
Remember me
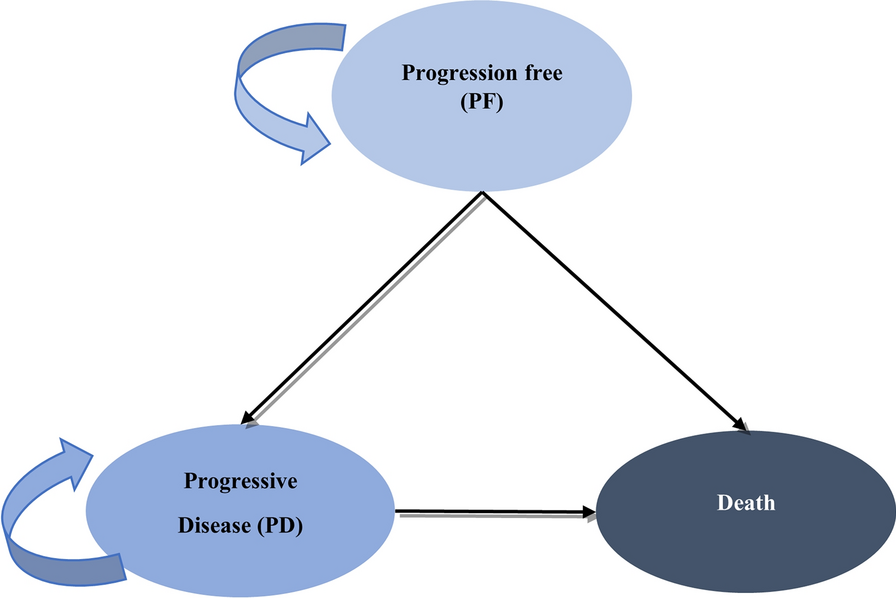
A partitioned survival model with a 28-day cycle length was developed in Microsoft Excel 2016 (Microsoft Corporation; Redmond, WA) to compare the cost-effectiveness of brigatinib versus alectinib as first-line treatment for patients with ALK-positive NSCLC in China. This model included three health states: progression-free (PF), progressive disease (PD), and death (Fig. 1).
Fig. 1
The average age of patients in the ALTA-1L study of brigatinib was 58 years [12], and the life expectancy of Chinese people is 78.2 years [13]. Thus, the time horizon was set as 30 years as a proxy for lifetime. Costs and quality-adjusted life years (QALYs) were discounted at an annual rate of 5%, according to China guidelines for pharmacoeconomic evaluations (2020) [14]
Clinical DataThe efficacy of brigatinib was modeled on the basis of progression-free survival (PFS) as assessed by the independent review committee (IRC) and overall survival (OS) obtained from the final results of the ALTA-1L trial [15]. Seven survival distributions were considered to fit and extrapolate the PFS and OS from the ALTA-1L trial: Exponential, Weibull, Log-normal, Gamma, Log-logistic, Gompertz, Gen. Gamma (Supplementary Figs. 1 and 2). The exponential distribution was chosen, consistent with a previously published cost-effectiveness analysis of brigatinib conducted from the payer perspective in the USA [16]. Treatment duration was set consistent with the label instructions for brigatinib and alectinib in China to administer treatment until disease progression [17, 18].
There are no head-to-head trials between brigatinib and alectinib in first-line treatment, so the clinical data from published indirect treatment comparisons (ITC) were considered in this study. The relative efficacy of brigatinib versus alectinib in terms of PFS by IRC and OS was based on previously published ITCs of brigatinib (ALTA-1L trial) and alectinib (ALEX trial) [19, 20]. The ITCs used Burcher, Anchored Matching-Adjusted Indirect Comparisons (MAIC) with crizotinib as common comparator, and unanchored MAICs, all of which showed that there were no statistically significant differences between brigatinib and alectinib in terms of PFS and OS in patients with ALK-TKI-naive NSCLC. Thus, the efficacy of brigatinib and alectinib was assumed to be the same in the base case analysis through cost-minimization analysis, and safety was also assumed equal between both treatments. It should be noted that, although in all the methods used in the published ITCs, no statistically significant differences were found between brigatinib and alectinib, the point estimates of the PFS and OS hazard ratios (HRs) may have sometimes favored brigatinib and sometimes alectinib. Thus, cost-effectiveness analyses were conducted as scenarios using different point estimates from the results of the previously published ITCs [19, 20].
Ethical StatementThis article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Cost ParametersThis study adopted the perspective of China’s healthcare system. The costs considered in the model included the drug costs of brigatinib and alectinib, medical and healthcare resources before and after progression, adverse events management, concomitant medications, subsequent treatments, and palliative care. Costs were obtained from public sources, literature (costs converted using 2025 exchange rate [7.25 Yuan per 1 USD]), and clinical expert opinion. Consulted clinical experts are listed in Supplementary Table 1.
Drug CostsSupplementary Table 2 presents the drug costs, usage, and dosage of brigatinib and alectinib. The recommended dosages were derived from the label instructions, among which brigatinib was 90 mg orally once daily (OD) for the first 7 days and then increased to 180 mg OD orally [18]; alectinib was 600 mg (4 capsules of 150 mg), orally twice daily (BID) [17].
Cost of Medical and Healthcare Resources UtilizationThe healthcare resource utilization (HCRU) included medical oncology outpatient registration fees, laboratory tests, imaging, and electrocardiograms (ECGs). Considering that the patient’s disease state worsens after disease progression, the model assumed that the utilization of healthcare resources was different in the PF and PD states. Healthcare resource utilization and the corresponding unit costs were obtained from clinical expert opinion (Supplementary Tables 3–5).
Cost of Adverse Events ManagementConsistent with previously published cost-effectiveness analyses of ALK-TKIs [21, 22], this study estimated and analyzed the treatment costs of severe adverse events (AEs) in patients receiving ALK-TKI therapy. This study calculated AE management costs, including grade ≥ 3 AEs, according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0 and estimated the management costs with incidences. The AE management costs were obtained from clinical expert opinion (Supplementary Table 6).
Other CostsMedications such as acetaminophen, metoclopramide, dexamethasone, loperamide hydrochloride, and amoxicillin were included in the ALTA-1L study [15]. Through clinical expert opinion, this pharmacoeconomic analysis study limited concomitant therapy to hepatoprotective drugs, which increase white blood cells, thymosin, and antiallergic drugs; the estimated cost of concomitant medications based on the clinical expert opinion was 20.97 USD per 28-day cycle for both brigatinib and alectinib.
According to the recommendation of the guideline of CSCO 2024 [9], the subsequent treatments for patients after progression on first-line treatment of second-generation TKI was lorlatinib. In this model, we assumed that the treatment used after the patient progresses was lorlatinib for a total of 5.6 months according to a trial in China [23]. Supplementary Table 7 summarizes the subsequent costs.
In this model, the total cost of palliative care for patients with NSCLC was 1801.33 USD on the basis of the published data that evaluated the cost effectiveness of ceritinib and alectinib versus crizotinib in the Chinese healthcare setting [21].
Utility ParametersThe utility value used in the model was according to Shen et al. [24]. The utility value of progression-free state in the model was 0.856, and the utility value of disease progression state was 0.768. Disutility due to AEs and getting older were included in the utility estimation. In this model, the incidence of AEs (grade ≥ 3) was adjusted for the cycle length, and the QoL loss was 0.024 for each adverse event based on a previously published cost-effectiveness analysis of brigatinib conducted from the payer perspective in USA [16]. In addition, the model included a utility decrement associated with increasing age [16, 25].
Sensitivity AnalysisLike most pharmacoeconomic analyses, one-way sensitivity analysis was conducted in the CMA. The model uncertainty was assessed by varying all costs included in the model (Supplementary Table 8).
Comments (0)