
Remember me
An open research design was chosen, because it best captures the emotional and cognitive elements in the patients’ treatment decision and to focus on the most essential aspects. The study follows a suitable explorative mixed methods design.
Patient sampleFemale patients with HR + /HER2- non-metastatic EBC with high risk of relapse, defined by (neo)adjuvant chemotherapy pre-treatment, who were on adjuvant ET or were planning to receive it were included. This stepwise multimodal study was conducted in Germany between October 2021 and March 2022 consisted of three phases: (1) desk research, (2) qualitative interviews, and (3) a quantitative online survey. The qualitative interviews included 20 patients, while the quantitative online survey included 85 patients. As the inclusion criteria targeted a very specific cohort of women, respondents for the ACBC analysis were recruited and screened via different channels such as physicians, support groups, social media (Facebook and Instagram), and free recruitment.
All patients were informed about the voluntary, confidential, and anonymous nature of this study. Additionally, patients were given relevant information in accordance with the European Society for Opinion and Market Research (ESOMAR)/European Pharmaceutical Market Research Association (EPhMRA) code of conduct such as data privacy. All respondents provided written consent.
Study designDesk researchDesk research consisted of the review of online resources from platforms such as Google and PubMed, as well as offline resources such as patient material from patient organisations and review of existing studies. Hereby, all side effects reported in context of patient reported outcome studies and other studies were considered. The aim of this phase was to deliver a series of attributes that are potentially relevant to treatment decision (decision criteria, treatment characteristics, side effects) and to develop an initial model of the treatment decision.
The outcome of this phase consisted of a model that included treatment attributes under four categories: “treatment goals”, “quality of life”, “side effects”, and “treatment modalities” (Fig. 1). Additionally, in this step, 3 levels were introduced per treatment attribute. Of note, attributes with major differences between known characteristics of ET treatment and abemaciclib + ET treatment were prioritised. This model was then taken forward to the qualitative phase for further refinement. Based on desk research, input from a cross-functional team as well as feedback from a patient testimonial, attributes in Fig. 1 were taken forward to the qualitative phase.
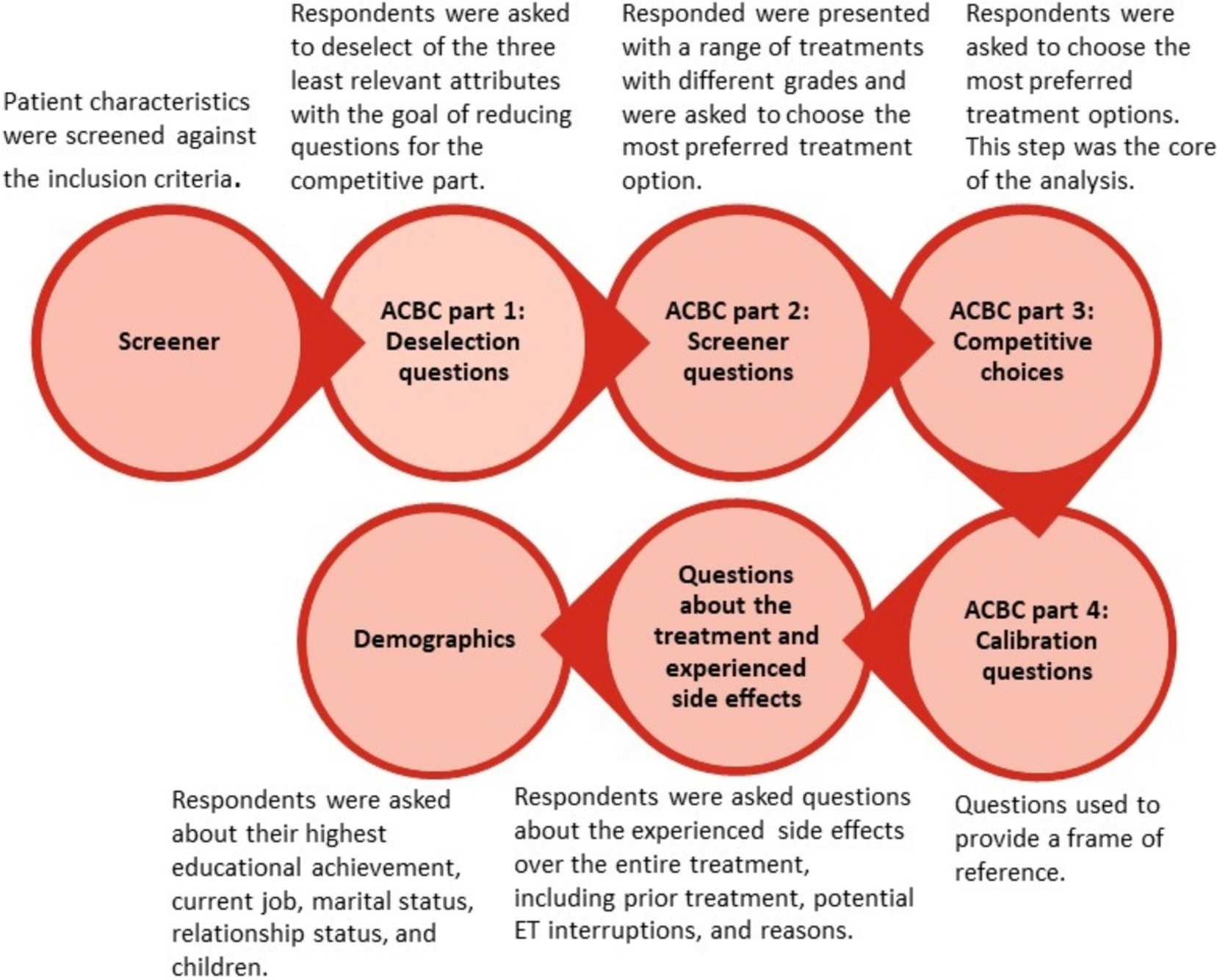
Fig. 1
ACBC analysis questionnaire breakdown. ET; endocrine therapy, QoL; quality-of-life, ACBC; Adaptive Choice-Based Conjoint analysis
Qualitative phaseIn the subsequent qualitative part of the project, the initial model of the treatment decision was further developed by means of guided semi-structured interviews with physicians (n = 6 gynaecologists and n = 6 oncologists), patients (n = 20), and caregivers (n = 5) between July 2nd and August 9th, 2021. Included physicians were recruited from both hospitals and from office-based practice and were actively participating in decision-making for EBC treatment. Patients’ selection criteria were as follows: at least 18 years old, high-risk HR + /HER2- EBC, defined as having received (neo)adjuvant chemotherapy, completed surgery ± radiotherapy, and ongoing adjuvant ET (for max. 10 years) or completed it no more than 6 months ago. To ensure that the eligibility criteria were met, a screening questionnaire was conducted via a telephone call with the recruitment centre of the agency. For patient characteristics, please refer to Suppl. Table 1.
Additionally, this step identified 2–3 levels for all attributes based on the insights from the desk research, the cross-functional discussions, and side effects profiles of drugs available for adjuvant ET of HR + Her2- EBC or standing shortly before market introduction for this indication, which at that time point were ET alone and abemaciclib in combination with ET. For the quality-of-life attributes, the levels “barely restricted” (level 1), “restricted” (level 2), and “severely restricted” and for side effects attributes, the levels “mild/low” (level 1),”moderate/intermediate “ (level 2), and “severe/high” (level 3) were defined (regarding diarrhoea, in both the absolute and relative assessment phases, the patients were informed that it was expected mainly at the start of treatment and is usually easy to manage, which is in accordance with diarrhoea observed with abemaciclib). Treatment modalities comprised 3 attributes: “restrictions/caution when taken with other drugs (co-medication)” with the grades: “barely restricted” (level 1), “restricted” (level 2), and “severely restricted” (level 3), “frequency of taking drug” with the grades “1 × per day” and “2 × per day” and “number of follow-up appointments and time required (effort/monitoring)” with the levels “check-up appointments every 3 months” and “check-up appointments: month 1–2: every 2 weeks, month 3–4: 1 × per month, and as of month 5: every 3 months”.
For the subsequent quantitative phase, the attributes and levels were critically reviewed in a cross-functional workshop to reduce the complexity to be able to use the method of conjoint analysis. In addition, it was considered whether the respective attributes and the levels of the attributes are different for the available treatment options in the market. Findings of the qualitative phase were employed to develop a conjoint matrix (table showing the number of attributes including the levels for each attribute, e.g. in Table 1) that was used as the basis of the subsequent quantitative online survey.
Table 1 Attributes and levels employed in the conjoint analysisQuantitative phaseThe quantitative phase consisted of web-assisted phone surveys with the option of self-administered 30-min online survey based on the ACBC analysis. Surveys were conducted with 85 patients between 25th October 2021 and 2nd March 2022. Inclusion criteria for the quantitative phase were similar to the qualitative, with the only exception that patients with the adjuvant ET planned were also included. Patients responded to an announcement via various channels mentioned above, additionally via social media (Instagram und Facebook) and advocacy groups.
A screening was conducted online with questions relevant to test eligibility programmed before the main questionnaire. Only patients who qualified were forwarded to the main questionnaire. For patients’ characteristics, please refer to Suppl. Table 2.
In the adaptive choice-based conjoint method, respondents were presented a range of choice-based tasks where treatments were distinctly described with properties (attributes) of different intensity according to the list in Table 1. This method is reactive meaning that the respondents’ answers or choices from previous questions impact the treatment options and characteristics (attributes) subsequently presented.
The ACBC method comprises 4 phases (Fig. 2):
(1)In phase 1, patients were presented with a list of nine variable treatment characteristics (attributes) (Table 1) and were asked to pick those three that would be least relevant for them when deciding for or against ET. Being the central goal of treatment, the tenth attribute (relapse risk reduction) could not be deselected as “least relevant for the decision”. The characteristics were presented according to the first column (“Attributes”) from Table 1 without the grades from the second column. During the survey, the selected and deselected attributes were not shown again, so the burden of answering was further reduced for each individual respondent.
(2)In phase 2, treatment options with various attributes and levels (e.g. attribute physical fitness and activity, level hardly restricted and attribute diarrhoea, level 1–3 times per day above baseline) were presented to the patients, who had to decide separately whether the treatment options would be basically acceptable or whether they would refuse to endure it with the goal of screening treatments for the following phase.
(3)Phase 3 was the core conjoint measurement where respondents were offered pairs of treatment alternatives and had to choose the most acceptable treatment options. This competitive choice phase helped to build the preference structure of the ACBC analysis.
(4)In the final phase, the respondents were presented with 4 adapted treatment options based on previous choices with the purpose of preference calibration. Respondents were asked how likely they were to select each respective treatment choice (calibration question). This phase served to identify the relative relevance of each attribute.
Fig. 2
Attributes recommended for the qualitative phase
Conjoint analysisDuring the screening phase and the choice task tournament, 85 respondents completed 2566 tasks in total, i.e. they made 2566 decisions average of 30 decisions per respondent. Based on the individual utility values*, the likelihood of the chosen alternative being selected was determined for each of these tasks. The likelihood product across all tasks and respondents resulted in the likelihood value which was the basis for the model fit quality criteria.
In the screening phase and during the choice task tournament, respondents always had to choose between two alternatives (either treatment is an option yes/no or a choice of treatment). The Root likelihood (RLH) which reflects the mean likelihood for the actually chosen alternatives based on the individual utility values was 79.2%. The higher the RLH, the better the selection behaviour of respondents is reflected by the estimated utility values. At 79.2%, the RLH is noticeably higher than the 50% to be expected with a random selection.
The model fit was measured by McFadden’s R2 which is part of the pseudo-R2 measures. The percent certainty is 0.664 which means a very good fit of the model.
The likelihood ratio (LR) enables testing the null hypothesis that all parameters are zero. The LR is 2,363.12 and asymptotically χ2-distributed. Due to p < 0.001, the null hypothesis has to be rejected.
*Utility values describe which attribute levels have the biggest or lowest “worth” (benefit) for respondents compared to the other levels of the same attribute. The specific utility values of the various attribute levels are calculated on the basis of the frequency with which the respondents decide in favour or against treatment profiles with the specific attribute levels in the context of the conjoint task. If the utility values of all levels of an attribute (for all respondents) are zero or in other words: if there is no trend across all respondents towards choosing a therapy with a certain level of an attribute (e.g. “1–3 × diarrhea “), this would mean that the respective attribute has no relevance for the patient’s decision.
Comments (0)