
Remember me

The participants were recruited from the “Gait and Alzheimer Interactions Tracking” (GAIT) cohort, which conducted a cross-sectional study between November 2009 and November 2015 to compare the gait characteristics of individuals with varying cognitive profiles, ranging from healthy individuals to those with dementia. The study procedure has been described in detail previously (Beauchet et al. 2019). Participants had to be 60 years of age or older, ambulatory, community-dwelling, with adequate understanding of French language, and without acute medical illnesses in the past month. Additionally, they were required to have a MMSE score of at least > 10, visual acuity of at least ≥ 2/10, no severe depressive symptoms (15-item Geriatric Depression Scale score ≤ 10), and no acute medical illnesses in the past month. Individuals were excluded from participation if they had preexisting locomotor disorders, a history of stroke or sensorimotor sequelae from the central nervous system, any acute medical or surgical condition less than 3 months old, a score of greater than 10 on the 15-item Geriatric Depression Scale, or if they were unable to walk unaided for less than 15 min. For this analysis, we only included participants who underwent a brain MRI and a dual-task gait assessment. Participants were included after providing written informed consent to participate in the study. The research protocol was approved by the Angers Ethics Committee (CPP Ouest II-2009–12) and registered as ClinicalTrials.gov n° NCT01315717.
Clinical assessmentCognitive assessmentThe Memory clinic of Angers University Hospital (France) assessed all participants. Cognitive status diagnoses were made during multidisciplinary assessments involving geriatricians, neurologists, and neuropsychologists. Controls were subjects with normal neuropsychological results (MMSE score > 25 and negative Winblad criteria) (Winblad et al. 2004). Dementia was diagnosed using the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition, Text Revision) (Quinn 1999) and NINCDS/ADRDA criteria (Dubois et al. 2007). MCI was diagnosed according to the criteria detailed by Winblad et al (2004). These criteria require that the person is neither normal nor with dementia, there is evidence of cognitive deterioration shown by either objectively measured decline over time and/or subjective report of decline by self and/or informant in conjunction with objective cognitive deficits, and activities of daily living are preserved, and complex instrumental functions are either intact or minimally impaired.
Participants underwent evaluation using a neuropsychological battery that included standardized assessments of various cognitive domains. Global cognition was assessed using the Mini-Mental State Examination (MMSE), (Folstein et al. 1975) Alzheimer's Disease Assessment Scale-Cognitive Subscale (ADAS-Cog), (Kueper et al. 2018) and Frontal Assessment Battery (FAB) (Dubois et al. 2000). To assess instrumental functions, language abilities were evaluated with the ADAS-Cog and specific subtests from the Wechsler Adult Intelligence Scale-Revised (WAIS-R). Praxes were examined through the assessment of five different upper limb postures, along with related items from the ADAS-Cog. Visuo-spatial abilities were assessed using the Visual Object and Space Perception (VOSP) test battery as described by Warrington and James (1991). Memory performance was evaluated through a French version of the Free and Cued Selective Reminding Test (Dion et al. (2015), in addition to the Digit Span task (both forward and backward) derived from the WAIS-R. To assess executive functions, the Trail Making Test (TMT) parts A and B was administered.
Gait evaluationGait assessment was conducted using a Gaitrite© System, which is 972 cm long, to evaluate spatiotemporal gait parameters in older adults according to the European guidelines (European GAITRite® Network Group, Kressig, et Beauchet 2006). Participants completed three gait trials in random order to minimize the effects of learning and fatigue. They were instructed to walk at their usual gait speed (cm/s) while wearing their own footwear. During the dual-task trials, participants were instructed to walk at their usual pace without prioritizing either the gait or cognitive task. They were asked to perform the following cognitive tasks aloud: (i) counting backwards (CB) from fifty to zero one by one and (ii) naming animals (NA). The dual-task gait cost (DTC) was calculated for each trial using the appropriate gait speed with the formula: DTC = [(single-task gait speed—dual-task gait speed)/single-task gait speed] × 100 (Plummer et al. 2015). DTC was expressed as a percentage of slowing from the usual gait speed due to the added cognitive task. High DTC was defined as a slowing down of 20% or more, while low DTC is defined as less than 20%, as determined by our previous work (Sakurai et al. 2019; Montero-Odasso et al. 2017). The decision to utilize dichotomous DTC instead of continuous DTC was predicated on the observation that the 20% cutoff point has been demonstrated to be more clinically relevant and sensitive, given its capacity to account for intersubject variability (Montero-Odasso et al. 2017). The reliability of this protocol has been previously demonstrated (Montero-Odasso et al. 2009a, b).
MRI acquisitionBrain imaging was performed using either a 1.5-Tesla MRI scanner (until 2011, Magnetom Avanto; Siemens, Erlangen, Germany) or a 3-Tesla (from 2011, Magnetom Skyra, Siemens, Erlangen, Germany) using a standard MRI protocol including 3D T1-weighted magnetization prepared rapid acquisition gradient echo (MP-RAGE) images (for 1.5-Tesla MRI: acquisition matrix = 256 × 256 × 144, field of view (FOV) = 240 × 240 × 187 mm, echo time (TE)/repetition time (TR)/inversion time (TI) = 40.07 ms/2170 ms/1100 ms); for 3-Tesla MRI acquisition matrix = 256 × 256x128, FOV = 240 × 240x176 mm TE/TR/TI = 2.98 ms/2300 ms/900 ms).
MRI processingThe analysis utilized the CAT12 toolbox (Computational Anatomy Toolbox 12, vCAT12.8.2), an extension of SPM12 (Statistical Parametric Mapping, v7771), to conduct the voxel-based morphometry (VBM) on anatomical T1-weighted images. These images underwent automated segmentation into gray matter, white matter, and cerebrospinal fluid. Additionally, the volume of white matter hyperintensities (WMHs) was delineated as a separate class using the “expert mode” (Gaser et al. 2022). The pre-processing steps, adhering to the standard VBM protocol, involved comprehensive brain tissue segmentation and spatial alignment using the Shooting template (Ashburner et al. 2000, 2011; Gaser et al. 2022). The resulting gray matter volume (GMV) images, aligned to the template, were of a resolution of 1.5 × 1.5x1.5. Quality assurance was robust, involving both automated and visual inspections to ensure the absence of artifacts. To minimize individual gyral variations, the data were smoothed using a 6 mm full width at half maximum (FWHM) Gaussian Kernel. An absolute gray matter threshold of 0.1 was applied to ensure the inclusion of solely gray matter regions in the statistical analyses.
To extract GMV data from each significant cluster, binary masks were applied to the non-smoothed, modulated GMV images of each participant.
StatisticsTo describe the study population based on cognitive status groups (control, individuals with MCI, and those with dementia), we utilized appropriate statistical tests such ANOVA with post-hoc test and Tukey correction, or Chi-square test as appropriate. To adjust for skewness, we log-transformed WMHs volumes. We conducted statistical comparisons using JASP (Version.17.1, https://jasp-stats.org/).
To compare GMV (outcome) between the high and low DTC groups (predictor), we used the general linear model approach implemented in SPM12. Statistical analysis was conducted using a whole-brain ANOVA that included covariates such as age, sex, educational level (post-secondary or none), MRI field strength (1.5 T or 3 T), WMHs, and total intracranial volume (TIV). The VBM results were adjusted for multiple comparisons using the family-wise error (FWE) method, with significance set at p < 0.05. This correction was implemented alongside threshold-free cluster enhancement (TFCE) with 5000 permutations (Spisák et al. 2019). Significant clusters were identified on VBM statistical maps. These clusters were defined as having notable differences in gray matter (negative or positive) and comprising at least 10 contiguous voxels. The locations of these clusters were determined using the Automated Anatomical Labeling version 3 (AAL3) atlas (Rolls et al. 2020).
To investigate the effect of cognitive status on the relationship between GMV (outcome) and high versus low DTC (predictor), a moderation analysis was conducted using the PROCESS macro on R Core Team (Version 4.2.3, 2023, https://www.R-project.org/) and following Hayes’ guidelines. The PROCESS macro provides results that include logistic regression and the interaction with the regression coefficient if the interaction is significant.
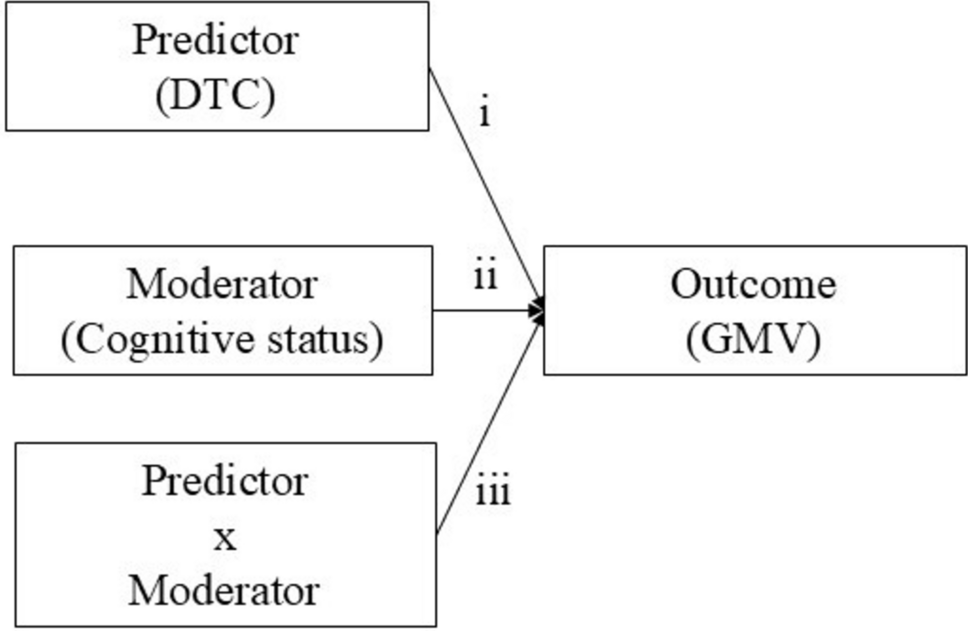
To probe for the moderation effect of the cognitive status (H1), it was necessary for the relationships for (i), (ii), and (iii) to be significant (Fig. 1). These relationships include (i) the direct effect of the predictor (DTC) on GMV, (ii) the direct effect of the moderator (cognitive status) on GMV, and (iii) the direct interaction effect (DTC x cognitive status) on GMV. In R PROCESS, the software automatically calculates the interaction effect and produces the likelihood ratio test explained by the moderating effect of cognitive status (increase due to interaction). The potential moderators, each assessed within an independent moderation model, were as follows: dementia versus control groups, MCI versus control groups, dementia versus MCI groups. A p < 0.05 was considered statistically significant. The moderation model was adjusted for covariates including age, sex, educational level, TIV, and MMSE.
Fig. 1
Output model of Cognitive Status Moderation effect on the relationship between Gray Matter Volume (GMV) and Dual-Task Cost (DTC)
Comments (0)