
Remember me



Chronotype preference has emerged as a significant vulnerability factor in mental health. While not a clinical diagnosis itself, eveningness is consistently associated with a higher prevalence and greater severity of psychiatric symptoms, including mood disturbances, anxiety, attentional difficulties, and emotional dysregulation [1,2,3, 5,6,−7, 29].
In our recent analysis of more than 70,000 middle-aged and older adults in the United Kingdom (UK Biobank cohort), we found that self-reported evening chronotype preference was associated with a significantly higher prevalence of major depressive disorder, generalized anxiety disorder, and other psychiatric conditions [3]. Notably, these associations extended beyond cross-sectional patterns: survival analysis showed that evening types had a higher risk of developing these disorders over time, underscoring eveningness as a potential risk factor for future psychopathology [3]. These findings are supported by other studies demonstrating a consistent relationship between eveningness and elevated depressive symptoms [20]. This vulnerability is not limited to adults– a systematic review in youths found that eveningness was significantly associated with general mental health problems, mood-related disturbances, anxiety, increased risk for psychotic symptoms, and maladaptive eating behaviors [30]. Eveningness in students has also been linked to more frequent and severe feelings of defeat and entrapment, as well as suicidal ideation [31].
Association of Psychiatric Disorders with the Timing of BehaviorWhile chronotype preference provides valuable insights into mental health risk, emerging evidence suggests that the actual timing of behavior—when individuals habitually go to sleep and wake up—may be an even stronger predictor of psychiatric outcomes. Behavioral timing reflects the lived expression of sleep–wake rhythms and captures the combined influence of biological, social, and environmental factors.
In our analyses of the UK Biobank, we also examined objectively (actigraphy) measured sleep–wake timing to assess their independent associations with psychiatric outcomes [3]. We found that, as with chronotype, later behavioral timing was consistently linked to a higher prevalence of conditions such as depression, anxiety, and broader categories of mental and behavioral disorders. Crucially, this association persisted even after adjusting for chronotype preference, suggesting that actual sleep–wake patterns may exert a direct influence on psychiatric risk, independent of chronotype [3]. While later sleep timing is often associated with shorter sleep, individuals with later sleep timing had an increased risk for psychiatric disorders regardless of how much sleep they obtained, indicating that sleep quantity is not the sole driver of this association [32, 33].
Additional recent studies support these findings. In a community-based sample of older adult women, later sleep timing was associated with both depressive symptoms and an increased likelihood of surpassing the clinical threshold for depression, independent of sleep duration [34]. Similarly, a systematic review of pediatric populations found that later sleep timing in children and adolescents was linked to poorer emotional regulation, lower academic performance, and reduced cognitive functioning [35]. Evidence from forensic psychiatric populations further underscores this pattern [36]. Individuals in these settings are more likely to exhibit later behavioral timing than the general population, with the strongest evening preferences observed among those diagnosed with personality disorders [36].
A central theory of circadian research is that misalignment—a mismatch between an individual’s preferred sleep-wake timing and their actual behavioral schedule—is detrimental to mental health [37]. Misalignment has been linked to mood disturbances, metabolic dysfunction, impaired cognition, and increased psychiatric vulnerability [37,38,39]. Circadian misalignment can result from rigid schedules that force individuals to operate out of synchrony with their natural preferences, often leading to chronic sleep restriction, daytime fatigue, and elevated stress. Theoretically, aligning behavior with preference should mitigate these outcomes.
However, our findings—and those of others—suggest that synchrony between chronotype preference and behavior may not be the most decisive factor in determining mental health outcomes. While circadian misalignment is linked to poorer mental health outcomes, the timing of behavior itself appears to be a stronger and more consistent predictor of psychiatric risk [3]. While individuals with an evening preference who maintain a sleep schedule aligned with their internal clock still show elevated rates of depression, anxiety, and related disorders if their sleep–wake timing is late, evening individuals who maintain earlier sleep timing have lower rates [3].
This distinction highlights a key insight: it is not just the mismatch that matters, but the timing itself. While alignment between preference and behavior may offer some buffering effects, it does not eliminate the risks linked to late sleep-wake timing. Therefore, interventions to reduce psychiatric vulnerability should not only aim to reduce misalignment but also consider shifting behavioral timing earlier when feasible, regardless of chronotype.
These findings highlight an important, yet still unresolved, question: why is being awake late so detrimental to mental health? Unpacking the biological, environmental, and psychosocial mechanisms at play will be crucial for developing more targeted and personalized approaches to prevention and treatment.
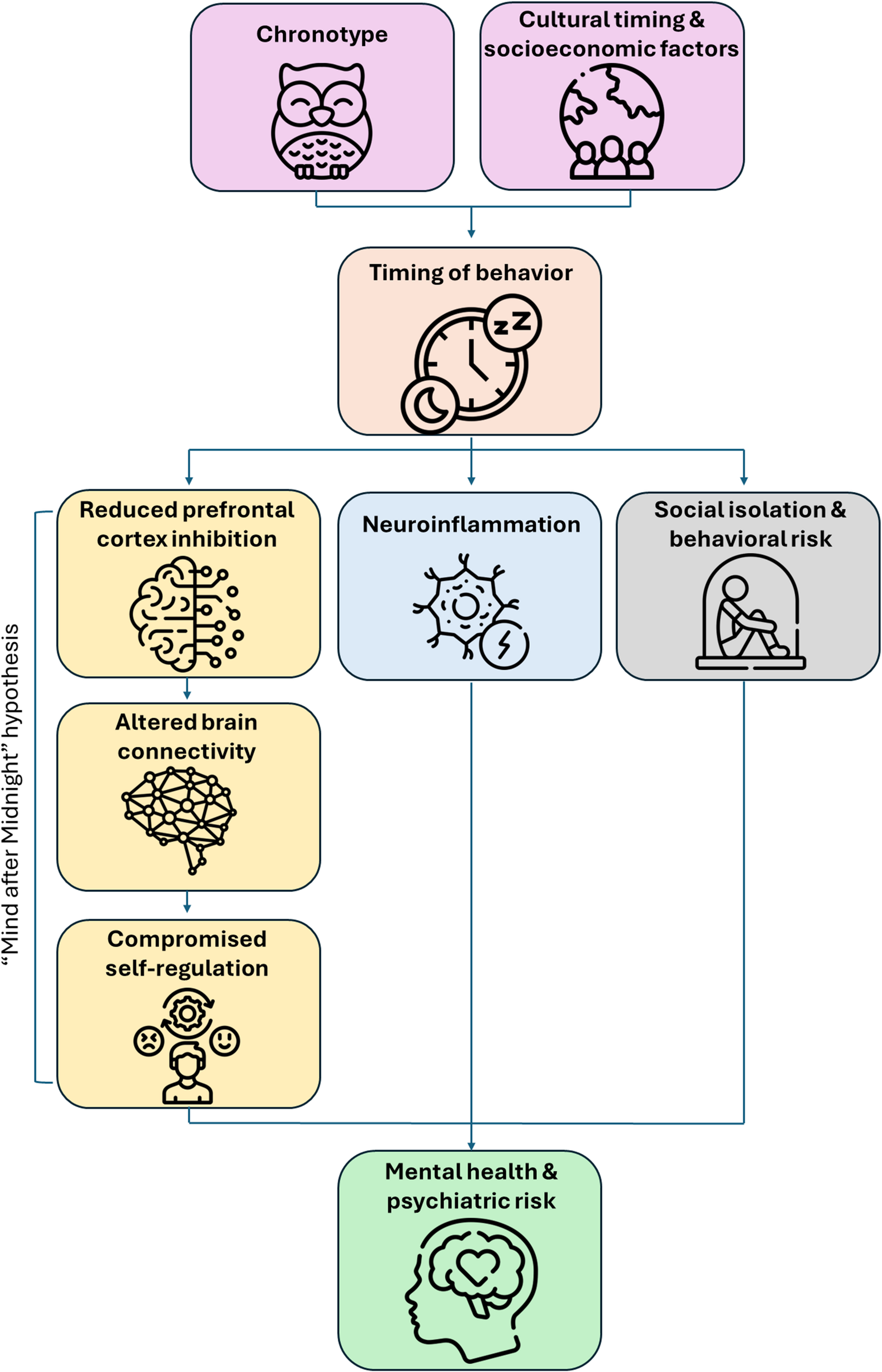
What about Staying Up Late is Bad for You?While the association between later sleep timing and worse psychiatric outcomes is well-documented, the underlying mechanisms remain poorly understood. Several non-exclusive factors may contribute to the increased vulnerability associated with being awake late at night, though these are all hypothetical at this point. Among the most likely factors involved in the association between being awake late at night and poor mental health outcomes are circadian misalignment, sleep loss, behavior, and light exposure (Fig. 1).
(1) Circadian misalignment. When some individuals stay awake late into the night, they are awake during a time at which the circadian clock is expecting sleep, the “biological night.” Staying awake during the biological night creates a mismatch between internal physiology and external demands that can have negative consequences on mood [40]. However, not everyone who goes to bed late is necessarily awake during their biological night; individuals with a delayed circadian phase may remain aligned with their internal clock despite a late schedule [22, 23].
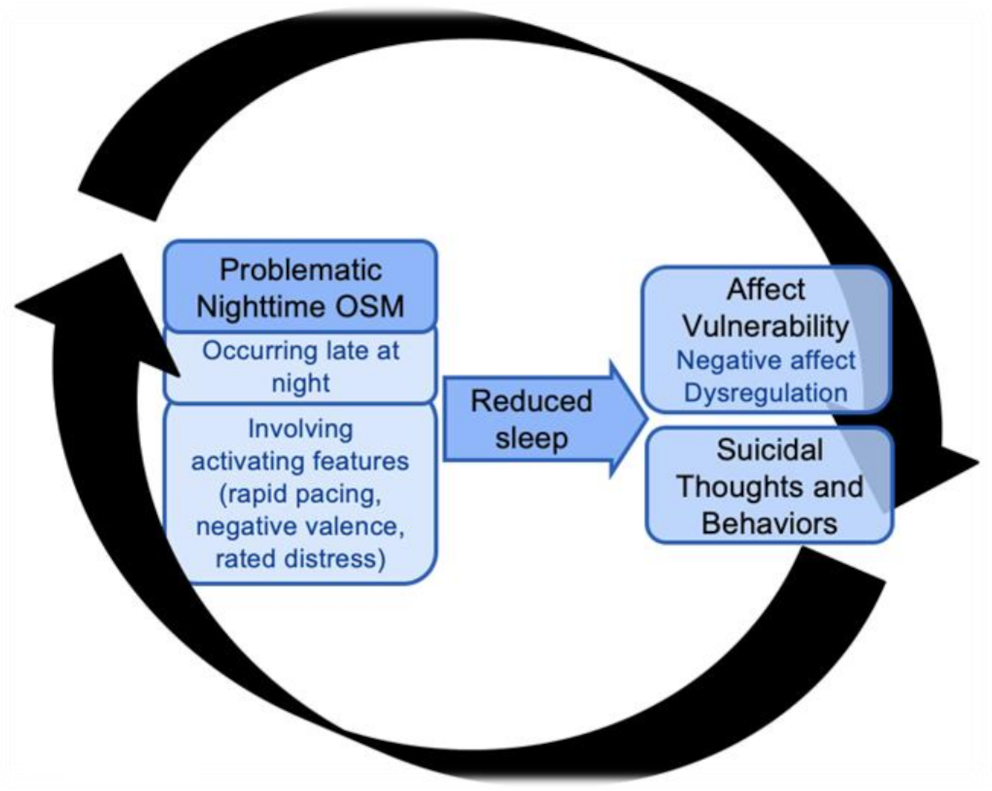
(2) Sleep loss. Sleep loss disrupts neural communication and impairs emotional and cognitive regulation [41]. When periods of extended wake are coupled with circadian misalignment, it may create a uniquely vulnerable state, conceptualized as the “Mind After Midnight,” characterized by reduced cortical activity, altered connectivity, and compromised self-regulation [42]. During this state, emotional reactivity is heightened, and attention becomes biased toward negative or ambiguous information. This may be due to increased amygdala activity in the absence of the regulatory influence typically exerted by prefrontal regions during the day [42]. Simultaneously, changes in the brain’s reward circuitry may emerge. Neurochemical shifts, particularly involving dopamine, alter the sensitivity and balance of reward processing systems. Increased activity in regions like the ventral striatum (nucleus accumbens region) is paired with reduced engagement of the dorsal striatum (caudate and putamen), leading to a state in which the anticipation of reward is amplified, even as actual satisfaction is diminished. This neural profile may explain why late-night wakefulness is linked to increased impulsivity, risk-taking, and vulnerability to maladaptive behaviors [42].
(3) Behavior. Being awake late at night often occurs in social isolation, with limited access to supportive interactions, a key protective factor against mental health challenges. While individuals with an evening chronotype report significantly higher levels of loneliness and lower perceived social support, both established risk factors for depression and anxiety, comparable data are lacking for actual sleep–wake timing [44]. Thus, the psychosocial consequences of late behavioral timing remain an important but underexplored area of research. While individuals who rise early in the morning, and who have a lower burden of mental health disorders, also have a similar social isolation, there may be unique factors associated with late night social isolation, including different levels of homeostatic sleep pressure, the burden of a day’s worth of stress and anxiety, and difference in natural illuminance. Whether these factors contribute to the interaction of late-night behavior and social isolation is unknown.
(4) Light. Association studies have linked artificial indoor light exposure and adverse mental health outcomes in several large epidemiological studies [45, 46]. These studies, however, provide limited mechanistic evidence that the illuminance of nocturnal light to which individuals are exposed and have differential mental health outcomes are physiologically relevant [47]. For example, one recent study claimed that different mental health outcomes were associated with wrist actigraph-recorded illuminances of 0.5 lx, 0.8 lx, and 3.0 lx [46], all of which are far below the published sensitivity thresholds of hypothalamus-mediated light responses [48, 49]. The association between nocturnal light and mental health is more likely mediated by the behavior that light enables rather than a direct physiologic effect. Even dim indoor artificial light may allow for engagement in stimulating or emotionally charged activities, such as scrolling through social media [50], or engaging in less mental-health-promoting activities like drinking alcohol [51]. These behaviors can extend wakefulness and disrupt emotional regulation [50, 51].
Many epidemiological studies have also associated outdoor artificial light at night (ALAN) with negative mental health outcomes [52,53,54]. From a human physiology perspective, ALAN levels in residential areas are typically low, and the use of curtains, blinds, or other forms of indoor light shielding further reduces actual exposure to ALAN. As a result, most individuals encounter only minimal levels of outdoor light at night, making the direct physiological impact on mental health likely negligible. In addition, ALAN is highly confounded by urbanization: areas with higher outdoor light levels also tend to exhibit other features, such as noise pollution, higher population density, reduced green space, socioeconomic inequality, and increased nighttime activity, all of which can independently contribute to poor mental health outcomes [55, 56].
(5) Other considerations. It is essential to consider both economic and social factors in relation to the relationship between behavioral timing and mental health. Early bedtimes are associated with contextual and socioeconomic factors that may impact health. For instance, adolescents with earlier bedtimes often come from lower-resource environments and have reduced access to digital devices, the internet, and extracurricular activities [57]. Conversely, later bedtimes in youth are often associated with greater access to screens [58] and more autonomy over evening routines [59]. In adults, shift work [60], crowded living conditions, or caregiving responsibilities [61, 62] may also delay sleep timing, particularly in socioeconomically disadvantaged populations. These contextual influences can confound the relationship between sleep timing and mental health and may partially explain why late timing is more prevalent in certain demographic groups. Therefore, interpretations of behavioral timing must be situated within a social determinants of health framework, especially when assessing psychiatric risk in youth, underserved communities, or marginalized populations. Future research should actively examine how structural inequities, such as housing instability and occupational demands, intersect with sleep behaviors to shape health outcomes.
Fig. 1
Conceptual model linking timing of behavior to psychiatric risk through multiple independent pathways. Chronotype and cultural/socioeconomic context (purple) shape the timing of behavior (orange), defined as the habitual timing of the sleep–wake schedule. Timing of behavior, in turn, influences downstream moderating mechanisms, including nocturnal vulnerability through reduced prefrontal cortex inhibition, altered brain connectivity, and compromised self-regulation (“the mind after midnight”, yellow), and neuroinflammation (blue). It may also contribute to mental health risk through social isolation and behavioral risk factors (grey), although empirical data directly linking these pathways to behavioral timing are currently limited. These pathways independently contribute to mental health and psychiatric risk (green). Arrows indicate proposed directional relationships based on current evidence. The model emphasizes the importance of both upstream contextual factors and downstream biological and psychosocial mechanisms in shaping psychiatric vulnerability
Comments (0)