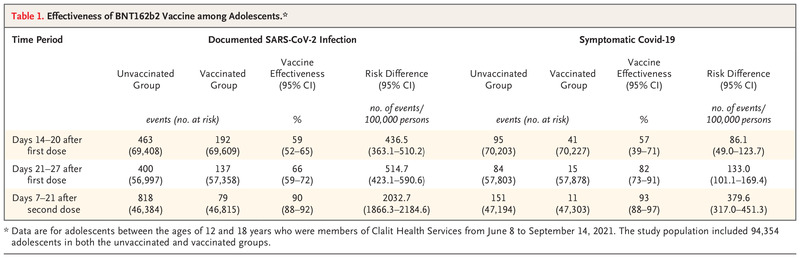
Dr. Hanno Hock: I participated in the care of this patient, and I am aware of the diagnosis. This 21-year-old man had been in excellent health until the week of admission, when oropharyngeal and cutaneous bleeding developed. On presentation, the severely decreased platelet count explained the bleeding. The very low total white-cell count and absolute neutrophil count indicated that he was at risk of infection. The only moderately decreased hematocrit suggested that he did not have long-standing severe anemia, but the absence of reticulocytes showed that red-cell production was profoundly impaired. Because he tested positive for SARS-CoV-2 RNA, could this patient’s cytopenias be related to SARS-CoV-2 infection?
Patients with SARS-CoV-2 infection and an acute febrile illness often have blood abnormalities such as pancytopenia,1-3 which are sometimes triggered by hemophagocytic lymphohistiocytosis.4,5 However, this patient did not have a febrile illness. In the absence of illness, his positive SARS-CoV-2 test could be indicative of the presymptomatic incubation period of SARS-CoV-2 infection, asymptomatic active infection, or shedding of RNA after asymptomatic infection. However, none of these circumstances have been associated with major blood abnormalities. Therefore, we needed to consider the wide spectrum of causes of pancytopenia.
Sickle Cell Trait
This patient did not use medications, illicit drugs, or alcohol and had normal levels of vitamin B6 and vitamin B12. These features rule out several common causes of cytopenia. Patients with sickle cell disease are at risk for aplastic crisis, which is an acute decrease in the red-cell count that often occurs after parvovirus B19 infection.6 This patient was a carrier of sickle cell trait but was not at risk for the major complications of sickle cell disease.7 Although sickle cell trait is associated with some health risks8 and should be considered as a potential factor contributing to poor outcomes among Black patients with Covid-19,9 it has not been linked to pancytopenia.7
Increased Cell Destruction
Pancytopenia can result from several conditions that cause increased cell destruction. Cells may pool in an enlarged spleen or be destroyed by the splenic reticuloendothelial system, but this patient did not have splenomegaly. Evans syndrome — a combination of immune thrombocytopenic purpura, autoimmune hemolytic anemia, and immune neutropenia — causes pancytopenia from peripheral destruction.10 Immune thrombocytopenic purpura has recently been reported in association with Covid-19.4 However, this patient did not have evidence of hemolysis or compensatory reticulocytosis, which would be expected in a patient with Evans syndrome. Hemophagocytic lymphohistiocytosis can be triggered by numerous infectious agents other than SARS-CoV-2, including Epstein–Barr virus and cytomegalovirus,5 but this patient did not have signs of infection or inflammation.
Decreased Cell Production
Infection can impair cell production through various mechanisms.11,12 Parvovirus B19,13 hepatitis C virus,14 human herpesvirus 6,15 human herpesvirus 7,16 cytomegalovirus,17 and the human immunodeficiency virus (HIV)18 can directly infect hematopoietic stem cells and progenitor cells. Cytomegalovirus, HIV, and coxsackievirus B can infect bone marrow stromal cells and suppress cell production,11 but this usually occurs in patients who have a chronic condition, take an immunosuppressive medication, or have overt signs of infection. Many pathogens suppress cell production indirectly, through cytokine release and inflammation.11 Respiratory viruses such as influenza A, influenza B, rhinovirus, and SARS-CoV-2 can cause transient cytopenias in ill patients, but this patient did not have a fever and was otherwise well.1,19
Cancer
Lymphoma, myeloma, leukemia, and myelodysplastic syndromes can cause pancytopenia by replacing normal hematopoietic stem cells with malignant cells. Leukemia can be aleukemic, without leukemic blasts in the blood. The presentation of myelodysplastic syndromes in children and young adults may be different from that in older adults; younger patients more often have hypocellular bone marrow, which makes it harder to differentiate the condition from aplastic anemia.20-23 In addition, paroxysmal nocturnal hemoglobinuria, a clonal disorder that initially manifests as hemolytic anemia because of complement-mediated destruction, may cause pancytopenia in the late stages.24 However, the absence of constitutional symptoms, sudden onset of bleeding, and nearly complete absence of cell production made cancer and paroxysmal nocturnal hemoglobinuria unlikely diagnoses in this case.
Aplastic Anemia
Aplastic anemia is characterized by pancytopenia and the loss of hematopoietic stem cells, progenitor cells, and precursor cells in the bone marrow.25,26 It was the most likely diagnosis in this previously healthy patient with pancytopenia in the absence of constitutional symptoms and abnormal cells. Aplastic anemia results from one of three main mechanisms25: damage by extrinsic factors, manifestations of familial genetic mutations, and autoimmune attack on hematopoietic stem cells and progenitor cells.
Extrinsic causes of aplastic anemia are usually obvious and include major accidental or therapeutic exposure to radiation, chemotherapy, or massive exposure to benzene25 or pesticides such as organochlorines and organophosphates.27Several medications have been infrequently associated with aplastic anemia.27,28 However, this patient was not taking any medications and had no known chemical or radiation exposures.
The genetic disorder most commonly associated with aplastic anemia is Fanconi’s anemia, a DNA repair defect that results from a mutation in 1 of at least 15 known genes.29 Patients with Fanconi’s anemia typically have bone marrow failure in the first or second decade of life, as well as other congenital abnormalities, including thumb and facial deformities and short stature.29 The second most common genetic cause of bone marrow failure is dyskeratosis congenita, which is due to mutations in genes involved in telomere repair or protection.30 Dyskeratosis congenita typically manifests in childhood with skin pigmentation abnormalities, oral leukoplakia, and dystrophic nails. However, the disease may cause isolated bone marrow failure.31 Finally, GATA2 mutations have emerged as a potential genetic cause of aplastic anemia.32 These mutations are associated with other manifestations, including lymphedema, generalized warts from human papillomavirus infection, and mycobacterial infection.23 This patient’s pancytopenia was unlikely to be caused by a congenital genetic abnormality because he had no family history of such a condition and no associated signs or symptoms.
Up to 70% of cases of aplastic anemia occur sporadically, resulting from the sudden onset of T-cell–mediated destruction of hematopoietic stem cells and progenitor cells.28 Most cases of aplastic anemia are designated as idiopathic because the triggers for the immune attack on hematopoiesis are obscure. There are known associations with thymoma33 and eosinophilic fasciitis.34 However, both these diseases develop predominantly in the seventh decade of life, and this patient did not have the widened mediastinum on chest radiography that is suggestive of thymoma or the dimpled skin thickening (peau d’orange change) that is suggestive of eosinophilic fasciitis.34
The most common known trigger for aplastic anemia is seronegative hepatitis, which precedes 5 to 10% of cases of aplastic anemia by approximately 2 to 3 months.35,36 The median age at the onset of hepatitis-associated aplastic anemia is 20 years, but this patient’s history did not suggest recent hepatitis. Aplastic anemia is also thought to occur after infection with common hepatitis viruses37 and other viruses, including HIV and parvovirus B19,12,38,39 but at a much lower frequency than with seronegative hepatitis.
It is intriguing that this patient’s exposure to SARS-CoV-2 and probable asymptomatic infection occurred 2 months before his presentation, an interval similar to that between the onset of seronegative hepatitis and the development of aplastic anemia; therefore, it is tempting to speculate that SARS-CoV-2 infection may have been a trigger. However, his presentation and age also fit with idiopathic aplastic anemia, which has an incidence of 2 to 3 cases per 1 million per year.27 Given the scale of the Covid-19 pandemic, a potential association may eventually be confirmed if the incidence of aplastic anemia rises. Regardless of the trigger, this patient’s presentation and blood abnormalities were highly suggestive of aplastic anemia, a diagnosis that must be confirmed with evidence of markedly reduced hematopoiesis in a bone marrow–biopsy specimen. The severity of aplastic anemia is determined by the degree of the associated peripheral-blood cytopenias.28,40,41 The near absence of platelets, neutrophils, and reticulocytes in this case was associated with a high risk of death and a very low chance of recovery without urgent treatment and consideration of bone marrow transplantation.





Comments (0)