
Remember me


Approximately 1.6 million people in the United States have type 1 diabetes (T1D).1 The incidence of T1D is increasing in the United States across all populations, most significantly among Hispanic and non-Hispanic Black (NHB) patients.2, 3 Unfortunately, widespread inequities exist in health outcomes among patients with T1D in the United States.4-7
In 2016, the T1D Exchange Quality Improvement Collaborative (T1DX-QI) was established.8 T1DX-QI is a learning health network9 with over 40 centers across the United States. Participating centers use continuous quality improvement (QI) methods10-12 and real-world electronic medical record (EMR) data4, 6 for T1D population health improvement.
The T1DX-QI is coordinated by the T1D Exchange, a Boston-based nonprofit coordinating center. The goals of the T1DX-QI were described in a separate commentary.13
The T1DX-QI has successfully used QI principles and implementation science to improve clinical processes, including increased use of continuous glucose monitors (CGM), insulin pumps, depression screening, improved access to care, and population-level glycemic outcomes.9-12
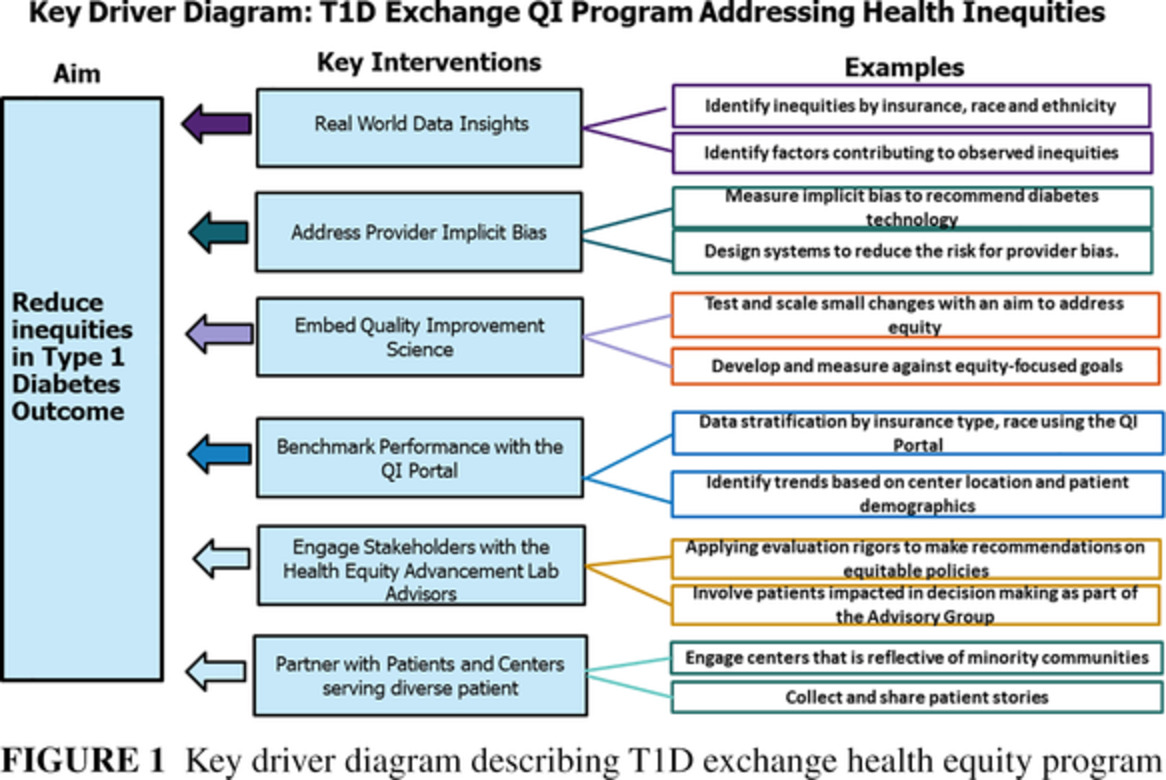
In 2020, the T1DX-QI established its health equity program to address inequities systematically and comprehensively in T1D outcomes.14 This commentary describes practical approaches being employed by the T1DX-QI to address health inequities. These approaches can be valuable examples for diabetes researchers and providers interested in addressing health inequities (Figure 1).

Key driver diagram describing T1D exchange health equity program
2 T1DX-QI APPROACHES TO ADDRESSING HEALTH INEQUITIES IN THE UNITED STATES 2.1 Identify inequities with real-world EMR dataThe T1DX-QI uses its unique EMR database with de-identified data on over 35 000 people with T1D to perform population health analysis. Recent analyses have revealed troubling and unnecessary inequities in diabetes device use and health outcomes.4, 6 Majidi et al,4 in an analysis of the T1DX-QI population health data of 18 000 patients with T1D (73% non-Hispanic White [NHW]; 8% NHB, 9% Hispanic, 10% other), found significant differences in glycosylated hemoglobin (HbA1c) in NHB and Hispanic patients with T1D compared to NHW patients (NHB 10.3%; Hispanic 9.2%; NHW 8.3%; P < .001). NHB patients also had the lowest rate of CGM use (NHB 17%; Hispanic 37%; NHW 40%; P < .001) and insulin pump use (NHB 41%; Hispanic 56%; NHW 60%; P < .001). Desalvo et al,6 using real-world pediatric data from the T1DX-QI, found that among youth with private insurance, NHB patients with T1D had less use of CGM than NHW patients with private as well as public insurance.
These inequities were amplified with the onset of the COVID-19 pandemic, as uncovered in the T1D Exchange COVID-19 Surveillance study.5, 15, 16 Ebekozien et al5 found that NHB patients with T1D and COVID-19 had about four times increased odds of being hospitalized for COVID compared to NHW patients. In addition, Noor et al15 found a strong association between device use and race-ethnicity, with an increased risk for hospitalization among patients with T1D not using diabetes technology.
In addition to driving QI initiatives, these real-world EMR data are used to support advocacy efforts. The T1DX-QI shares these data with state and national diabetes advocates to influence policy decisions that can positively impact systemic changes, such as efforts to increase access to diabetes management technologies like CGM.
2.2 Measure and address diabetes provider implicit biasImplicit or unconscious bias is a well-documented provider-level contributor to the inequities in health care generally as well as in diabetes management17 and can play a role in access to and use of diabetes technology and quality of care. The T1DX-QI collaboratively adapted the D-Provider Implicit Bias tool (D-PIB)17 to measure implicit racial bias related to technology recommendations in seven pilot sites. Over 200 diabetes clinic team members were assessed and trained in the pilot phase. Future publications will include the results of the implicit bias assessment and evaluate the effectiveness of provider implicit bias training as an intervention to address systemic inequities in T1D management.
2.3 Use of QI science to address institutional contributors to racismQI is a practical approach to test changes and sustain successful interventions.11, 12 Due to the thoughtful approach and emphasis on process changes, QI has extensive applicability to T1D management and can help address health inequities with suitable equity adaptations. In 2020, the T1DX-QI developed an Equity Framework,18 which is an adapted QI method designed to promote equity principles in QI interventions. The framework consists of 10 practical steps. Steps include reviewing baseline data for inequities, inviting patients and families to participate in QI activities, and examining local systems and processes for factors contributing to inequitable outcomes. It is now being used in an ongoing Health Equity QI Project by seven sites with a goal of reducing inequities in insulin pump and CGM use.
Data were collected and analyzed at baseline to identify opportunities to improve technology use, and sites will continue to submit monthly data, stratified by race and ethnicity, to monitor ongoing progress toward project goals. In addition, relevant data are extracted from EMR, flowsheets, or other appropriate documentation sources.
2.4 Equip the T1DX-QI EMR Portal benchmark tool to address inequitiesThe QI Portal, launched by the T1DX-QI in 2019, is an online platform developed with business intelligence software.19 Participating clinics securely share patient-level de-identified data monthly to a central data warehouse that is then transmitted to the portal. T1DX-QI clinics can assess, benchmark, and visually chart their EMR data with other clinics using the same improvement metric definitions. Clinics have access to the following: (1) the Dashboard Tab, with a clinic-to-clinic ranking on quality metrics; (2) the Compare Tab, with fully customizable benchmarking features, allows sites to compare outcome trends across clinics; (3) the Reports Tab, with built-in statistical process control charts to identify improvement trends and filter data by demographic indicators, including race, ethnicity, and insurance coverage; and (4) the Library Tab allows access to T1DX-QI case studies, QI publications, and other related improvement tools and resources.
New features released in 2021 allow clinics to display data stratified by race and ethnicity to visualize equity in key T1D metrics, including HbA1c, CGM use, insulin pump use, diabetic ketoacidosis events, and percentage of eligible patients completing depression screening. This feature builds on the existing health equity functionality by allowing sites to filter by a single racial or ethnic identity and simultaneously display multiple data series for ease of comparison. The QI Portal is a tool for sites to use real-time data to review trends and quickly identify opportunities for improvement, optimizing EMR data as a critical strategy in reducing inequities.
2.5 Engage diverse people with T1D and leaders from the Health Equity Advancement Lab (HEAL) Advisory CommitteeIn 2021, T1DX-QI established the HEAL Advisory Committee, a network of experienced health equity clinical and research leaders. The goal of this group is to provide thought leadership around T1DX health equity initiatives.14 The HEAL Advisory Committee contributes to best practices regarding equitable T1D care through multiple strategies. The group activities include developing new health equity measures, providing advice and feedback on new health equity initiatives, applying evaluation rigor, assisting in formulating recommendations for equitable policies, and sharing learning and best practices nationally.
2.6 Partner with people with T1D and clinics serving diverse people with T1DThe T1DX-QI engages with patients on multiple levels to involve them in process improvement. Patients are regularly invited to participate in QI activities, including QI projects led through the health equity pilot. Two members of the T1DX-HEAL are patients or parents of patients with T1D. They advise action steps alongside the clinical and research staff. Additionally, the T1DX-QI intentionally partners with endocrinology clinics serving diverse populations. Two recently contracted clinics reside in urban safety-net hospitals which primarily serve underserved and vulnerable populations, including communities of color, families whose primary language is not English, and un- or underinsured individuals.20
3 CONCLUSIONThis commentary describes six approaches with actionable steps that the T1DX-QI program is applying to address inequities in T1D care. Although addressing health inequities is an extremely complex issue, with the intentionality and engagement of diverse stakeholders, closing gaps in inequitable care and outcomes is achievable.
ACKNOWLEDGEMENTSWe appreciate all members of the T1DX-QI and T1DX-HEAL advisory committees.
We acknowledge Medtronic Diabetes for funding the T1DX-QI Health Equity Pilot Program.
Special thanks to the Leona M. and Harry B. Helmsley Charitable Trust that funds the T1DX-QI Collaborative.
DISCLOSURESO.E. is a member of the Medtronic Diabetes Health Equity Advisory Board. He is the principal investigator for research projects funded by Eli Lilly, Medtronic Diabetes, Abbot, and Dexcom. All the funds for these industry-funded projects and board roles are paid directly through his organization T1D Exchange. R.S.W. participates in multicenter clinical trials through her institution, sponsored by Medtronic, Insulet, Eli Lilly, Boehringer Ingelheim, Novo Nordisk, and Kowa, and Dexcom has contributed CGM for other studies. R.R. is an associate editor for the Journal of Diabetes. Other authors have no relevant disclosures.
Comments (0)