This study sought to identify risk factors in LACC patients undergoing radiotherapy with and without CCRT, and to explore the prognostic influence of MRI-based TVR across diverse patient risk profiles. Our findings underscore the significance of FIGO stage, CYFRA21-1 levels, and TVR as key independent predictors of LACC treatment outcomes. This investigation uniquely evaluates the predictive value of TVR across different LACC risk categories, highlighting its prognostic relevance particularly in patients with CYFRA21-1 levels below 7.7 ng/ml undergoing CCRT. In the lymph node metastasis subgroup, patients with NVR ≥ 94% demonstrated still had a better prognoses prognosis.
Using MRI, we assessed TV and NV before treatment and mid-RT to calculate TVR and NVR. While previous studies have established the prognostic value of TVR in cervical cancer, the significance of NVR in cervical cancer prognosis has been less explored. Additionally, reported TVR cutoff values vary widely across studies [8,9,10].
This study found that in the node-positive subgroup, patients with NVR ≥ 94% demonstrated better survival outcomes, indicating that NVR, like TVR, is a valuable prognostic marker for cervical cancer. Sun et al. [20] applied the Youden index to identify an optimal TVR cutoff of ≥ 82.19%, correlating with improved outcomes in LACC patients undergoing CCRT. Using a similar approach, our study identified a distinct TVR cutoff, likely influenced by differences in patient demographics and treatment protocols. Variations in results may also reflect regional and ethnic differences.
LACC exhibits significant heterogeneity, even among patients with similar TVR levels, indicating diverse characteristics of residual disease. FIGO stage, a well-established prognostic factor, remains pivotal in guiding treatment stratification [12, 13]. Wagner et al. [21] retrospectively analyzed 18,649 CC cases from the SEER database, confirming TV as a consistent prognostic indicator across all FIGO stages. This underscores the importance of assessing TVR’s prognostic value within each FIGO stage category. Additionally, serum albumin levels, which reflect nutritional status, are recognized as significant prognostic factors in advanced cancers [22,23,24]. Our findings reaffirm the independent prognostic significance of FIGO stage and pre-treatment albumin levels in LACC, further validating the role of TVR in prognostication across different FIGO stages and in the context of albumin levels.
While CCRT demonstrated prognostic significance in univariate analyses, its effect was less pronounced in multifactorial analyses that included TVR, likely due to the higher proportion of patients achieving TVR ≥ 94% in the CCRT group. Mayr et al. [10] analyzed 114 CC patients and identified residual TV after EBRT exceeding 20% as a negative prognostic factor. However, only a small fraction of Mayr et al.‘s cohort received concurrent platinum-based chemotherapy, which may account for differences in key TVR thresholds between studies.
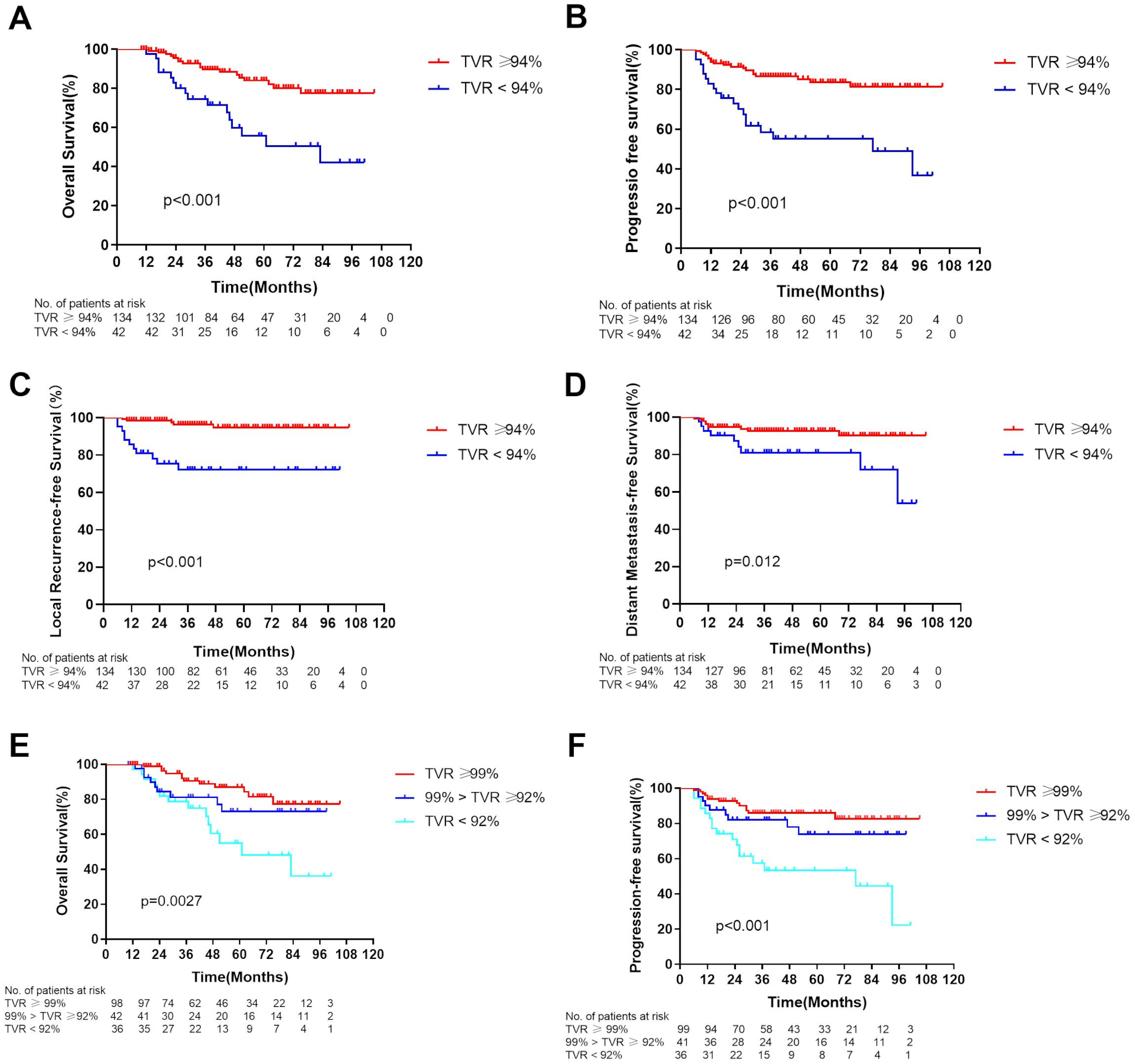
Our subgroup analysis, stratified by synchronous chemotherapy administration, reaffirmed TVR as a significant prognostic marker for OS and PFS in patients receiving CCRT, consistent with prior studies [9, 10, 20]. Conversely, the association between TVR and prognosis was not observed in patients treated with RT alone. These findings indicate that the prognostic value of TVR may be influenced by the treatment modality.
These findings suggest that treatment modalities may influence the prognostic value of TVR. Additionally, CYFRA 21 − 1 is an independent prognostic factor that may modify TVR’s prognostic significance [25]. Further validation is necessary to clarify TVR’s role in LACC patients with varying CYFRA 21 − 1 levels [17]. Our subgroup analysis showed no significant survival differences between TVR levels in patients with elevated CYFRA 21 − 1, likely due to a significant interaction between CYFRA 21 − 1 and TVR [17, 25]. These results highlight the importance of incorporating CYFRA 21 − 1 levels into future assessments of TVR’s prognostic impact. Notably, even in patients with elevated CYFRA 21 − 1, a high TVR does not ensure a favorable prognosis. This underscores the need for more intensive treatment strategies and vigilant follow-up in this subgroup.
The study has several limitations. Its stem from its retrospective design and execution at a single center setting, which may restrict limit the generalizability generality of our findings. Additionally, there is heterogeneity in the treatment regimens, necessitating validation through regimen, which needs to be further verified by external data. The intracavitary brachytherapy in this study was performed using conducted on a Point A-based approach rather than RT guided by 3D imaging, which could impact the results. Finally, the analysis study was conducted exclusively on T2-weighted imaging sequences. In future studies, other MRI sequences, such as diffusion-weighted imaging (DWI), should be incorporated to further validate these findings.









Comments (0)