Research design and patient selection
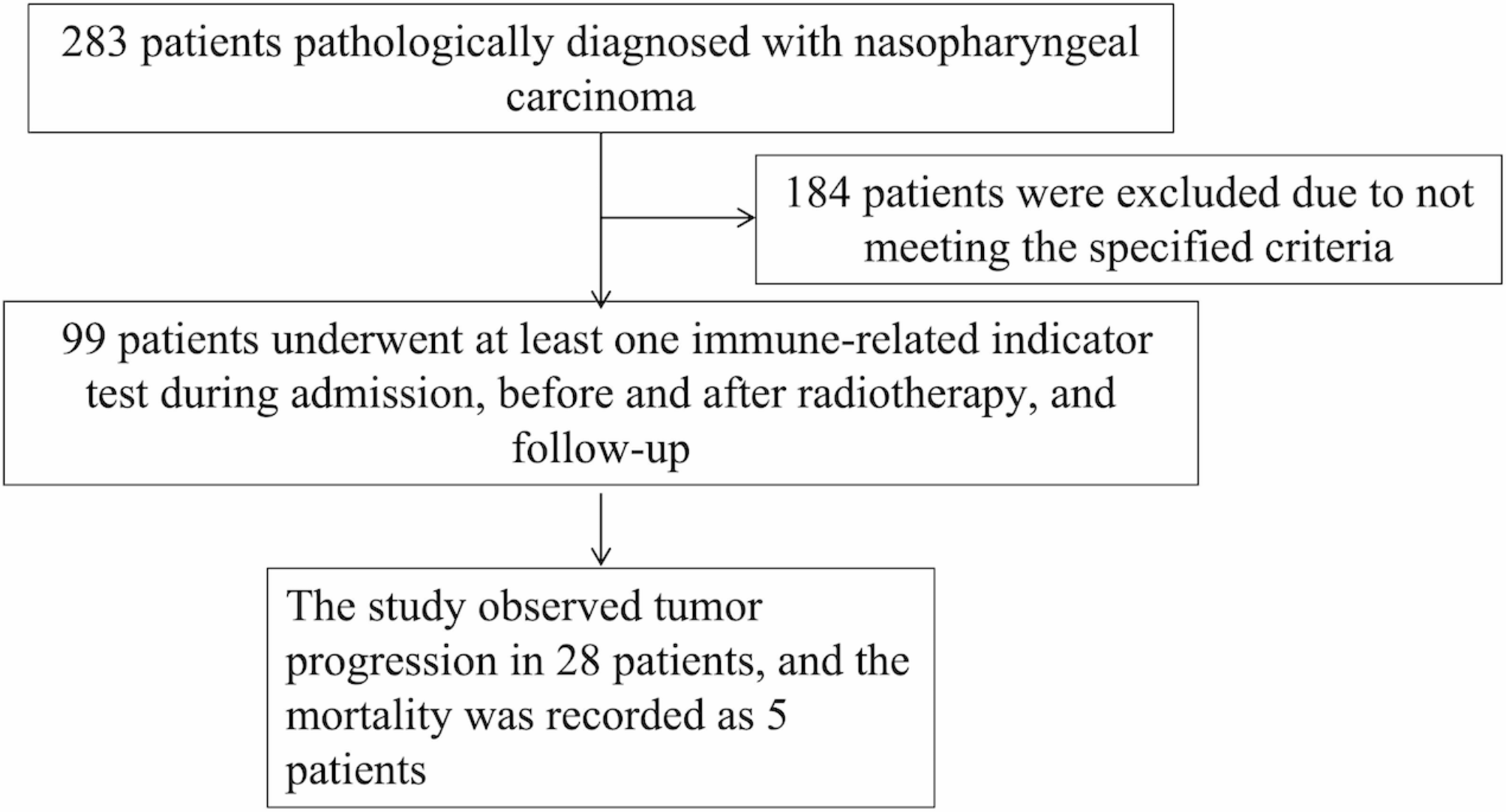
This study employed a prospective cohort study design. It included patients with NPC who were initially diagnosed and treated at our Hospital between August 2019 and July 2021. The inclusion criteria encompassed patients with comprehensive clinical, imaging, and laboratory examination data, those without prior treatment for NPC or other tumor types, and individuals who provided informed consent to undergo routine radiotherapy and chemotherapy treatments. Exclusion criteria comprised patients with severe infections or mental illnesses, those unable to complete radiotherapy and chemotherapy, individuals with immune system diseases undergoing immunotherapy, as well as patients lost to follow-up due to relocation or unrelated causes of death. Approval from the hospital ethics committee was obtained for this study.
Diagnosis and treatment of NPC
All patients were diagnosed with NPC based on pathological examination, using squamous differentiation as the diagnostic criteria. According to the 1991 World Health Organization (WHO) classification, NPC was classified into two types: type I, keratinizing squamous cell carcinoma or squamous cell carcinoma (KSCC), and type II, non-keratinizing carcinoma, which includes differentiated non-keratinizing carcinoma (NKDC) and undifferentiated carcinoma (NKUC) [13]. The TNM [14] staging was performed in accordance with the 8th edition of the Union for International Cancer Control/American Joint Committee on Cancer (UICC/AJCC) staging system.
The patients in this study received curative radiotherapy according to the “Chinese Nasopharyngeal Carcinoma Radiation Guidelines” [15]. The induction chemotherapy regimen consisted of a platinum-based two or three-drug combination, including cisplatin plus gemcitabine, cisplatin plus docetaxel, or docetaxel plus cisplatin plus fluorouracil. The dosages were as follows: intravenous administration of 75 mg/m2 of docetaxel on day 1, 75 mg/m2 of cisplatin on days 1–3, and 500 mg/m2 of fluorouracil on days 1–5. Each cycle lasted for three weeks with a total duration of 2–3 cycles. Synchronous chemotherapy drugs included either docetaxel plus cisplatin or monotherapy with intravenous administration of 75 mg/m2 of cisplatin on days 1–3, with or without intravenous administration of 75 mg/m2 of docetaxel on day 1 every three weeks per cycle. Alternatively, weekly intravenous administration could be done using a dosage of 30 mg/m2 for cisplatin. Efficacy assessment after systemic therapy was conducted according to the WHO Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST v1.1).
Data collection and follow-up
The clinical data, including gender, age, presence of chronic diseases, smoking and drinking history, diagnosis time, and treatment data, were collected from medical records. Prior to treatment initiation, all patients underwent routine testing for EBV serology using DNA analysis and CD lymphocyte subsets on the first day of admission. Plasma EBV DNA, which the cutoff value for EB DNA is set at < 5.0 × 102 copies, the units are copies per ml, was detected using a real-time fluorescence quantitative PCR method, Circulating immune cell subsets and NK cells in peripheral blood were analyzed using flow cytometry prior to treatment.
The treatment cycle lasted for a duration of 2 years, during which follow-up visits were scheduled at intervals of the first day of every 3 months for the first 2 years post-treatment, the first day of every 6 months from year 2 to year 5, and annually thereafter. Each follow-up cycle encompassed comprehensive assessments including blood routine and biochemical tests, nasopharyngoscopy, nasopharyngeal MRI, low-dose chest CT scan, abdominal ultrasound examination, and bone scan.
Outcome measures
The primary endpoint of this study is the progression of NPC, which encompasses tumor recurrence, infiltration, metastasis, or invasion of distant tissues and organs.
Statistical analysis
The chi-square test or Fisher’s exact probability method was employed to compare categorical variables between groups, while Student’s t-test or rank sum test was used for comparing quantitative variables. Survival curves were generated using the Kaplan-Meier method and compared using the log-rank test. A Cox model with progression as the endpoint event was utilized for multivariate analysis of survival time. Statistical analysis was performed using SAS 9.4 software with a two-tailed test, considering a p-value < 0.05 as indicative of statistical significance.





Comments (0)