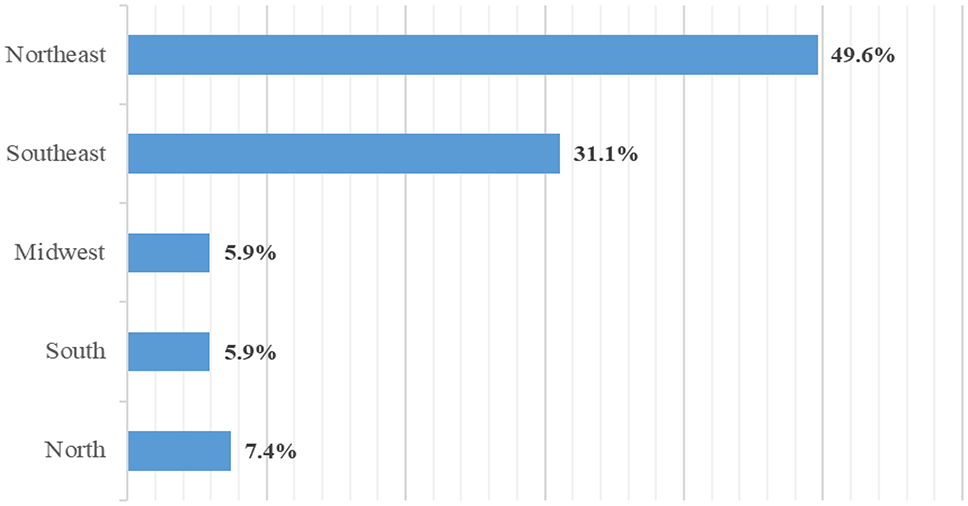
This is to our knowledge the first Brazilian study in the last decade to evaluate rheumatologists’ knowledge, beliefs and perceptions of biosimilars. Our results provide a comprehensive picture of the acceptance of biosimilars and the associated challenges. Most of the respondents were women aged 30–59 years, matching the demographics of the Brazilian Society of Rheumatology [14]. Predominantly located in the Northeast, many of the respondents worked in both the public and private sector, a fact that may have influenced their view on the prescription of biosimilars.
Almost all were familiar with the definition of biosimilars and adhered to guidelines. In comparison, in another study 83% of the respondents were familiar with the definition given by the Food and Drug Administration (FDA) [11]. Most were aware of the requirement of equivalence between biosimilars and their reference drugs with regard to effectiveness and safety, contrasting with another study in which only half the participants were aware of such criteria [12]. In another Brazilian survey performed in 2010, Brazilian rheumatologists’ knowledge of biosimilars proved to be limited. Although 67% claimed to be familiar with them, only 34% correctly defined the term [15]. Moreover, the rheumatologists in our sample reportedly keep abreast with the literature on the topic, suggesting a strong interest in and endorsement of the concept.
However, despite the high level of knowledge and familiarity observed, over half the respondents did not feel comfortable replacing the reference drug with a biosimilar. In contrast, 91% of the participants in another study were in favor of substitution [12]. Data from a rheumatologists’ opinions study showed that the main concern regarding commercialization was pharmacovigilance [15]. Thus, our results point to the need for Brazilian rheumatologists to engage in continuing education [16].
In addition, only half the participants believed biosimilars to be as safe and effective as their reference drugs for all indications, despite being aware of the concept of extrapolation of indications. In another study, only 12% felt comfortable prescribing biosimilars [12].
The idea of switching between biosimilars based on the same reference drug, without consulting an expert, was met with considerable resistance, indicating a limited understanding of the concept of interchangeability, according to which one biosimilar can be replaced with another biosimilar without compromising effectiveness or safety [13].
International regulatory agencies guarantee the safety of such substitutions [17, 18], and the Brazilian regulatory agency established the criteria for interchangeability in 2017 [19]. Although an authorization is not required, informing the original prescriber and involving the patient is a recommended practice [20, 21]. Multiple changes within a year should be avoided since the persistence of the treatment in this period is similar to that of the respective reference drug [22, 23].
Patients with no history of biologic drug use were the preferred profile for prescription, followed by stable patients, matching the findings of another study [11]. This approach is consistent with the recommendation of prescription of biosimilars to stable or naive patients [24].
Adherence to guidelines was the decisive factor for prescribing biosimilars in our sample. Only 28.1% laid more emphasis on cost reduction. In another studies, however, more than half of the rheumatologists specified cost reduction as the main reason for prescribing biosimilars [15, 25], highlighting the need to clarify these issues among prescribers.
Interestingly, while 84.3% of respondents acknowledged that biosimilars improve access to biologic therapy, only 28.1% cited cost reduction as a primary reason for prescribing them. This apparent contradiction underscores a disconnect between the perceived systemic benefits of biosimilars and their practical implications in clinical decision-making. Although lower cost is the principal advantage of biosimilars from a policy and budgetary perspective, individual prescribers may not directly observe or be impacted by these savings, particularly within SUS, where drug procurement is centralized and decisions are often made through institutional bidding processes.
Consequently, physicians may associate improved access more with policy-level strategies and broader availability than with the direct economic incentives that drive biosimilar adoption in other healthcare systems. This highlights the importance of aligning clinical education with the broader economic rationale behind biosimilar integration, to foster more coherent adoption strategies.
International experiences highlight that the successful adoption of biosimilars depends largely on national policy and system-level coordination. In Spain, biosimilars generated €2.3 billion in savings over a decade, mainly through competitive pricing and hospital procurement strategies [26]. Norway and the UK also demonstrated that structured approaches, such as national tendering, prescriber incentives, and switching protocols—can expand access to biologics while reducing costs [27]. In Poland, real-world data showed that biosimilar policies doubled treatment access without increasing healthcare spending, and enhanced disease control when combined with physician oversight and continuous education [8, 28]. These findings reinforce that effective biosimilar integration requires more than prescriber willingness, it demands supportive health system frameworks.
Our study was limited by the cross-sectional design which made it impossible to evaluate changes in acceptance over time. Also, the self-administered questionnaire may have influenced the participants’ perceptions, and although the demographic profile of respondents resembles national data, the use of spontaneous recruitment via social media, email, and WhatsApp may have introduced a selection bias, with a higher proportion of respondents from the Northeast, despite the greater concentration of rheumatologists in the Southeast. This geographic imbalance may limit the generalizability of the results. Finally, institutional, economic and regulatory issues were not analyzed in depth, limiting our understanding of the hurdles preventing the adoption of biosimilars in Brazilian clinical practice.







Comments (0)