This study sought to evaluate the use of existing guidance for the genetic evaluation of HL in Ohio through surveying parents of children with HL and providers involved in the diagnosis and care of HL. The first effort to evaluate this in the state of Ohio, these results demonstrated inconsistency with provider practice and perceived responsibilities, and variable parent experiences in receiving genetic HL evaluation. These findings underscore important deficits and opportunities for both provider and community education in this area.
Many parents did not provide the type and severity of their child’s HL. Prior literature has demonstrated variable recall of diagnostic hearing results, more commonly only reporting knowledge of final diagnosis but poor understanding of the details of the audiogram and hearing mechanism (Watermeyer et al. 2012). This may be due, in part, to emotional responses such as grief, worry, and sadness to a new HL diagnosis that may impact one’s memory of fine details (Gilliver et al. 2013). Variable knowledge may also be due to health literacy (Gilbey 2010; Minchom et al. 2013). The timing and modality used to relay diagnostic information and strategic timing may also have an impact. During the time of this study, it was not required of Ohio HL providers to provide the diagnostic hearing evaluation results in writing. OAC 3701-40-08 was implemented on December 1, 2019, and hearing screening providers are now required to provide the results of the hearing evaluation in writing to parents/caregivers upon completion of the diagnostic evaluation. Future studies are needed to assess impact of this new documentation procedure.
Several participants commented on the timing of their child’s evaluation and their perceived impact of this timing. Participants 7 and 23 emphasized the importance of early detection and treatment of HL in an open response survey question: “We are thankful for newborn screening because we were able to get him aided before he was three months old” (Participant 7) and “We are very thankful it was diagnosed early so we could get hearing aids and not lose any time to learn language” (Participant 23.) In contrast, Participant 38 statesd, “the way it was presented to me was that it was not something needed immediately so I deemed it not important right now.” These contrasting Participant reflections suggest a need for providers to evaluate patients individually and provide flexibility in their plan for medical management. A variety of personal and medical factors can influence parental decision making, especially regarding genetic testing, and thoughtful interactions with the medical team are needed to support shared decision making.
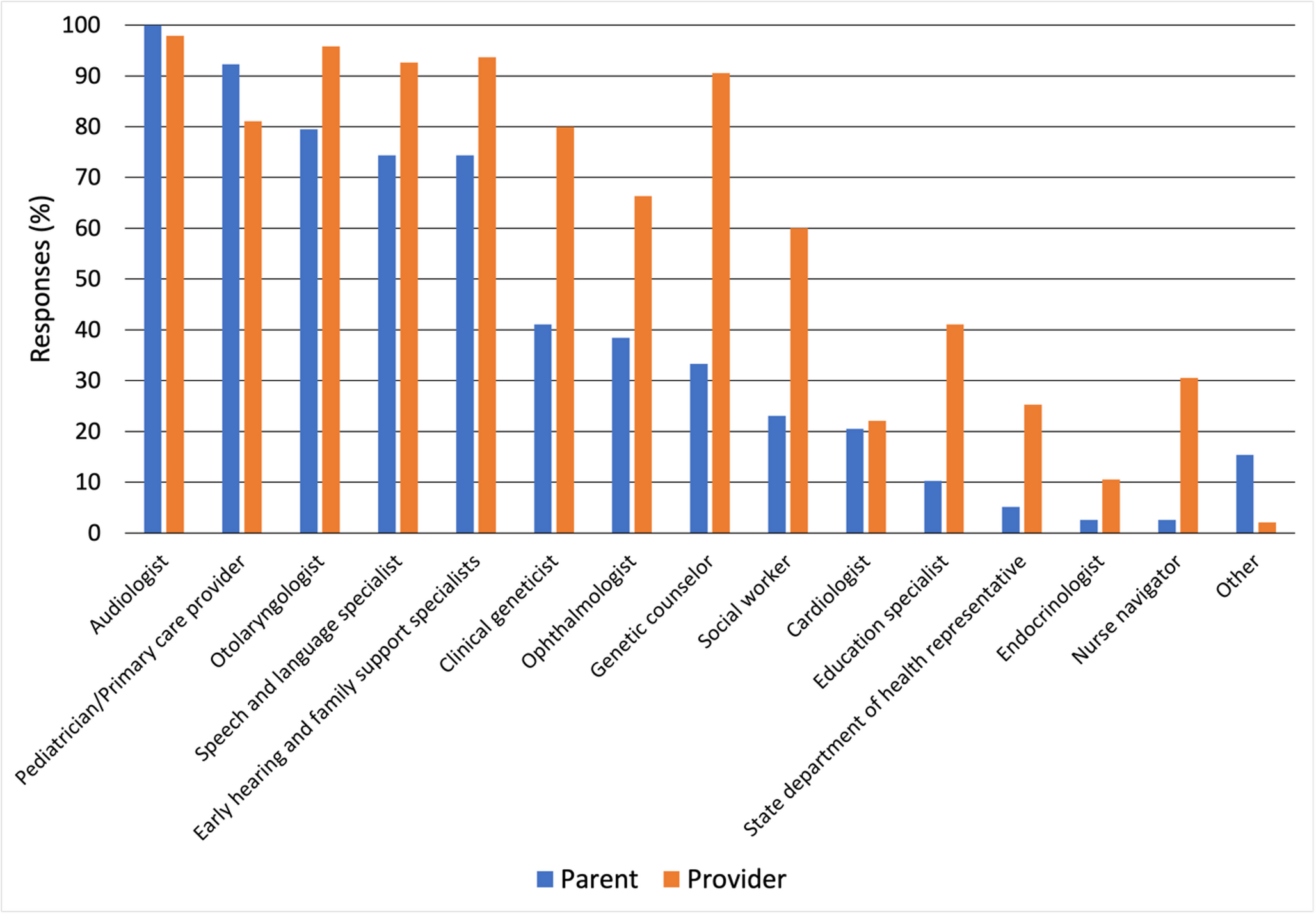
The JCIH, AAP, and ACMG recommend that a multidisciplinary care model of HL include a referral for a clinical genetics evaluation (Table 1) (ACMG 2024; JCIH 2019, 2007; Li et al. 2022; Alford et al. 2014a, b; Harlor and Bower 2009). Less than half of participating parents reported receiving complete multidisciplinary care within three months, with three-quarters of affected children seeing all members of the multidisciplinary team by age six months. Further, less than half of parents (41%) interacted with genetics, despite 91% of providers indicating that genetics should be part of the care team (Fig. 1). This may be due to a lack of referrals from care providers, or lack of parental awareness of the referral and availability of genetics services. Lesperance et al. found that the optimization of guideline implementation is dependent upon consideration of the parent/family, informed decision making, and flexibility in approach and timing of the genetics evaluation (Lesperance et al. 2017). This survey was distributed between August and December 2019 to families of children born in 2017–2018, all affected children were three years of age or younger at the time of participation. As a result, this study captured family experiences relatively early in the post-diagnosis trajectory. Genetic testing within a few months after birth may offer clinical and reproductive benefits, including informing etiology, guiding medical management, and clarifying recurrence risk. However, we also recognize this cross-sectional approach and sample time frame as a limitation, as it is also possible that families may have pursued testing as their children at later ages than would have been captured by this study, albeit outside the recommended genetic testing time window according to US professional organizations.
A collaborative approach involving the primary care provider, ENT, ophthalmologist, developmental pediatrics, early hearing support specialists, social work, and genetics is recommended by JCIH (JCIH 2019). The recently updated ACMG clinical evaluation and diagnosis of newborn HL guidelines highlight the role of the genetic counselor and recommend all newborn HL patients receive post-test genetic counseling, regardless of testing result (Li et al. 2022). However, a barrier to this care model is currently limited size of the clinical genetics’ workforce, as recognized by The American Board of Medical Genetics and Genomics (Jenkins et al. 2021; Maiese et al. 2019). Novel service delivery models will be needed to accommodate access to genetics services for diverse patient populations, including HL (Raspa et al. 2021).
Parental concerns about the cost of genetic testing was a commonly cited drawback. A recent study evaluating parental perceptions and experience of genetic testing for HL also extends this finding in a survey of 146 parents of children with HL, with less than half (48%) of participant’s children received genetic testing; cost was cited as a reason for not having testing in this study, in addition to being unaware of recommendation, not interested, time, fear of results, and testing not being offered (Cejas et al. 2024 ). Accordingly, families with a household income over $100,000 were more likely to pursue genetic testing ( p = 0.044, Fisher’s Exact Test). This suggests that lower income may be a barrier to receiving genetic testing, and indirectly to receiving genetics services. Participant 2 commented that, “ It would be nice if this was covered by insurance so we could test her genetics to see how this will impact her, if any other issues will arise, and what her future of a family would look like. However, the testing is not affordable so we will continue to focus on her treatments and whatever other issues arise. ” A confirmed genetic diagnosis may, in some cases, lead to additional medical evaluations or surveillance due to associated health risks. For example, in Jervell and Lange-Nielsen syndrome, which includes bilateral sensorineural HL and a predisposition to Long QT syndrome, a genetic diagnosis will prompt a cardiac evaluation. Genetic diagnosis also has potential to reduce the need for ongoing diagnostic testing by clarifying the etiology early in the care pathway, potentially limiting long-term costs of the diagnostic journey for patients and families. Further, with a future of precision therapies including gene-specific treatments on the horizon for HL, diagnosing genetic etiology will be the gateway to access novel treatment approaches as they enter into clinical care. With such care options emerging, it is not surprising that cost has been shown to also be a provider concern, with another investigation reporting that ENTs voiced insurance barriers as preventing them from ordering genetic testing (Heyward et al. 2023 ).
The AAP and IPOG guidance state that ENTs should consider ordering connexin gene testing for HL, while the updated ACMG guidelines recommend a broadere HL gene panel for all newborns with HL (Harlor and Bower 2009; Liming et al. 2016; Li et al. 2022). Half of ENTs in this study reported ordering connexin gene testing as one of their primary responsibilities, while only 36% reported routinely ordering connexin genetic testing in clinical practice. No ENTs in this study reported ordering comprehensive HL gene panels. While this study did not directly evaluate reasons for lack of ENT uptake of genetic testing, an open-ended response was provided by a parent Participant that “Genetic testing does not change the treatment. Hearing loss isn’t something we need to figure out or cure. Doctors push this testing for their own benefits/reasons. Even with testing hearing loss becoming more severe still isn’t predictable”. This perspective underscores the importance of shared decision making in the genetic evaluation of HL. Genetic counselors are trained to facilitate the genetic testing decision making process, including both educational and psychological support as a part of this consideration, which is why guidelines recommend this service as a part of the HL care team. However, a recent study of parents who pursued genetic testing for their child with HL found that 55% did not receive counseling before testing, and only 42% received genetic counseling afterward. The study team noted that their data was consistent with prior research, which showed that parents who received either pre-test or post-test counseling reported a more positive experience with the genetic testing process (Cejas et al. 2024). Cultural identity in the HL community influences perspectives on genetic testing, highlighting the importance of informed decision-making that respects patient and family values.
An opportunity for comprehensive genetic evaluation of HL is essential to ensure accurate and timely diagnosis and personalized care planning. Emerging gene therapies for genetic forms of HL highlight the potential for personalized care, with a definitive genetic diagnosis being required for eligibility. Many different therapies are in development including gene replacement therapies via adeno-associated viral (AAV) vectors, antisense oligonucleotides, small molecules, and CRISPR-based gene editing (Omichi et al. 2019; Leclère et al. 2024). Gene replacement therapy using AAV for OTOF-related auditory neuropathy spectrum disorder (DFNB9) has shown early safety and efficacy in clinical trials in China, with ongoing studies worldwide, including in the United States (Lv et al. 2024; Wang et al. 2024). These rapidly evolving precision medicine treatments for HL emphasize the critical need for early genetic diagnosis to ensure access to emerging therapies (Shearer 2024).
There are limitations to this study. Some items analyzed in the survey instrument were not validated, we were limited by asmall sample size, and the study was only conducted in Ohio; Therefore, the reported results are not generalizable. In addition, both participant groups were comprised of mostly metropolitan/suburban, white, middle-class females. These data are crossectional and were collected within the first three years of life of the affected children, therefore it is possible genetic testing may have been performed at a later age, albeit outside of the recommended time window for genetic diagnosis according to current guidance. There is also potential ascertainment bias, with parents and providers with interest in the genetics of HL more likely to participate, in which case these utilization patterns reported may be overestimates. Additionally, the study materials were created and study completed prior to the release of the JCIH 2019 update and the ACMG 2022 update. The 2022 ACMG update includes a recommendation change to order a multi-gene HL panel, rather than GJB2/GJB6 gene sequencing, for initial evaluation. While our study did not directly assess opinions regarding targeted gene testing versus multi-gene HL panels in providers, we can anticipate an updated survey may identify a broader movement to multi-gene HL panels.






Comments (0)