Comparison of baseline data between the two patient groups
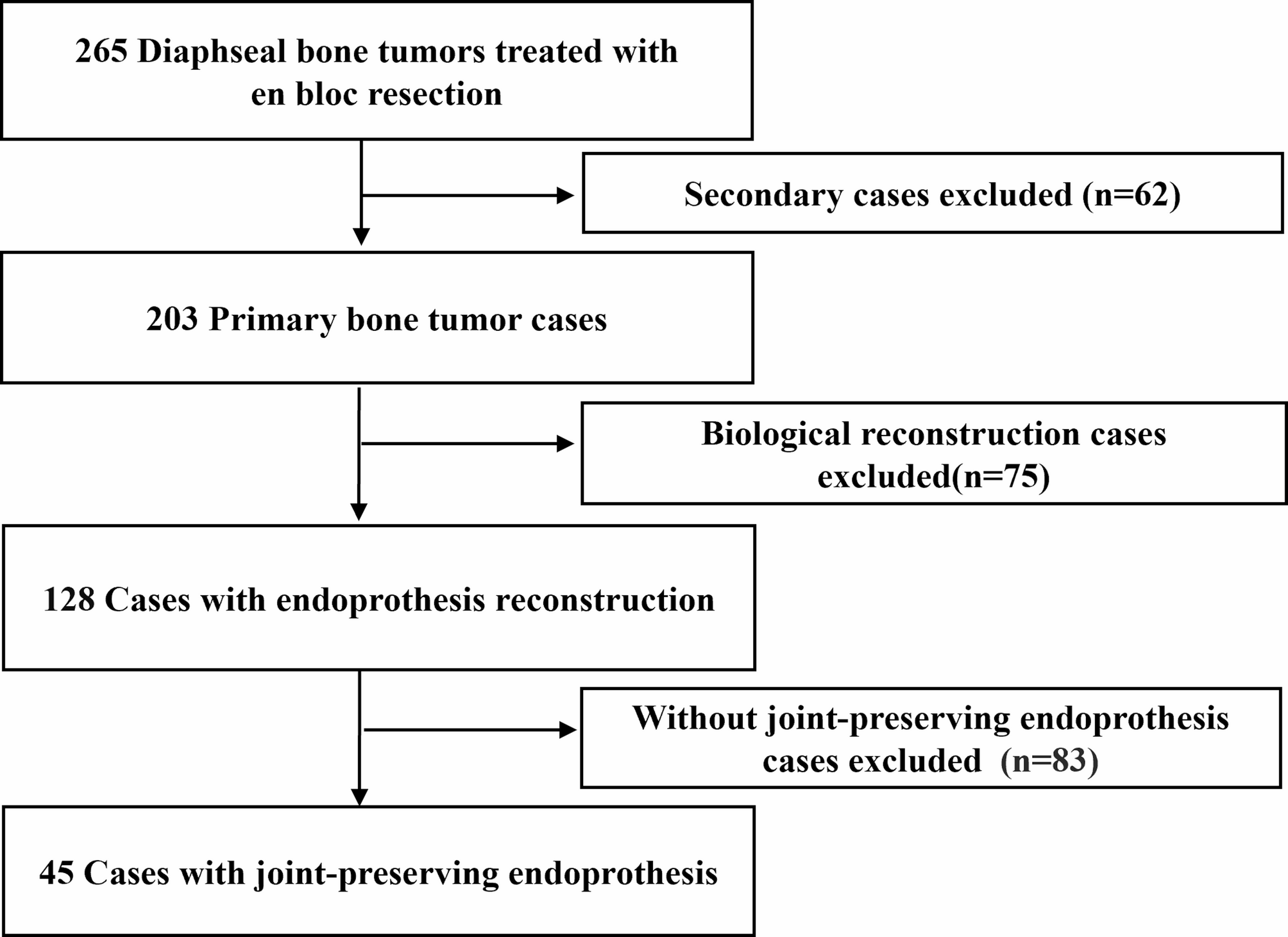
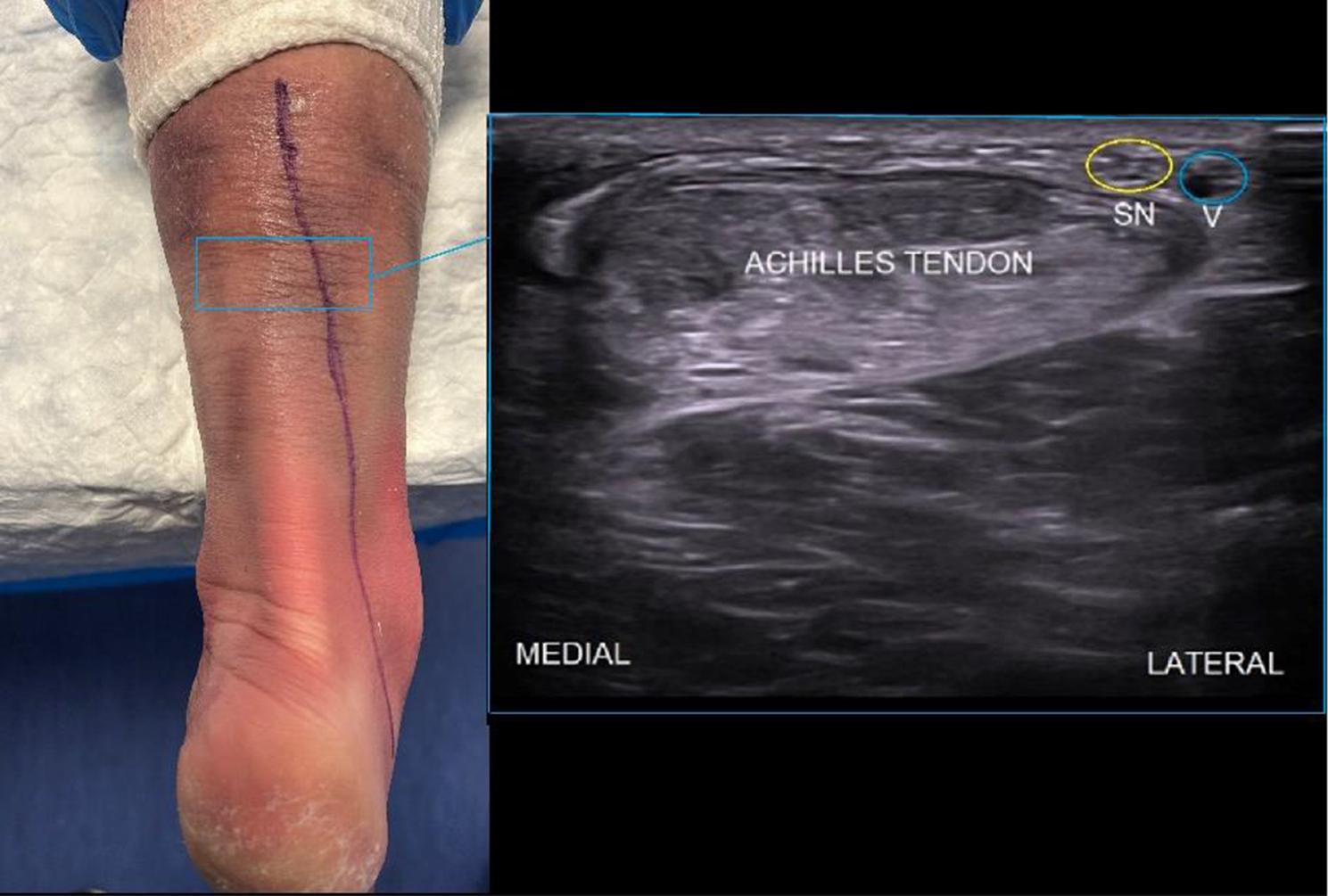
A total of 147 patients were included in this study, of whom 117 were male and 30 were female, with an average age of 43 (36, 56) years. The causes of injury included 73 traffic accidents, including 52 wheel spoke injuries and 21 other traffic accidents; 36 crush injuries; 38 mechanical injuries; all injuries were open injuries. The area of the limb soft tissue defect was classified according to the Meyerson classification: Type I in 34 patients, Type II in 77 patients, and Type III in 36 patients. Open Achilles tendon defect wounds with infections were observed in 42 patients, whereas 105 patients had simple defects. All 147 patients were followed up for a period of 12– 36 (25.6 ± 1.8) months. All surgical incisions healed in the first stage without infection. Three months after surgery, colour Doppler ultrasound revealed good continuity of the Achilles tendon, with no complications, such as rerupture. Ten weeks after surgery, ankle dorsiflexion was 0°, and patients could walk in regular shoes without discomfort. At the final follow-up, the flap appearance was satisfactory, with good softness and elasticity and no scar contracture or significant pigmentation. The flap could withstand some degree of friction during walking and daily activities and had regained a protective sensation. All patients could perform single-leg heel raises and were satisfied with the surgical results. No complications, such as rerupture, delayed incision healing, incision nonhealing, infection, deep vein thrombosis, sensory reduction, Achilles tendon pain, Achilles tendon contracture, Achilles tendon laxity, or muscle hernia, were observed, and there were no abnormalities in the movement of the donor limb. The patients were divided into a one-stage reconstruction group (81 patients) and a staged reconstruction group (66 patients). Baseline data, such as age, sex, height, body weight, calculated body mass index, injury site (left or right), injury type (Myerson classification), length of Achilles tendon defect, area of skin and soft tissue defect, Achilles tendon thickness, surgery time, suture removal time, cause of injury, and presence of infection, were compared between the two groups (see Table 1 for details). The test results revealed that, except for differences in the length of the Achilles tendon defect and the areas of the skin and soft tissue defects (tL = 4.749, PL < 0.001; tS = 5.170, PS < 0.001), other baseline data did not significantly differ between the groups (P > 0.05).
Table 1 Comparison of baseline data and leading observation indicators between the two groupsComparative Analysis of Long-term Ankle Joint Function Between the Two Groups of Patients
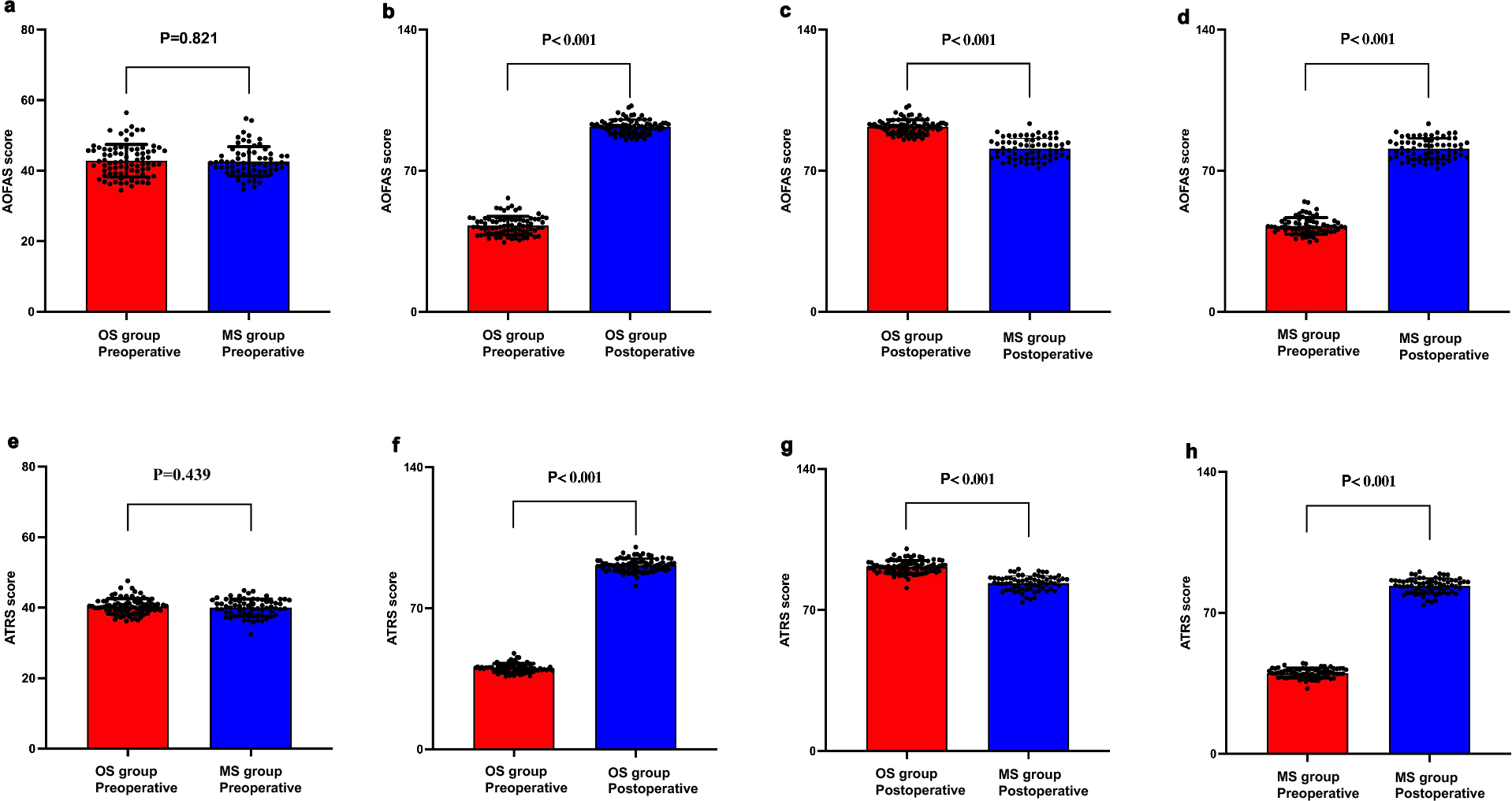
A comparative analysis of the long-term postoperative follow-up ankle joint function scores of the two groups of patients (Table 2) revealed that the postoperative follow-up ankle joint function scores of the one-stage reconstruction group were significantly better than those of the staged reconstruction group (PAOFAS < 0.001; PATRS < 0.001). Further comparative analysis of the two microsurgical methods within the one-stage reconstruction repair group (Table 3) revealed no significant difference in the overall postoperative follow-up ankle joint function scores (PAOFAS = 0.792; PATRS < 0.001). However, in terms of daily activities, walking ability on uneven surfaces, ability to ascend stairs quickly, abnormal gait, plantar flexion and dorsiflexion, inversion and eversion, the one-stage technique of free flap transplantation of the descending genicular artery with the adductor magnus tendon was superior to the vascular anastomosed fascia lata free anterolateral thigh perforator flap transplantation. Additionally, the two surgical methods were compared in the staged surgery group. The results (Table 4) of long-term follow-up of ankle joint function in patients revealed that the one-stage gastrocnemius neurocutaneous flap combined with a two-stage peroneus longus muscle tendon transfer with the lateral calcaneal artery was superior to the one-stage gastrocnemius neurocutaneous flap combined with a two-stage flexor hallucis longus tendon transfer (PAOFAS < 0.001; PATRS < 0.001).
Table 2 Comparison of American Orthopedic Foot–Ankle Society scores and Achilles Tendon total rupture scoresTable 3 Comparison of American Orthopedic Foot and Ankle Society scores and Achilles Tendon total rupture scores between the two one-stage surgical treatment subgroupsTable 4 Comparison of American Orthopedic Foot and Ankle Society scores and Achilles Tendon total rupture scores between the two traditional surgical reconstruction subgroups Correlation analysis of the Achilles tendon defect length, area of skin and soft tissue defects in the heel region, degree of wound infection, Meyerson classification, and postoperative follow-up ankle joint function score (ATRS score, AOFAS score)
The correlations among the degree of preoperative wound infection, classification of heel area injury, size of the defect area in the heel region, length of the Achilles tendon defect, and a series of clinical characteristics with postoperative follow-up data related to ankle joint function were evaluated. The results (Figs. 3, 5) revealed that the classification of heel area injury (P < 0.001), the size of the defect area in the heel region (PAOFAS < 0.001, RAOFAS = -0.397; PATRS < 0.001, RATRS = -0.436), and the length of the Achilles tendon defect (PAOFAS < 0.001, RAOFAS = -0.429; PATRS < 0.001, RATRS = -0.280) were correlated with postoperative ankle joint function in the affected limb, whereas preoperative wound infection was not correlated with postoperative ankle joint function (PAOFAS = 0.690, PATRS = 0.759).
Regression analysis results of factors affecting postoperative ankle joint function
The results of univariate logistic regression analysis for each variable (Tables 5 and 6) revealed significant differences among the groups of variables, including the surgical method, the length of the Achilles tendon defect, and defect area of the heel area of the affected limb (P < 0.05). Collinearity diagnostic analysis of the above indicators revealed no collinearity among the indicators (variance inflation factor < 10). Further multifactorial logistic regression analysis revealed (Tables 5 and 6) that the surgical method (OR = 49.725, 95% CI: 16.996 ~ 145.478) and defect area of the heel region (OR = 0.947, 95% CI: 0.903 ~ 0.992) were independent risk factors affecting patients’ long-term follow-up ankle joint function postoperatively.
Table 5 Univariate and multivariate analyses of the logistic regression results for the Achilles tendon total rupture scoreTable 6 Univariate and multivariate logistic regression analyses of American Orthopedic Foot and Ankle Society scoresDiscussion
The skin and soft tissue of the heel area are thin and have poor mobility[9], making them prone to necrosis and defects after trauma, which can lead to the exposure of deep tissues, such as the Achilles tendon, bone, and joints. Improper handling can easily result in infection and osteomyelitis, requiring multiple surgeries and leading to a high disability rate[10]. In Achilles tendon reconstruction surgery, consideration must be given to restoring the shape of the Achilles tendon while maintaining its original biomechanical structure, requiring the graft material to be wear resistant[11]. The unique functional and anatomical characteristics of the heel region demand high standards for the appearance, stability, wear and pressure resistance, and sensory requirements of the repaired skin and soft tissue. The reconstruction of Achilles tendon defects combined with surrounding tissue loss presents a significant challenge. Currently, a wide variety of surgical options are available for repairing open Achilles tendon defects, both domestically and internationally. However, no unified criteria for indications and contraindications have been established[12]. Traditional treatments often involve flap coverage of soft tissue defects in the heel area, followed by secondary Achilles tendon reconstruction. Although this approach reduces the difficulty of surgery, it results in an extended treatment cycle, with old Achilles tendon repairs being complex and more prone to complications, such as tendon adhesion, stiffness, severe retraction, and increased postoperative infection rates[13]. Since Taylor et al. applied the anastomosed vascular iliac-inguinal composite flap for the repair and reconstruction of Achilles tendon and heel region soft tissue composite defects in 1979[14], setting a precedent for one-stage repair of composite tissue defects in the heel area with free composite tissue, one-stage repair has been increasingly applied in clinical practice. Some scholars have compared the postoperative pathological tissue of the Achilles tendon in patients who have undergone different surgical methods: in patients with one-stage Achilles tendon repair, postoperative inflammatory infiltration in the Achilles tendon tissue is not significant and anatomical landmarks are clear, whereas in patients undergoing staged surgery, fibrous scar proliferation at the Achilles tendon stump, reduced elasticity and toughness, and loss of moisture are observed[15]. Although one-stage repair requires specific microsurgical techniques and has greater surgical complexity, it can reduce the occurrence of complications in secondary reconstruction[2]. This study compared the long-term postoperative follow-up ankle joint function scores between the two groups of patients (Table 2). The results revealed that the postoperative follow-up ankle joint function scores were significantly better in the one-stage repair group than in the staged reconstruction group (PAOFAS < 0.001; PATRS < 0.001). Additionally, logistic regression analysis was performed on various variables (Tables 5 and 6), and the results revealed that the surgical method (OR = 49.725, 95% CI: 16.996 ~ 145.478) was an independent risk factor affecting the postoperative ankle joint function of patients. One-stage microsurgical repair allows for precise repair of damaged tissues, promoting early regeneration and repair of Achilles tendon cells. This approach effectively avoids the challenges of reconstructing and repairing neglected Achilles tendon defects, meeting the current requirements for ideal Achilles tendon repair and reconstruction surgery: the healing period should not be excessively long; otherwise, local adhesion and inflammation can affect Achilles tendon function. The repaired area should have appropriate local tensile strength soon after surgery, thus facilitating early functional exercise of the patient's ankle joint. Clinicians should strive to choose one-stage repair for open Achilles tendon defects to reduce the degree of psychological trauma and economic burden on patients, resulting in greater social benefits.
Traditional free anterolateral femoral flap repairs are bloated in appearance, and patients often face problems such as low flexibility of the ankle joint, poor dorsiflexion and plantar flexion function of the affected foot, difficulty wearing shoes, and the need for a second surgery to thin the flap. In contrast, the repair of Achilles tendon defects using descending genicular artery free flap transplantation with the adductor magnus tendon has the following advantages: a consistent anatomical donor site, sizeable external diameter of the blood vessels, long vascular pedicle, minimal damage to the donor site, and a relatively thick and close shape and tensile strength to the standard Achilles tendon. While repairing the Achilles tendon and skin defects, it is even possible to reconstruct the insertion point of the Achilles tendon. In addition, the reconstructed skin of the heel region is smooth and has a good appearance, and the flap is thin, thus facilitating wearing of the shoe with good abrasion resistance [16]. In this study, the two microsurgical repair methods in the one-stage reconstruction repair group were further compared. The results (Table 3) revealed no significant difference in the overall postoperative follow-up ankle joint function score (PAOFAS = 0.792). However, in terms of daily life, the ability to walk on uneven surfaces, the ability to climb stairs quickly, abnormal gait, plantar flexion and dorsiflexion, and inversion and eversion, descending genicular artery free flap transplantation with the adductor magnus tendon was superior to vascular anastomosed fascia lata free anterolateral thigh perforator flap transplantation. This finding shows that the traditional anterolateral thigh free flap has advantages in repairing sizeable soft tissue defects in open Achilles tendon defects. For patients with small soft tissue defects, the use of descending genicular artery free flap transplantation with the adductor magnus tendon results in better ankle joint flexibility postoperatively. This finding suggests that when one-stage microsurgical repair and reconstruction are selected for open Achilles tendon defects, the choice of the one-stage microsurgical procedure should be based on the characteristics of the injury in the heel region to optimise the prognosis of the patient's affected limb function.
Achilles tendon reconstruction and repair can be categorised into two types: those with a blood supply and those without a blood supply. Some scholars have conducted meta-analyses comparing these two surgical methods and have suggested that the use of tendon grafts with a blood supply can promote the healing of the Achilles tendon ends. Soft tissue with good vascularization covering the tendon can improve the wear resistance and gliding ability of the Achilles tendon [17]. Other scholars have conducted comparative studies using New Zealand rabbits to repair Achilles tendon defects with vascularised peroneus longus muscle tendon grafts. The transplanted tendons were repaired with a vascularised peroneus longus muscle tendon, and the tendons showed minimal adhesion to the surrounding tissue and good sliding function. Their tensile strength reached 67.7% of that of a standard Achilles tendon, and their stiffness was similar to that of a standard Achilles tendon. The tensile strength of the reconstructed tendon without vascularization is only 35.5% of that of a standard Achilles tendon, and its stiffness is far from that of a standard Achilles tendon[18]. Achilles tendon repair with a vascular supply is undoubtedly advantageous and has become the consensus of most scholars. In this study, we compared and analysed the long-term ankle joint function of patients who underwent staged surgical repair via two sub-microsurgical methods. The results (Table 4) revealed that the long-term ankle joint function of patients who underwent second-stage peroneus longus muscle tendon transfer with the lateral calcaneal artery was superior to that of patients in the second-stage nonvascularised flexor hallucis longus tendon transfer group (PAOFAS < 0.001; PATRS < 0.001). These results are consistent with the descriptions of the aforementioned scholars. In the repair of Achilles tendon defects, having a reconstructed tendon with a rich blood supply is crucial for a good patient prognosis. A healthy blood supply undoubtedly promotes granulation tissue formation and the proliferation of Achilles tendon fibroblasts, accelerates both exogenous and endogenous repair processes, facilitates early healing of the Achilles tendon, reduces adhesions with surrounding tissues, and aids in the early recovery of movement and gliding functions of the Achilles tendon. Selecting a tendon graft surgical method with an adequate blood supply is important, and efforts should be made during the surgery to preserve the paratenon (tendon sheath and microvessels) to the greatest extent possible to protect the blood supply of the Achilles tendon.
Basic research indicates that in the repair process of Achilles tendon injuries, type III collagen, which has regenerative repair functions, predominates in the scar at the severed end. The scar tissue gradually transforms into tendon-like tissue, which can be seen as a transformation from newly formed type III collagen fibres to mature type I collagen fibres [19]. The regenerative repair capacity of type III collagen fibres is closely related to the abundance of surrounding skin and soft tissue[20]. In other words, a smaller injury and fewer soft tissue defects indicate stronger ability to produce new type III collagen fibres. Other scholars have indicated that in patients with large areas of heel region damage, the collagen fibres in the reconstructed area are sparse, disorganised, curved, and poorly aligned. In contrast, patients with smaller damaged areas have denser collagen fibres in the reconstructed area, with more organised fibre structures, and the fibre orientation aligns with the longitudinal direction of the tendon [21]. This study revealed (Fig. 5) a negative linear correlation between the area of heel defects and the long-term postoperative ankle joint function score of patients. Multivariate regression analysis revealed (Tables 5 and 6) that the defect area in the heel region is an independent risk factor for long-term postoperative ankle joint function in patients (PARTS = 0.023, ORARTS = 0.947, 95% CI: 0.903 ~ 0.992), indicating that the area of the heel region defect plays an important role in assessing the severity of open Achilles tendon defects and predicting postoperative function. Therefore, during the intraoperative repair of soft tissue defects around the heel, repairing the deep soft tissue bed and peritendinous membrane of the Achilles tendon, as well as filling significant soft tissue defects around the heel with flaps as much as possible, is beneficial for Achilles tendon healing.
Reasonable tension and periodic stress promote tendon healing [22]. Some scholars believe that the length of the Achilles tendon defect directly correlates with the loss of type I collagen fibres, the repair time, the and tension load used to directly anastomose the two ends of the Achilles tendon. If repaired through grafting or transfer surgery, the reconstructed Achilles tendon conduction chain often differs significantly from the biomechanical conduction of the original chain, making it more challenging to maintain appropriate cyclical tension and resulting in poorer healing [23]. In this study, the length of the Achilles tendon defect was linearly and negatively correlated with the patient's postoperative ankle joint function score (Fig. 5). In the multivariate regression analysis (Tables 5 and 6), the length of the Achilles tendon defect was shown to be an independent risk factor affecting the patient's postoperative ankle joint function (PAOFAS = 0.013, ORAOFAS = 0.731, 95% CI: 0.570 ~ 0.937). Appropriate cyclical stress can coordinate various healing mechanisms at the microscopic level and improve the structural reconstruction of Achilles tendon tissue. Excessive Achilles tendon defects, whether end-to-end anastomosis or transfer grafting, lead to excessive tension load or cyclical stress disorders, which affect patient prognosis. Therefore, the length of the Achilles tendon defect plays an important role in the assessment of injury during Achilles tendon reconstruction and in postoperative functional prediction. During Achilles tendon repair surgery, efforts should be made to restore the original biomechanical conduction chain of the Achilles tendon. When the defect length is significant, tendon grafting or transfer reconstruction should be used to prevent excessive anastomotic tension and poor prognosis. A certain amount of tension should also be maintained during anastomosis to avoid laxity.
Clinical classifications usually guide surgical treatment, and the Myerson classification divides Achilles tendon defects into the following: type I, with defects less than 2 cm in size; type II, with defects between 2 and 5 cm in size; and type III, with defects more than 5 cm in size[24]. The analysis of the correlation of the Achilles tendon injury classification (Fig. 3) in this study revealed that patients with higher-grade injuries had lower long-term postoperative ankle joint function scores than those with lower-grade injuries. Indeed, the length of the Achilles tendon defect and the defect area in the heel region are important criteria for assessing the severity of Achilles tendon defects according to the Myerson classification. Therefore, we believe that the Myerson classification is correlated with long-term postoperative ankle function in patients, likely because of differences in the length of the Achilles tendon defect and the defect area of the heel region. Patients with open Achilles tendon defects have thin skin around the heel region and poor blood supply. After suffering high-energy injuries, they are prone to ischaemia and necrosis, which subsequently lead to wound infection. If flap coverage treatment is not applied, the patient’s prognosis is usually poor. This study analysed the correlation between preoperative wound infection and long-term postoperative ankle joint function in the affected limb (Fig. 4). The results revealed no correlation between the two scores (PAOFAS = 0.690, PATRS = 0.759). Because the duration of preoperative infection in patients with open Achilles tendon defects does not exceed 4 weeks, its impact on the prognosis may be minimal. Of course, we cannot rule out systematic errors due to the small sample size.
Currently, the comparability of various studies on the repair of open Achilles tendon defects, both domestically and internationally, is relatively low. The evaluation indicators are primarily subjective and lack objective evaluation criteria. Among the few literature reports with objective evaluation standards, most are single-centre retrospective studies with small sample sizes, which limits the role of statistical analysis.





Comments (0)