This study was approved as “exempt with limited review status” by Hunter College of the City University of New York (IRB protocol #2022–0542-Hunter) on September 9, 2022.
Paper consent forms were provided to in-person control-group participants and all experimental-group participants prior to data collection. For online control-group participants, an online consent form was provided via Qualtrics Survey software prior to data collection. There was no more than minimal risk for participation in this study.
Experimental-group participants received $30 compensation ($10 for the first data collection session and $20 for the follow-up) while control-group participants received $20 ($10 for each session). Participants were encouraged to use this compensation to purchase non-perishable food items that meet the household’s dietary needs for their disaster kit.
Potential participants were recruited from Korean Community Services of Metropolitan New York, Inc. (KCS), one of the largest community-based, social service organizations in the USA. KCS is dedicated to addressing the needs of the Korean American communities, helping them overcome economic, health, and social barriers to become independent and thriving members of the community [21]. KCS has seven locations across NYC’s Queens, Brooklyn, and Manhattan boroughs, offering a wide range of services that extend beyond community and immigration assistance.
Participants were recruited at the KCS community centers via both on- and off-line flyer distribution, including outreach efforts, such as health fairs, engagement with ethnic media (i.e., local Korean newspapers and radio stations), workshops at local libraries, partner organization facilities, and at Korean churches. Screening was conducted in-person, via telephone, or online, depending on how the potential participant contacted the study team.
One participant per household was eligible to participate. Inclusion criteria included being aged 18 years or older, fluent in Korean, and living independently within the New York metropolitan area. Participants with cognitive impairments were excluded due to their limited role in household disaster preparedness. Non-Korean-speaking individuals were excluded because this study was also a pilot test of the K-HEPI. Study team members screened participants for eligibility, delivered the recruitment script, obtained informed consent, and administered the demographic data form.
Recruitment and data collection for the study began in February 2024 and concluded in July 2024. Three KCS sites, which could accommodate large class sizes, were selected to host the experimental groups. To limit cross-contamination, recruitment for the control group was excluded from sites nearest to the intervention locations. Other potential data collection sites were contacted to determine their interest in participating. Participants were assigned to study groups based on the site through which they were recruited, and sites were blinded to which group their members were assigned to.
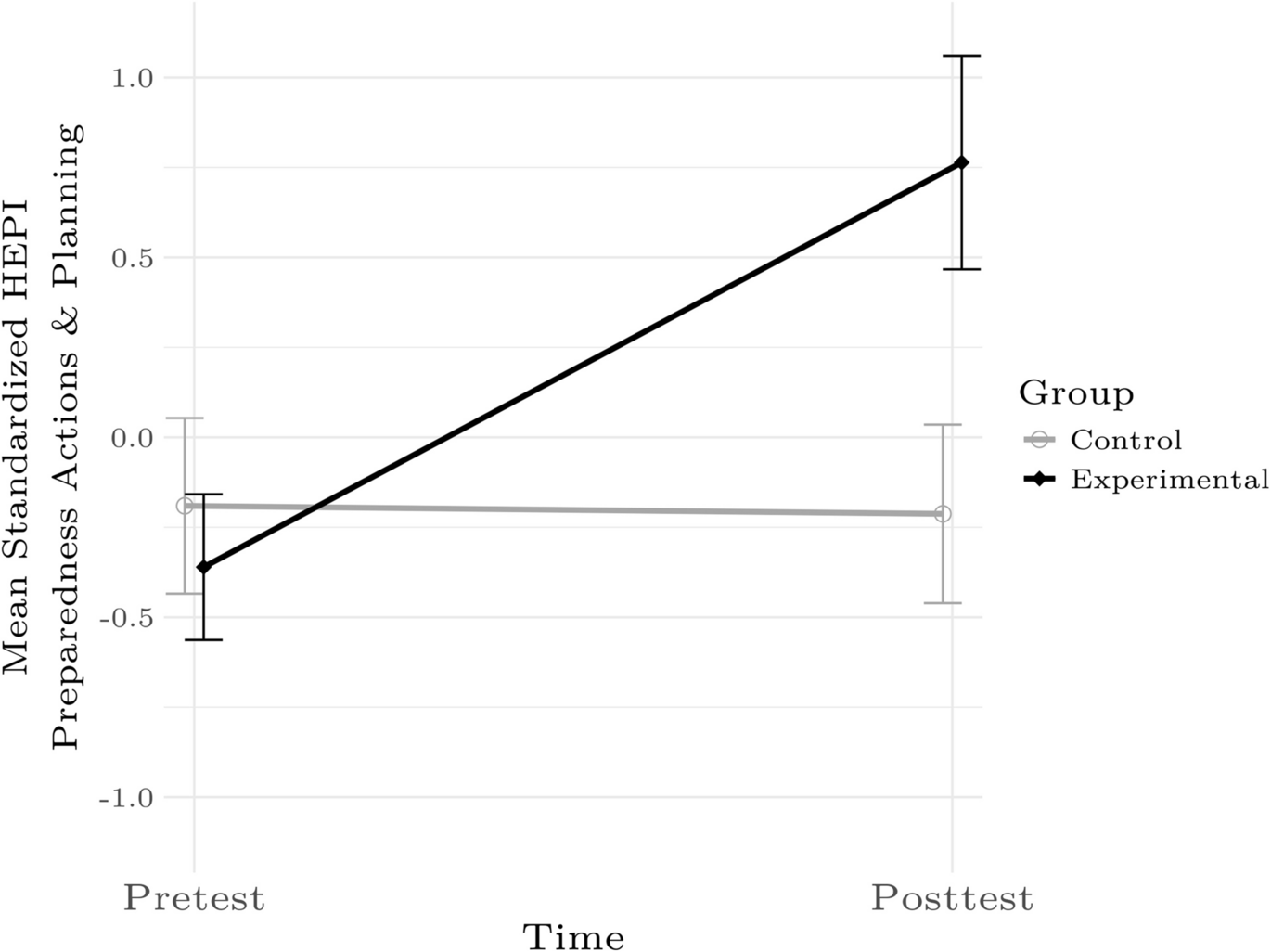
After the K-HEPI was translated and field tested [20], we utilized it in a controlled, single-blinded, non-randomized, before-after study to measure the level of household disaster preparedness of the target population before and after participating in the N-TORM educational intervention. We compared the K-HEPI scores of the experimental group and the control group at baseline and 1-month follow-up.
This was a phase I feasibility study for which we did not have prior knowledge of effect sizes, correlations of scores between time points, or estimations of any sphericities between time points. We therefore estimated that we would have a “small” effect (f = 0.1) [22] for differences between the two groups measured at two time points, that the inter-time correlation of K-HEPI scores would be moderately high (r = 0.5) and that there would not be significant sphericity. We assumed power (1 – β) is 0.8 and used α = 0.05 as the threshold for statistical significance. Given these parameters, we estimated needing a total of 350 participants for a repeated measures ANCOVA. To account for a potential attrition of 10%, we estimated needing 388 participants.
The primary outcome was the K-HEPI General Preparedness score, which was derived from a translation [20] of the 51-item English HEPI [23,24,25] that measures disaster preparedness actions, knowledge, and supplies of households. The K-HEPI questions are objective and assess what the respondent presently does or has for disaster preparedness in a dichotomous format. Respondents are asked to check which preparedness actions they have completed and what disaster supply kit items they have in their home; raw scores on the K-HEPI’s General Preparedness scale can range from 0 to 41. The General Preparedness scale is designed to be divisible into two subscales, Preparedness Actions and Planning and Disaster Supplies and Resources, that are themselves applicable to all households. The K-HEPI has three additional subscales (Special Actions Part 1, Special Actions Part 2, and Access and Functional Needs) that are only relevant to households with infants, children, pets, utility connections within the home, or with members who are dependent on prescription medications or eyeglasses, have a disability, are 65 years of age or older, or are pregnant.
Secondary outcomes included participants’ experience with the N-TORM intervention and the community health worker’s experience with implementation. Covariates included military status, history of chronic disease, disability status, predominant language proficiency, age, household composition or familial structure, ethnic/national origin identity, place, race, gender, education, employment, income, disaster risk perception, disaster preparedness self-efficacy, and prior disaster experience.
Control Group
While the control group did not receive a disaster preparedness intervention, they may have been exposed to mass media campaigns in NYC. After their second data collection, participants received the Korean version of the two-page pocket guide, Prepared New York: Disaster and Emergency Preparation [26]. In-person participants received paper copies, while online participants were provided with a PDF link.
Experimental Group
Nurses on the study team trained KCS community health workers to deliver the N-TORM intervention. One individual was selected as the instructor to ensure consistency in delivering the educational component. The instructor demonstrated competency by teaching back to the study team. She used a standardized presentation and handouts for all classes. To monitor intervention fidelity, study team members observed most N-TORM sessions and documented the instructor’s activities, including meeting frequency, content, and duration.
The experimental group received two, 1-h, in-person classes 2 to 4 weeks apart to help them develop their family evacuation and communication plans, identify community resources, and assemble a disaster supply kit. The instructor used a lecture and the Korean version of a booklet called Ready New York: My Emergency Plan [26] along with a disaster supply kit shopping list as handouts to educate the participants about the essentials of household disaster preparedness.
The first class began with instructing the participants to fill out the booklet during class and complete the remaining sections as homework. The class content complemented the booklet and the K-HEPI. The instructor reviewed different sections of the booklet and instructed the participants on how to write down their emergency plans. Participants wrote their medical history, medications, physicians, next of kin, pharmacy contact information, evacuation plan information, and emergency communication plan. The booklet included household disaster preparedness recommendations, evacuation zone information, a disaster supply kit contents list, local utility contact information, insurance coverage recommendations, shelter locations, and special needs and priority utility restoration registry information. Participants were instructed to keep their completed booklets as a reference for their household disaster preparedness plans and community disaster resources information.
During the second class, the instructor reviewed the participants’ booklets for completion (approximately 2 min per participant), addressed their questions on their evacuation and communication plans and disaster kits, and facilitated a 30-min group discussion to share disaster preparedness experiences and foster social support. The discussion was guided by participants’ progress with their booklet completion. For example, if a participant had not listed two emergency contacts, the instructor asked, “Is anyone willing to serve as the second emergency contact for a classmate? If so, please exchange contact information.” Similarly, if a participant had not recorded an emergency meeting place, she prompted, “What locations have others chosen as a meeting place in case of an emergency evacuation?” Finally, the instructor led a discussion on tips and techniques for creating the disaster supply kit by asking, “Has anyone created or started their disaster supply kit? What is your plan to complete it?”.
Data Analysis
Descriptive statistics were reviewed prior to regression analyses examining the associations between the study variables. We tested differences in K-HEPI scores between the groups (control vs. experimental) and times (pre- vs. posttest) with hierarchical linear regressions with time nested within participants. Adding additional terms, like demographics, did not lead to stable final models and so were not included in these tests.
The reliability of the K-HEPI was measured by looking at the internal consistency of the items (ordinal α coefficients and item-total correlations). Confirmatory factor analysis was used to examine the factor structure of the K-HEPI and to compare it with that of the English version. Details on the psychometric data analysis are provided in Samuels et al. [20].

Comments (0)