rank-sum test. Correlation analysis between variables was checked using the Spearman rank test or Wilcoxon rank-sum test. In the correlation analysis of lncRNA ZFAS1 expression with RFS and OS, patients were categorized into high- and low-expression groups based on the median expression value (0.417) of lncRNA ZFAS1 in AIS patients. Kaplan-Meier curves were employed to display RFS and OS, which were analyzed using the log-rank test. A two-sided P-value less than 0.05 (p > 0.05) was set to define statistical significance. SPSS 26.0 (IBM Corp., Armonk, New York, USA) and GraphPad Prism 6.01 (GraphPad Software Inc., San Diego, CA, USA) were used for analysis and plotting.
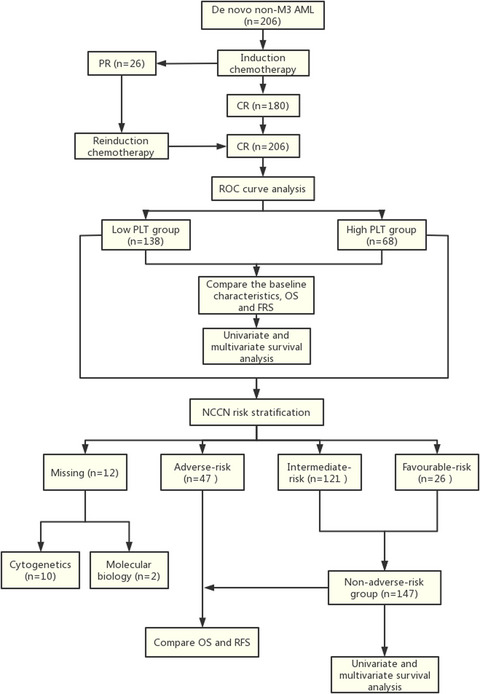
3 RESULTS 3.1 Study flowIn total, 279 AIS patients were screened for the current study, while 38 patients were excluded, including 21 patients for inclusion or exclusion criteria and 17 patients/guardians who declined participation. Thus, 241 patients were included in the study, and their PBMCs and serum were isolated from the blood samples. Next, the level of lncRNA ZFAS1 in PBMCs was evaluated using RT-qPCR, and the levels of TNF-α, IL-1β, and IL-6 in serum were assessed using ELISA. During follow-up examinations, the following was noted: 17 events happened within the 1st year, including 7 patients who experienced recurrences, 6 patients who died, and 4 patients who were lost to follow-up; 40 events happened within the 2nd year, including 8 patients who suffered from recurrences, 6 patients who died, and 26 patients who were lost to follow-up; and 54 events happened within the 3rd year, including 33 patients who underwent recurrences, 6 patients who died, and 15 patients who were lost to follow-up. All patients were included in the intention-to-treat analysis. The RFS and OS of patients were processed as censored data if they were lost to follow-up (Figure 1).

The flow diagram of this study
3.2 Characteristics of participantsAIS patients showed a mean age of 65.9 ± 9.4 years with 71 (29.5%) females and 170 (70.5%) males; the controls had a mean age of 64.5 ± 8.1 years with 48 (40.0%) females and 72 (60.0%) males. No difference in demographic characteristics (age, sex, body mass index (BMI), and history of smoking) was observed between AIS patients and controls (all p > 0.05). However, the percentage of patients with hypertension (p = 0.045) and hyperuricemia (p = 0.002), as well as the number of risk factors (p < 0.001), were higher in AIS patients than in controls. In AIS patients, the NIHSS score was 10.1 ± 4.9; the median (interquartile range [IQR]) values of C-reactive protein (CRP), TNF-α, IL-1β, and IL-6 were 14.8 (9.3–23.9) mg/L, 71.5 (56.4–95.6) pg/ml, 2.6 (2.0–3.8) pg/ml, and 37.9 (30.0–50.0) pg/ml, respectively. Other clinical features of the participants are presented in Table 1.
TABLE 1. Characteristics of AIS patients and controls Items Controls (N = 120) AIS patients (N = 241) Statistic (t/χ2/Z) p value Demographics Age (years), mean ± SD 64.5 ± 8.1 65.9 ± 9.4 −1.442 0.150 Gender, n (%) 3.564 0.059 Female 48 (40.0) 71 (29.5) Male 72 (60.0) 170 (70.5) BMI (kg/m2), mean ± SD 23.7 ± 3.0 24.2 ± 2.5 −1.568 0.118 History of smoke, n (%) 57 (47.5) 129 (53.5) 1.165 0.280 Underlying diseases Hypertension, n (%) 93 (77.5) 207 (85.9) 4.018 0.045 Hyperlipidemia, n (%) 64 (53.3) 117 (48.5) 0.734 0.392 Hyperuricemia, n (%) 31 (25.8) 103 (42.7) 9.809 0.002 Diabetes mellitus, n (%) 17 (14.2) 52 (21.6) 2.845 0.092 Chronic kidney disease, n (%) 14 (11.7) 43 (17.8) 2.298 0.130 No. of risk factors, mean ± SD 2.3 ± 0.5 2.7 ± 0.9 −5.386 <0.001 Disease features NIHSS score, mean ± SD - 10.1 ± 4.9 - - CRP (mg/L), median (IQR) - 14.8 (9.3–23.9) - - TNF-α (pg/ml), median (IQR) - 71.5 (56.4–95.6) - - IL−1β (pg/ml), median (IQR) - 2.6 (2.0–3.8) - - IL−6 (pg/ml), median (IQR) - 37.9 (30.0–50.0) - - Treatment Intravenous thrombolysis, n (%) - 24 (10.0) - - Endovascular interventions +Intravenous thrombolysis, n (%) - 217 (90.0) - - Abbreviations: AIS, acute ischemic stroke; BMI, body mass index; CRP, C-reactive protein; IL-1β, interleukin-1beta; IL-6, interleukin 6; IQR, interquartile range; NIHSS, National Institute Health of Stroke Scale; SD, standard deviation; TNF-α, tumor necrosis factor alpha. 3.3 Linkage of lncRNA ZFAS1 with AIS riskLncRNA ZFAS1 expression was lower in AIS patients than in controls (Z = −10.693, p < 0.001) (Figure 2A). Furthermore, the receiver-operating characteristic (ROC) curve showed that lncRNA ZFAS1 presented good value in identifying the risk of AIS with an area under the curve (AUC) of 0.845 (95% confidence interval [CI]: 0.802–0.888) (Figure 2B).

Long non-coding RNA zinc finger antisense 1 (lncRNA ZFAS1) expression in acute ischemic stroke (AIS) patients. Comparison of lncRNA ZFAS1 expression between AIS patients and controls (A); correlation of lncRNA ZFAS1 with AIS risk (B)
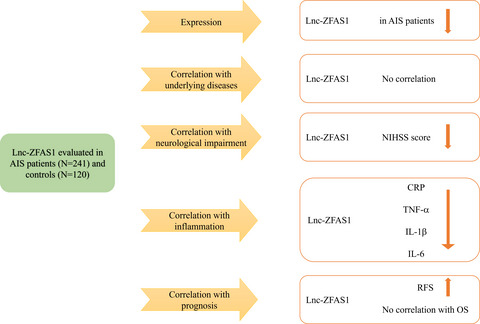
3.4 Correlation of lncRNA ZFAS1 with underlying diseases in AIS patientsThere was no association shown between lncRNA ZFAS1 and hypertension (Z = −1.655, p = 0.098), hyperlipidemia (Z = −1.688, p = 0.091), hyperuricemia (Z = −0.873, p = 0.383), diabetes mellitus (Z = −0.772, p = 0.440), or chronic kidney disease (Z = −1.867, p = 0.062) (Figure 3A-E).

The relationship of long non-coding RNA zinc finger antisense 1 (lncRNA ZFAS1) expression with underlying diseases in acute ischemic stroke (AIS) patients. Association of lncRNA ZFAS1 expression with hypertension (A), hyperlipidemia (B), hyperuricemia (C), diabetes mellitus (D), or chronic kidney disease (E)
3.5 Correlation of lncRNA ZFAS1 with neurological impairment in AIS patientsThe relationship between lncRNA ZFAS1 and NIHSS score in AIS patients is shown in Figure 4, which shows that lower lncRNA ZFAS1 expression was linked with higher NIHSS score (rs = −0.335, p < 0.001), which reflects a higher level of neurological impairment.

The relationship of long non-coding RNA zinc finger antisense 1 (lncRNA ZFAS1) expression with neurological impairment in acute ischemic stroke (AIS) patients
3.6 Correlation of lncRNA ZFAS1 with inflammation in AIS patientsLncRNA ZFAS1 expression was negatively associated with the levels of CRP (rs = −0.284, p < 0.001), TNF-α (rs = −0.293, p < 0.001), IL-1β (rs = −0.149, p = 0.021), and IL-6 (rs = −0.161, p = 0.012) (Figure 5A-D).

The relationship of long non-coding RNA zinc finger antisense 1 (lncRNA ZFAS1) expression with inflammation in acute ischemic stroke (AIS) patients. Association of lncRNA ZFAS1 expression with C-reactive protein (CRP) (A), tumor necrosis factor alpha (TNF-α) (B), interleukin 1β (IL-1β) (C), or IL-6 (D)
3.7 Correlation of lncRNA ZFAS1 with prognosis in AIS patientsLow lncRNA ZFAS1 expression was associated with worse RFS (χ2 = 6.222, p = 0.013). Additionally, the 1-year, 2-year, and 3-year RFS rates were 87.5%, 79.2%, and 71.6%, respectively, in AIS patients with low lncRNA ZFAS1 expression, and 94.2%, 88.3%, and 85.5%, respectively, in AIS patients with high lncRNA ZFAS1 expression (Figure 6A). However, lncRNA ZFAS1 expression was not associated with OS (χ2 = 1.404, p = 0.236). The 1-year, 2-year, and 3-year OS rates were 96.7%, 93.9%, and 89.6%, respectively, in AIS patients with low lncRNA ZFAS1 expression, and 98.3%, 95.8%, and 94.0%, respectively, in AIS patients with high lncRNA ZFAS1 expression (Figure 6B).

The relationship of long non-coding RNA zinc finger antisense 1 (lncRNA ZFAS1) expression with recurrence-free survival (RFS) and overall survival (OS) in acute ischemic stroke (AIS) patients. Correlation of lncRNA ZFAS1 expression with RFS (A) and OS (B) in AIS patients
Multivariate Cox's proportional hazards demonstrated that lncRNA ZFAS1 (high vs. low) was an independent risk factor for RFS (p = 0.042, HR = 0.506), but not for OS (p = 0.428, HR = 0.645) in AIS patients (Table S1).
4 DISCUSSIONThe role of lncRNA ZFAS1 in neurological diseases has gained wide attention. For instance, a study has shown that lncRNA ZFAS1 mediates spinal cord injury by binding to microRNA (miR)-1953 and regulating the phosphatase and tensin homolog (PTEN)/phosphoinositide 3-kinase (PI3K)/protein kinase B (AKT) pathway.23 Additionally, inhibiting lncRNA ZFAS1 modifies the apoptosis and autophagy of hippocampal neurons by activating the PI3K/AKT pathway and increasing miR-421 expression in epilepsy.24 Silencing lncRNA ZFAS1 regulates the recovery of neurological function in traumatic brain injury.25 In the AIS cell model, lncRNA ZFAS1 attenuates cell damage by upregulating pro-survival protein myeloid cell leukemia-1 (MCL-1) by sponging miR-186-5p.19 However, the relationship between lncRNA ZFAS1 expression, disease risk, and neurological impairment in AIS patients is still not fully understood. In our study, the circulating lncRNA ZFAS1 expression was lower in AIS patients than in controls, and its expression could be used to distinguish AIS patients from controls. Additionally, lncRNA ZFAS1 expression was negatively correlated with NIHSS score. This may be because (1) lncRNA ZFAS1 might protect neurons against inflammation and damage caused by acute cerebral ischemia, which reduces the risk of AIS; thus, lncRNA ZFAS1 expression was lower in AIS patients20; (2) lncRNA ZFAS1 might inhibit neuronal cell apoptosis through the B-cell lymphoma-2 (Bcl-2)/Bcl-2 associated x protein (Bax)/cleaved cysteine proteases (caspases)-3 pathway,20 which decreases the severity of neurological impairment in AIS patients; therefore, lncRNA ZFAS1 was linked with lower NIHSS score.
LncRNA ZFAS1 regulates the inflammatory response and exerts anti-inflammatory effects in diverse human diseases.26-28 For example, overexpression of lncRNA ZFAS1 decreases pro-inflammatory cytokines in sepsis-induced acute lung injury by targeting miR-193a-3p.29 In addition, a study focusing on AIS presents that lncRNA ZFAS1 inhibits inflammation in an animal model,20 while the correlation of lncRNA ZFAS1 with inflammation in AIS patients remains unclear. Our study showed that high expression of lncRNA ZFAS1 was associated with low levels of CRP, TNF-α, IL-1β, and IL-6. The explanation might be that lncRNA ZFAS1 decreases miR-582 expression and upregulates nitric oxide synthase 3 (NOS3) expression to reduce the production of pro-inflammatory cytokines, thereby alleviating inflammation in AIS patients.20
The prognostic value of lncRNA ZFAS1 is a potential biomarker for prognosis in human diseases.30-32 For example, elevated lncRNA ZFAS1 is associated with poor survival in chronic heart failure patients33; however, lncRNA ZFAS1 is used as a predictive factor for better prognosis in sepsis patients.34 The predictive value of lncRNA ZFAS1 for outcomes in AIS remains unclear. In our study, we observed that high expression of lncRNA ZFAS1 was associated with better RFS in AIS patients while no correlation was found between lncRNA ZFAS1 and OS. This result might be caused by: (1) abnormal lipid metabolism is an independent factor for AIS recurrence, while lncRNA ZFAS1 hampered the cholesterol efflux rate in an atherosclerosis cell model,27 showing that lncRNA ZFAS1 had a positive association with RFS; (2) lncRNA ZFAS1 was negatively linked with neurological impairment, and lncRNA ZFAS1 was correlated with favorable RFS in AIS patients; (3) our sample size was not large enough and the follow-up time was not long enough, resulting in the relationship of lncRNA ZFAS1 with OS not being shown.
In addition, some deficiencies exist in our study. First, all AIS patients were from China, which might mean that our conclusion had a bias against other ethnic populations. Second, we discovered that lncRNA ZFAS1 is associated with inflammation, but the mechanism by which lncRNA ZFAS1 mediates inflammation in patients with AIS requires further exploration in future studies. Third, we only included first-episode AIS patients, our summary could not be adapted to chronic or recurrent ischemic stroke. Fourth, we only evaluated the levels of lnc-ZFAS1 and inflammation in AIS patients one time, which was inadmissible as the proof to present the causality between lnc-ZFAS1 and inflammation. Fifth, zinc finger protein is associated with inflammation,35 further study should conduct to explore the correlation of zinc finger protein with inflammation in AIS.
In conclusion, lncRNA ZFAS1 is downregulated, and its lower expression is associated with more severe neurological impairment, increased inflammation, and worse RFS in AIS patients; therefore, lncRNA ZFAS1 may be a potential biomarker to manage AIS patients to improve their outcomes.
ACKNOWLEDGEMENTSThis study was supported by Scientific Research Fund of Zhangjiakou (No. 2121146D).
CONFLICTS OF INTERESTThe authors have no conflicts of interest to disclose.
Comments (0)