
Remember me


Coronavirus disease 2019 (COVID-19) vaccines are considered the most effective intervention to control the worldwide coronavirus epidemics we are nowadays confronted with.1
However, as for all types of drugs and vaccines, COVID-19 vaccines can cause adverse reactions, mainly from vaccine-induced immune responses.1, 2 Some of these may also involve the skin, often scaring unaware patients for the eye-catching, unfamiliar presentation.2
A better understanding of such adverse reactions may reduce concerns and promote the vaccination of large population groups.
For this reason, to provide a report on COVID-19 vaccine skin reactions, we collected all the patients' reports from our Dermatology Primary care to understand which cutaneous reactions were related to vaccination.
2 MATERIALS AND METHODSFrom March 2021 to June 2021 all the patients admitted for any dermatological issue at the Dermatology Primary Care, after the first aid triage, were asked for recent COVID-19 symptoms, exposures, and vaccination. All the reports were retrospectively examined to collect data on possible associations between cutaneous manifestations and COVID-19 vaccination.
3 RESULTSOf 200 patients (116 women, 84 men) admitted to the Dermatology Primary Care, who had been vaccinated against COVID-19, 21 (10.5%) referred cutaneous reactions after COVID-19 vaccination (Table 1).
Table 1. Features of patients, vaccines and cutaneous manifestations Patient no Age Sex Onset time from vaccination Vaccination type Dose no Cutaneous manifestations Other symptoms Presumed COVID-19 vaccine association 1 48 F 3 h Oxford-AstraZeneca 2nd Small pruritic wheals on the upper limbs and chest None reported Correlated 2 27 F 4 h BioNTech/Pfizer 2nd Generalized maculopapular pruritic rash, with erythemtous patches on the knees Headache Correlated 3 29 F 12 h Oxford-AstraZeneca 1st Facial swelling, flushing and erythema Headache, nausea, asthenia Correlated 4 76 M 24 h Oxford-AstraZeneca 1st Maculopapular with micropapules and urticarial pruritic generalized rash Headache, fever Correlated 5 67 M 48 h Moderna 2nd Bullous pruritic erythema multiforme Headache, fever, was hospitalized Correlated 6 58 M 48 h BioNTech/Pfizer 1st Maculopapular pruritic generalized rash None reported Correlated 7 84 M 48 h BioNTech/Pfizer 1st Maculopapular pruritic generalized rash, starting from injection site None reported Correlated 8 35 F 72 h Moderna 1st Maculopapular pruritic generalized rash Nausea, dyspnea, headache, vertigins Correlated 9 27. F 10 days Oxford-AstraZeneca 1st Macular pruritic generalized rash (especially on neck, wrists, arms) Headache Correlated 10 43 F 10 days BioNTech/Pfizer 1st Urticarial pruritic generalized rash (especially on eyelids and arms) None reported Correlated 11 44 F 15 days BioNTech/Pfizer 1st Macular pruritic generalized rash with erythematous patches on the elbows None reported Correlated 12 59 F 15 days BioNTech/Pfizer 2nd Lichen planus plaques on both feet and ankles None reported Correlated 13 56 M 16 days BioNTech/Pfizer 2nd Psoriasis plaques on the trunk and limbs None reported Correlated 14 53 F 72 h BioNTech/Pfizer 1st Cutaneous sarcoidosis of the nose, eyelids, cheek Dyspnea and pulmonary sarcoidosis Correlated 15 58 F 20 days BioNTech/Pfizer 2nd Herpes Zoster, crural Headache, asthenia Correlated 16 82 F 20 days BioNTech/Pfizer 2nd Herpse Zoster, cervical Generalized arthralgia and myalgia, asthenia, local dysesthesia Correlated 17 37 F 30 days Oxford-AstraZeneca 2nd Herpse Zoster, facial Flu-like symptoms Correlated 18 31 M 30 days BioNTech/Pfizer 2nd Pityriasis Rosea, diffuse, only mildly pruritic Headache, asthenia Correlated 19 42 F 4 days BioNTech/Pfizer 2nd Ecchymosis on the third finger of the left foot Headache, otalgia Noncorrelated 20 54 F 24 h BioNTech/Pfizer 2nd Eruptive angiomas of trunk and arms None reported Noncorrelated 21 80 F 24 h Oxford-AstraZeneca 2nd Giant seborrheic keratosis None reported NoncorrelatedOf these, 15 (71%) were females, with a mean age of 48 years, 6 (29%) were males, with a mean age of 62 years.
Female gender was not significantly more associated to reactions to the vaccine (4%, 15/116) than male gender (7%, 6/84) (p value >.05 calculated with Fisher exact test).
BioNTech/Pfizer was the most frequently reported vaccine used (62%, 13/21).
Reactions were more frequently reported after the second dose of vaccine (57%, 12/21) and occurred from 3 h to 30 days after vaccination. One patient out of 21, after the second dose of Moderna vaccine, developed a bullous erythema multiforme, which required hospitalization (Figure 1).

Severe diffuse bullous erythema multiforme with rapidly occurring and evolving, intensely red, round macules and papules, widely coalescing into large plaques and developing epidermal blistering
Ten of 21 patients developed macular-papular or urticarial reactions (Figure 2). In 4 patients out of 10, it appeared within 24 h of vaccine, in 6 patients after 24 h. Four out of 10 patients reported headaches associated with the rash. Two out of 10 patients reported nausea; only one had dizziness. The reaction developed after the first dose of vaccine in 6 of 10 patients.3

Urticarial reaction of the upper limbs and chest, characterized by small wheals with an erythematous rim and a pale center
Three out of 21 patients developed herpes zoster (HZ) 20 days after vaccination, associated with severe asthenia (Figure 3). None of the patients observed reported previous HZ. Only one patient out of 21 developed a diffuse form of pityriasis rosea of Gibert, only modestly itchy and associated with asthenia, after receiving the second dose of Pfizer vaccine.

Mild localized unilateral Herpes Zoster, erythematous, blistering and painful rash caused by reactivation of varicella-zoster virus, characterized by dermatomal distribution
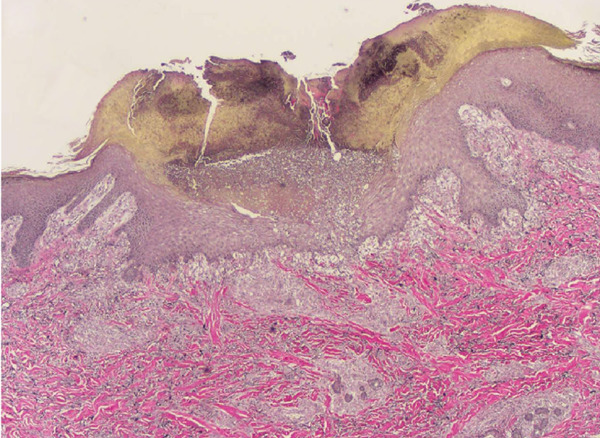
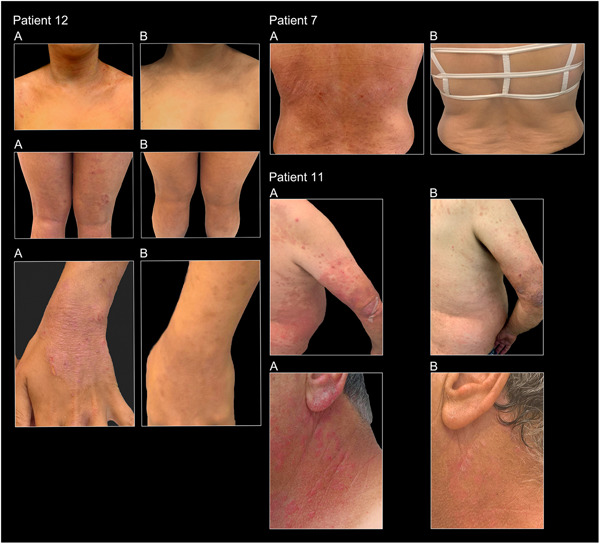
One patient reported the appearance of orange plaques on the nose, eyebrows and cheeks 72 h after administration of the first dose of Pfizer. A biopsy was performed and a diagnosis of sarcoidosis was made. One patient experienced a flare of lichen planus plaques4, 15 days after the second dose of Pfizer and one patient experienced recurrence of psoriatic plaques, 16 days after the second dose of Pfizer (Figure 4).

Recurrence of multiple psoriatic plaques, scaly, erythematous and slightly infiltrated, disseminated on the back
One patient out of 21 reported ecchymosis on the third toe of the left foot, 4 days after administration of Pfizer vaccine. One patient reported eruptive angiomas of the trunk and arms, which appeared within 24 h after the second dose of Pfizer vaccine. An 80-year-old patient claimed the appearance of a giant seborrheic keratosis within 24 h after the second dose of Pfizer vaccine.
4 DISCUSSIONSince COVID-19 vaccination is spreading, there have been numerous reports of adverse reactions to the vaccine.5-13 The fear of the vaccine in the population is not justified, since many supposed reactions to the vaccine are in fact not due to it.5, 6 In our sample, only one of the 21 patients reporting skin reactions required hospitalization for generalized bullous erythema multiforme, which occurred 48 h after the second Moderna vaccine dose. Erythema multiforme is an immune-mediated muco-cutaneous inflammatory condition, which has been already reported in association with COVID-19 and COVID-19 vaccination, possibly caused by vaccine components eliciting an immune dysregulation, leading to a T-lymphocyte auto-immune response directed against keratinocytes, causing cell death and dermo-epidermal junction detachment.14
Fortunately, none of the other patients developed life-threatening reactions.
Ten out of 21 developed macular or urticarial rashes, which resolved with antihistamine or spontaneously, similarly to cases reported in the literature.2-6 Two patients presented generalized pruritic rash shortly after vaccination (≤4 h), possibly representing immediate hypersentivity type I reactions against vaccine excipients.2-6
Other rapid reactions reported were one pruritic generalized rash and a facial swelling and flushing, which occurred ≤24 h, but >4 h after vaccination, probably representing nonallergic (non-immunoglobulin E mediated) but pseudo-allergic reactions considering the time of occurrence.5-8
The other 6 macular-papular/urticarial reactions reported, occurred >48 h after vaccination, probably representing a delayed hypersensitivity (Coombs and Gell type IV) reactions.8-10
Though initially rarely observed during clinical approval studies, these hypersensitivity reactions seem now to be a well described phenomenon after COVID-19 vaccination.1 Indeed, McMahon et al.8 reported in a recent study delayed large local reactions as the most frequent among cutaneous findings after messenger RNA (mRNA) COVID-19 vaccinations (BioNTech/Pfizer and Moderna).
Of note, it must be considered that the rash may also represent an immune response to spike protein, as similar morbilliform eruptions that are negative for viral particles have been observed in patients with primary COVID-19 infection.15
HZ virus reactivations were reported in 3 patients with a latency ≥20 days from vaccination, conceivably due to nonallergic vaccine immune dysregulation.7
All HZ cases reported in literature, following COVID-19 vaccination, and our three cases, were moderate-to-mild cases and were successfully treated with antiviral therapy.8, 16, 18
Though the precise mechanisms involved in HZ development following COVID-19 vaccinations are still unknown, the increasing reports of HZ reactivation after mRNA-based and adenovirus-based COVID-19 vaccine call upon further studies.817-20
Also, Pityriasis rosea (PR) (-like) eruptions have been described after COVID-19 vaccination. These may be secondary to a T-cell-mediated response, triggered by molecular mimicry from a viral epitope, or secondary to endogenous systemic reactivation of human herpes virus (HHV)-6 and/or HHV-7.19-24 Of note, PR eruptions have been already described following other types of vaccinations, such as influenza vaccination with detection of HHV-6 and HHV-7 in skin biopsies.19-23
In our patient it occurred 30 days from the second dose of BioNTech/Pfizer and lasted approximately 35 days.
Interestingly, three patients presented exacerbation of their cutaneous diseases, including a flare of lichen planus, psoriasis and sarcoidosis, already present, and worsened, possibly induced by the vaccine.25
Last, three patients presented lesions that were discarded as not related to vaccination.
Indeed, seborrheic keratosis, eruptive angiomas, acral ecchymoses were interpreted as likely unrelated to the COVID-19 vaccination and no literature reports were found to support possible causal associations.25
5 CONCLUSIONDespite the limitations of its descriptive and retrospective design, our study reports that cutaneous reactions to vaccination do not represent a contraindication to undergo COVID-19 vaccination. These data are in line with the literature so far collected, although we did not record in our patients the most common reported reactions in the literature following COVID-19 vaccines, i.e., local (early- or late-onset) reactions and chilblain-like lesions. This could possibly be the result of a selection bias, as the present study retrospectively assessed patients admitted at the Dermatology Primary Care.
Of note, cutaneous reactions considered worrisome by patients are mostly only mild or moderate, or not even associated with COVID-19 vaccination, possibly suggesting patients are just apprehensive about anything they note after vaccination.
However, awareness must be raised to recognize and treat eventual severe reactions. As worldwide vaccination efforts are being adopted against COVID-19, it is important for healthcare providers to recognize possible adverse events.
FUNDING INFORMATIONFunding information is not available.
CONFLICT OF INTERESTSThe authors declare that there are no conflict of interests.
AUTHOR CONTRIBUTIONSMartina Burlando, Astrid Herzum, and Claudia Micalizzi: performed the research. Martina Burlando, Astrid Herzum, Claudia Micalizzi, Emanuele Cozzani, and Aurora Parodi: designed the research study and revised the final version of the paper. Martina Burlando, Astrid Herzum, and Emanuele Cozzani: analyzed the data and wrote the paper. All authors have read and approved the final manuscript.
REFERENCES
1 CDC COVID-19 Response Team. Food and Drug Administration. Allergic reactions including anaphylaxis after receipt of the first dose of Pfizer-BioNTech COVID-19 vaccine - United States, December 14-23, 2020. MMWR Morb Mortal Wkly Rep. 2021; 70: 46- 51. doi:10.15585/mmwr.mm7002e1 2Chung EH. Vaccine allergies. Clin Exp Vaccine Res. 2014; 3: 50- 57. doi:10.7774/cevr.2014.3.1.50 3Burlando M, Herzum A, Cozzani E, Parodi A. Acute urticarial rash after COVID-19 vaccination containing Polysorbate 80. Clin Exp Vaccine Res. 2021; 10: 298- 300. doi:10.7774/cevr.2021.10.3.298 4Herzum A, Burlando M, Molle MF, et al. Lichen planus flare following COVID-19 vaccination: a case report. Clin Case Rep. 2021:e5092. doi:10.1002/ccr3.5092 5Kim MA, Lee YW, Kim SR, et al. COVID-19 vaccine-associated anaphylaxis and allergic reactions: consensus statements of the KAAACI Urticaria/Angioedema/Anaphylaxis Working Group. Allergy Asthma Immunol Res. 2021; 13: 526- 544. doi:10.4168/aair.2021.13.4.526 6Kounis NG, Koniari I, de Gregorio C, et al. Allergic reactions to current available COVID-19 vaccinations: pathophysiology, causality, and therapeutic considerations. Vaccines (Basel). 2021; 9:221. doi:10.3390/vaccines9030221 7Banerji A, Wickner PG, Saff R, et al. mRNA vaccines to prevent COVID-19 disease and reported allergic reactions: current evidence and suggested approach. J Allergy Clin Immunol Pract. 2021; 9: 1423- 1437. doi:10.1016/j.jaip.2020.12.047 8McMahon DE, Amerson E, Rosenbach M, et al. Cutaneous reactions reported after Moderna and Pfizer COVID-19 vaccination: a registry-based study of 414 cases. J Am Acad Dermatol. 2021; 85: 46- 55. doi:10.1016/j.jaad.2021.03.092 9 Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Authorized in the United States. Centers for Disease Control and Prevention. Accessed July 25, 2021. Available at: https://www.cdc.gov/vaccines/covid-19/clinical-considerations/covid-19-vaccines-us.html 10Johnston MS, Galan A, Watsky KL, Little AJ. Delayed localized hypersensitivity reactions to the moderna COVID-19 vaccine: a case series. JAMA Dermatol. 2021; 157: 716- 720. doi:10.1001/jamadermatol.2021.1214 11Jedlowski PM, Jedlowski MF. Morbilliform rash after administration of Pfizer-BioNTech COVID-19 mRNA vaccine. Dermatol Online J. 2021; 27(1). doi:10.5070/D3271052044 12Mahmood F, Muntyanu A, Besner Morin C, Litvinov I, Isabwe GAC, Netchiporouk E. Delayed cutaneous reactivity associated with COVID-19 vaccines is rare. J Cutan Med Surg. 2021; 25(5): 557- 559. doi:10.1177/12034754211027854 13Baden LR, El Sahly HM, Essink B, et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med. 2021; 384: 403- 416. doi:10.1056/NEJMoa2035389 14Lavery MJ, Nawimana S, Parslew R, Stewart L. A flare of pre-existing erythema multiforme following BNT162b2 (Pfizer-BioNTech) COVID-19 vaccine. Clin Exp Dermatol. 2021; 46: 1325- 1327. doi:10.1111/ced.14714 15Ghimire K, Adhikari N. Morbilliform rashes in a patient with COVID-19 infection: a case report. JNMA J Nepal Med Assoc. 2021; 59: 399- 401. doi:10.31729/jnma.5128 16Psichogiou M, Samarkos M, Mikos N, Hatzakis A. Reactivation of Varicella Zoster Virus after Vaccination for SARS-CoV-2. Vaccines (Basel). 2021; 9:572. doi:10.3390/vaccines9060572 17Aksu SB, Öztürk GZ. A rare case of shingles after COVID-19 vaccine: is it a possible adverse effect? Clin Exp Vaccine Res. 2021; 10: 198- 201. doi:10.7774/cevr.2021.10.2.198 18Chiu HH, Wei KC, Chen A, Wang WH. Herpes zoster following COVID-19 vaccine: report of 3 cases. QJM. 2021; 114: 531- 532. doi:10.1093/qjmed/hcab208 19Cyrenne BM, Al-Mohammedi F, DeKoven JG, Alhusayen R. Pityriasis rosea-like eruptions following vaccination with BNT162b2 mRNA COVID-19 Vaccine. J Eur Acad Dermatol Venereol. 2021; 13: 546. doi:10.1111/jdv.17342 20Drago F, Herzum A, Ciccarese G, Broccolo F, Rebora A, Parodi A. Acute pain and postherpetic neuralgia related to Varicella zoster virus reactivation: comparison between typical herpes zoster and zoster sine herpete. J Med Virol. 2019; 91: 287- 295. doi:10.1002/jmv.25304 21Papakostas D, Stavropoulos PG, Papafragkaki D, Grigoraki E, Avgerinou G, Antoniou C. An Atypical case of pityriasis rosea gigantea after influenza vaccination. Case Rep Dermatol. 2014; 6: 119- 123. 22Drago F, Ciccarese G, Parodi A. Pityriasis rosea and pityriasis rosea-like eruptions: how to distinguish them? JAAD Case Rep. 2018; 4: 800- 801. doi:10.1016/j.jdcr.2018.04.002 23Ciccarese G, Parodi A, Drago F, Herzum A, Drago F. Pityriasis rosea in a patient with retrovirus infection: a reply. Postepy Dermatol Alergol. 2018; 35: 116- 117. doi:10.5114/ada.2018.73172 24Rebora A, Ciccarese G, Herzum A, Parodi A, Drago F. Pityriasis rosea and other infectious eruptions during pregnancy: possible life-threatening health conditions for the fetus. Clin Dermatol. 2020; 38(1): 105- 112. 25Bauckneht M, Aloè T, Tagliabue E, et al. Beyond Covid-19 vaccination-associated pitfalls on [18F]Fluorodeoxyglucose (FDG) PET: a case of a concomitant sarcoidosis. Eur J Nucl Med Mol Imaging. 2021; 48: 482661- 482662. doi:10.1007/s00259-021-05360-w
Comments (0)