
Remember me
This single‐center retrospective comparative study was conducted following the Helsinki Declaration and was registered as a Chinese clinical trial (ChiCTR2400084358). The study’s approval was obtained from the Ethical Committee of Peking Union Medical College Hospital (PUMCH; approval no. I-24PJ0959).
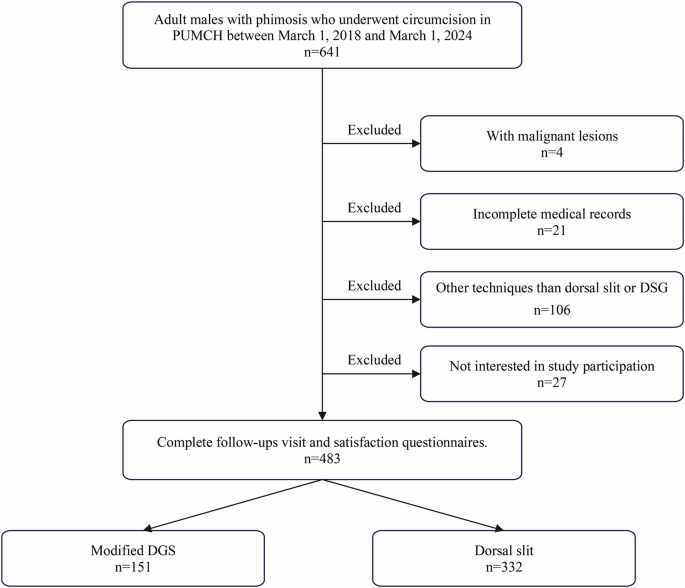
SubjectsAdult males with phimosis who underwent circumcision at PUMCH between March 1, 2018 and March 1, 2024 were recruited for this study by study staff via telephone. After receiving detailed explanations regarding the benefits, risks, and procedural differences of each method, patients were allowed to choose the surgical technique according to their personal preferences. The reasons for ineligibility are detailed in Fig. 1. Upon signing informed consent forms at the scheduled clinic, patients can be followed up immediately.
Fig. 1
Flowchart of cohort selection.
The inclusion criteria were as follows: (1) patients aged 18 and above; (2) patients diagnosed with phimosis; (3) patients who underwent circumcision at PUMCH.
The exclusion criteria included the following: (1) presence of malignant pathology in the resected foreskin lesion; (2) patients unable to understand the study conditions and objectives; (3) patients with incomplete clinical data; (4) patients circumcised using techniques other than the dorsal slit or modified DGS technique.
Data collectionAt the clinic, participants were physically examined by staff and completed a brief questionnaire about satisfaction with penile appearance. Additionally, medical data were collected through the hospital information system, including the patient’s age, diagnosis, medical history, circumcision techniques, surgical duration, postoperative pathological results, and complications recorded during outpatient follow-up.
Surgical proceduresThe patients underwent the same preoperative preparation: oral antibiotics administered on the surgery day, supine position, routine skin preparation, routine field disinfection with povidone-iodine, and spreading of a towel with 10 mL of 1% lidocaine block anesthesia of the penile dorsal nerve.
After circumcision, the patients’ cutting edge was wrapped with vaseline-coated gauze, and the outer layer was properly bandaged with elastic bandages. Dressing removal was scheduled 24–48 h after circumcision following confirmation of no bleeding. Intercourse should be avoided for four weeks after circumcision to prevent wound breakdown.
Dorsal slit techniqueIn the dorsal slit technique, the preputial orifice is first lifted with hemostatic forceps at the 3 and 9 o’clock positions to align the penis perpendicularly. A dorsal midline incision is then made in the prepuce using scissors until full retraction is achieved. Next, the adhesions between the glans penis and prepuce are carefully separated. The prepuce is freed up to 0.5–0.8 cm from the corona, and a circumferential incision is made around the glans, extending to the frenulum while preserving approximately 1 cm of frenulum tissue. Electrocoagulation is used to achieve hemostasis, and the two circular skin incisions are aligned. Finally, the full thickness of the foreskin, including both the skin and dartos fascia, is sutured together using 4–0 Coated Vicryl® Plus suture (Ethicon, Somerville, NJ, USA).
Modified DGS technique Modified dorsal slit techniqueMosquito forceps are applied at the 12 o’clock position of the prepuce, aligning them with the shaft of the penis. A dorsal incision is made between the forceps, which breaks the fibrotic ring and exposes the glans penis. The adhesions between the prepuce and the glans are then carefully separated until the prepuce is fully freed (Fig. 2A).
Fig. 2: Steps of the modified DGS procedure.
A Modified dorsal slit technique. B Marking the incision of the inner plate of the prepuce. C Marking the incision of the outer plate of the prepuce. D Modified guillotine technique. E Modified sleeve technique. F Separation of the inner plate and serosa. G Trimming of the inner plate. H Restoration of Dartos fascia continuity. I Skin suturing.
Marking incision linesFor the inner plate, incision lines are marked 0.3 cm from the corona at the 5–7 o’clock positions. A V-shaped incision line is drawn at the frenulum, approximately 1.5 cm from the corona (Fig. 2B). For the outer plate, the penis is stretched, and measurements are taken from the penopubic junction to the corona. The foreskin is then pulled over the glans, and the incision line is marked parallel to the coronal sulcus from the dorsal mark to the frenulum (Fig. 2C).
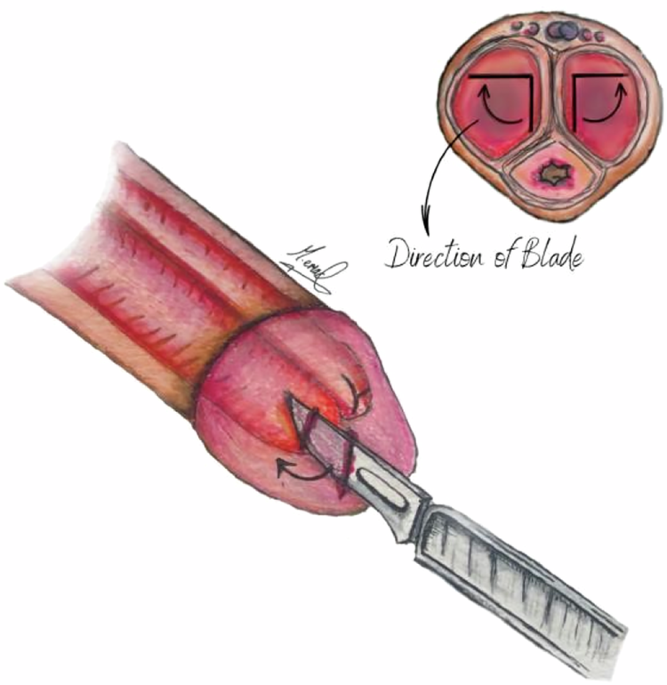
Modified guillotine techniqueThe frenulum is secured with an Allis clamp, and the prepuce is lifted vertically. The outer plate is clamped along the marked incision line, and the excess foreskin is excised (Fig. 2D). Any bleeding spots are treated as the clamps are removed.
Modified sleeve technique and inner skin trimmingMosquito forceps are used to lift the residual inner plate edge at specified points (Fig. 2E), and the dartos fascia is separated from the inner plate (Fig. 2F). The dorsal and lateral edges of the inner plate are trimmed along the marked line, leaving approximately 0.3 cm of skin proximal to the corona (Fig. 2G). The ventral dartos fascia and frenulum are left intact and are not separated.
RestorationThe dartos fascia is sutured at key points between the distal and proximal ends using 4–0 Coated Vicryl ® Plus suture (Ethicon, Somerville, NJ, USA) (Fig. 2H). The proximal penile skin is then sutured to the coronal preputial sleeve with the same suture (Fig. 2I).
For detailed surgical steps, please refer to the supplementary materials.
OutcomesThe primary outcomes of this analysis were (1) the rates and types of complications following circumcision, (2) participants’ satisfaction with penile appearance, and (3) surgical duration. Postoperative complications related to circumcision were defined based on World Health Organization guidelines and findings from previous studies [8, 13]. Complications were followed up on the 7th postoperative day, as most adverse events occur during or shortly after the circumcision procedure. Satisfaction with penile appearance includes overall satisfaction with penis appearance and the frequency of three common complaints: skin color mismatch, hypertrophic scarring, and edema [14]. Participant satisfaction was assessed using a self-designed, non-validated questionnaire. Surgical duration was calculated from the onset of anesthesia to the completion of the circumcision procedure.
Statistical analysisStatistical analysis was conducted following published guidelines [15]. Continuous variables are presented as mean ± standard deviation and analyzed using Student’s t-test or the Mann–Whitney U test, as appropriate. Categorical variables are presented as numbers and percentages and compared using Pearson’s chi-squared test or Fisher’s exact test, as appropriate. Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) software (version 22.0; SPSS Inc., Chicago, IL, USA). A p < 0.05 was considered statistically significant.
Comments (0)