
Remember me
Delirium is an acute brain dysfunction induced by physical illnesses or medications, which cannot be explained by dementia or other neurocognitive disorders.1 Delirium is observed in 23% of hospitalized elderly patients.2 Delirium is associated with various poor outcomes such as increased mortality,3 extended hospital stays,3 increased incidence of dementia,4 and decreased cognitive function.3 To date, antipsychotics have been the mainstay of pharmacologic treatment for delirium. A recent meta-analysis of 58 randomized controlled trials (RCTs) demonstrated the effectiveness of quetiapine and the combination of haloperidol and lorazepam in the treatment of delirium.5 However, antipsychotics can induce various side effects, including extrapyramidal symptoms, QT prolongation, and neuroleptic malignant syndrome.6 Elderly patients are particularly susceptible to these side effects,7 and antipsychotics increase the risk of mortality in elderly patients and those with dementia.8–10 Therefore, developing pharmacologic treatment with few side effects for delirium is a critical challenge.
Several studies have examined the efficacy of non antipsychotic sedative drugs in preventing and treating delirium. The meta-analysis revealed a significant preventive effect of melatonin and melatonin receptor agonists on delirium.11 A recent RCT demonstrated a numerical, but not statistically significant, superiority of an orexin receptor antagonist, suvorexant, over placebo for the prevention of delirium.12 Dexmedetomidine has been repeatedly reported to be effective in preventing and treating delirium in critically ill patients13; however, adverse events such as hypotension and bradycardia are concerning. Regarding the treatment of delirium with non-antipsychotic drugs by oral administration, a meta-analysis of RCTs showed that melatonin reduced the duration of delirium and the use of additional rescue medications.14 In addition, several retrospective observational studies reported that suvorexant, trazodone, and mianserin were effective for delirium.15–17 Nonetheless, pharmacologic treatment options for delirium remain limited.
Hydroxyzine is a first-generation antihistamine, introduced in the 1950s, with various formulations including injectables. As hydroxyzine has a sedative effect and is widely used as hypnotics and anxiolytics,18,19 it could be used for the treatment of delirium. Nevertheless, few studies have examined the effect of hydroxyzine on delirium. In a literature search using PubMed with the keywords of “delirium” AND “hydroxyzine,” 15 records were identified and 2 of the studies involved adult patients with delirium. One is a retrospective study that involved 497 patients with cancer and delirium, showing no difference in the time to delirium resolution or the frequency of detrimental incidents between intravenous administration of haloperidol 5 mg alone and that of haloperidol 5 mg plus hydroxyzine 25 mg.20 The other retrospective study including 39 adult patients with overactive delirium also found no significant difference in the rate of or time to delirium improvement between intravenous or subcutaneous administration of haloperidol 5 mg alone and haloperidol 5 mg plus hydroxyzine 25 mg.21 However, these 2 studies examined a combination of hydroxyzine and haloperidol in palliative care settings. In this study, we performed a retrospective study to compare the effects of intravenous hydroxyzine and haloperidol monotherapy on delirium. We hypothesized that hydroxyzine would be comparable to haloperidol for the treatment of delirium.
METHODS Study Design and SettingWe conducted a retrospective study of inpatients at Keio University Hospital from April 1, 2017, to September 30, 2022, who received intravenous hydroxyzine or haloperidol as monotherapy for the treatment of delirium. At Keio University Hospital, we use an algorithm for the prevention and treatment of delirium in clinical practice since 2021 to avoid excessive use of antipsychotics, considering their side effects particularly for elderly patients. Our algorithm recommends the use of ramelteon before the onset of delirium, followed by suvorexant/lemborexant, trazodone/mianserin, and quetiapine/levomepromazine after the onset. Before 2021, hydroxyzine was rarely used for the treatment of delirium. After 2021, according to the algorithm’s recommendation of the use of intravenous hydroxyzine before haloperidol when oral administration was difficult, hydroxyzine gradually came into use. When both drugs were used in the same episode of delirium, data were extracted only for the first drug administered. Patients were excluded if they met any of the following criteria: (1) receiving concomitant administration of antipsychotics, orexin receptor antagonists (ie, suvorexant and lemborexant), melatonin receptor agonists (ie, ramelteon), sedative antidepressants (ie, trazodone and mianserin), or oral administration of hydroxyzine or haloperidol; (2) receiving simultaneous intravenous administration of hydroxyzine and haloperidol; (3) receiving intravenous hydroxyzine or haloperidol before the onset of delirium; (4) receiving hydroxyzine or haloperidol not for the treatment of delirium (eg, use as antiemetics or antiallergics); (5) having benzodiazepine withdrawal delirium; (6) being at high risk of alcohol withdrawal delirium (defined as consumption of >60 g of pure alcohol per day); and (7) receiving a single administration of hydroxyzine or haloperidol for only 1 day, not for 2 or more consecutive days.
AssessmentAt Keio University Hospital, trained nurses assessed the risk of developing delirium before or at the time of admission for all inpatients, including (1) aged 70 years or older; (2) definitely or suspectedly diagnosed with dementia, (3) having a history of delirium, (4) having a history of stroke, (5) receiving benzodiazepines, or (6) drinking more than 60 g of pure alcohol per day. When a patient at high risk for delirium was admitted, the nurse further assessed for the presence of direct factors for delirium: acute infection, hyperinflammation, acute hyper or hyponatremia, hypoxemia, hypercapnia, and use of drugs as a risk of delirium. For patients with direct factors for delirium or suspected delirium, nurses assess the Confusion Assessment Method (CAM)22 or Confusion Assessment Method for the Intensive Care Unit (CAM-ICU)23 twice a day in the morning and evening, until the CAM or CAM-ICU result becomes negative for 3 consecutive days. In this study,the diagnosis of delirium was defined as a positive result of CAM or CAM-ICU, and the date of delirium onset was defined as a day when the CAM or CAM-ICU result became positive.
Data ExtractionThe following information was extracted from medical records: date of birth, sex, date of admission, date of discharge, diagnosis of baseline primary illness, presence of surgery, date of surgery, presence of dementia, degree of alcohol use, presence of steroid use, date of delirium onset, date of delirium improvement or censoring, reason for censoring, doses of hydroxyzine and haloperidol on the first day, duration of treatment with hydroxyzine or haloperidol, maximum doses of hydroxyzine and haloperidol during the treatment, outcome at discharge, and reason for using intravenous administration.
Statistical AnalysisThe primary outcomes were the time from administration of hydroxyzine or haloperidol to delirium improvement and the rate of delirium improvement. Patients were censored if they met any of the following criteria: (1) discontinuing hydroxyzine or haloperidol while CAM or CAM-ICU is still positive, (2) discharge from the hospital, (3) death, and (4) switching to another drug for treating delirium from intravenous hydroxyzine or haloperidol (in cases with drug switching, we also extracted whether the switching from intravenous to oral drugs was due to the resumption of eating and drinking). Improvement of delirium was defined as a negative result of CAM or CAM-ICU for 3 consecutive days. The time to delirium improvement was estimated using the Kaplan Meier method and compared between hydroxyzine and haloperidol using a log-rank test and Cox regression analysis with age and sex as covariates. The rate of delirium improvement was calculated for each drug and compared by using χ2 test. Additional analysis was conducted, excluding cases with switching to oral drugs due to the resumption of eating and drinking, which satisfies both of the following 2 conditions: (1) being prohibited from eating and drinking at the time of initiation of hydroxyzine or haloperidol administration, and (2) switching to other drugs within 24 hours after resuming eating and drinking. Patient linicodemographics were compared between the 2 groups using χ2 and t-tests for categorical and continuous variables, respectively. All tests were 2-tailed, with a significance level of 5%. IBM SPSS Statistics version 29.0 (IBM Corporation, Armonk, NY, USA) was used for analysis.
Ethical ConsiderationsThis study was approved by the institutional review board at Keio University School of Medicine. This study was conducted in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived due to the retrospective study design.The study information was posted on the website, giving participants an opportunity to opt out.
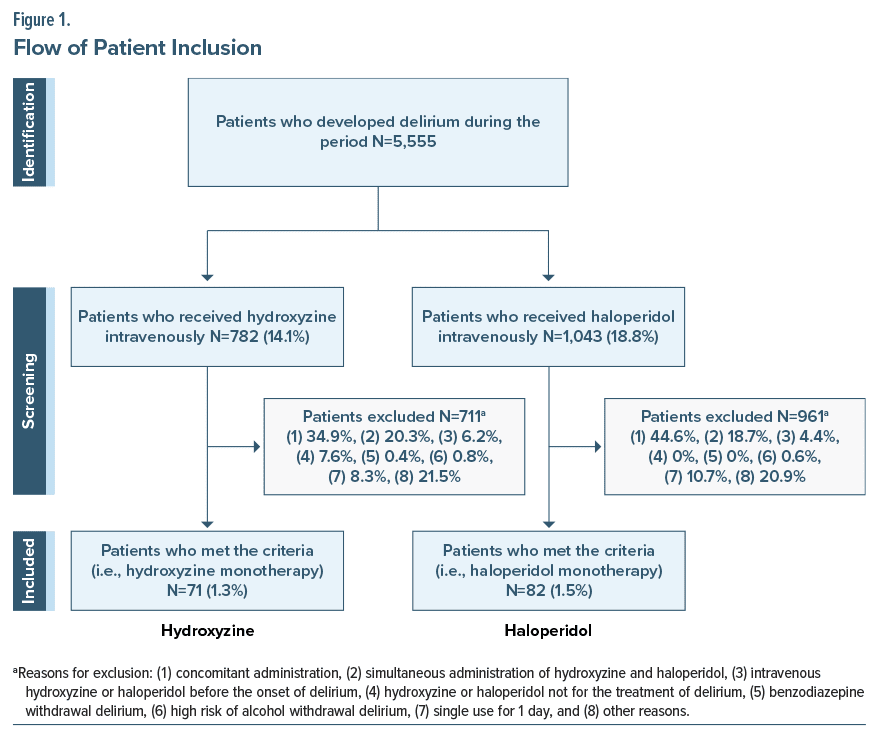
RESULTS Patient ClinicodemographicsAmong 5,555 patients who developed delirium during the study period, 782 (14.1%) and 1,043 (18.8%) patients received intravenous hydroxyzine and haloperidol, respectively. A total of 71 (1.3%) and 82 (1.5%) patients met the eligibility criteria for hydroxyzine and haloperidol as monotherapy for the treatment of delirium, respectively, and were included (Figure 1). The primary reasons for exclusion were as follows: (1) concomitant use of ramelteon, suvorexant, lemborexant, hydroxyzine, trazodone, mianserin, and/or antipsychotics (34.9% for hydroxyzine and 44.6% for haloperidol), (2) simultaneous administration of hydroxyzine and haloperidol (20.2% for hydroxyzine and 18.7% for haloperidol), and (3) single administration of hydroxyzine or haloperidol for only 1 day, not for 2 or more consecutive days (8.3% for hydroxyzine and 10.7% for haloperidol), in that order. Primary diseases for hospitalization were shown in Supplementary Table 1. As only 1 patient in the hydroxyzine group was hospitalized with COVID-19 (Supplementary Table 1), the impact of COVID-19 can be considered negligible in the study population. Hydroxyzine was used in approximately 90% of cases after 2021, while haloperidol was used in approximately 90% of cases before 2021 (Supplementary Figure 1). This reflects the fact that the first choice of intravenous drugs used for delirium has shifted through the years. The mean ages of patients included in this analysis were 75.2 ± 14.9 years for hydroxyzine and 76.4 ± 14.0 years for haloperidol. The proportions of patients who were 65 years or older were 76.1% (n = 54) for hydroxyzine and 84.1% (n = 69) for haloperidol. There were no significant differences in patient clinicodemographics between the 2 groups (Table 1).
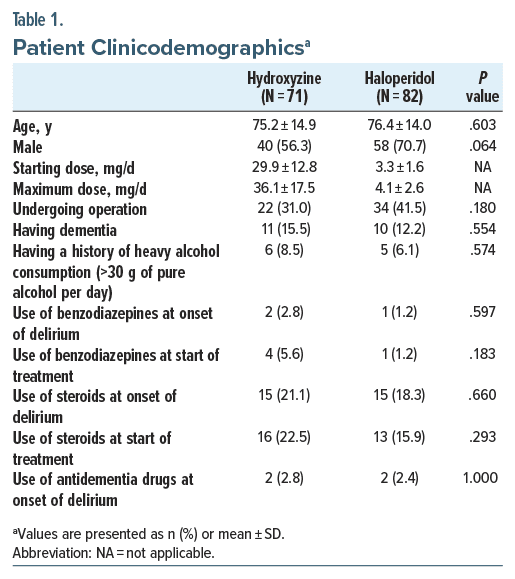
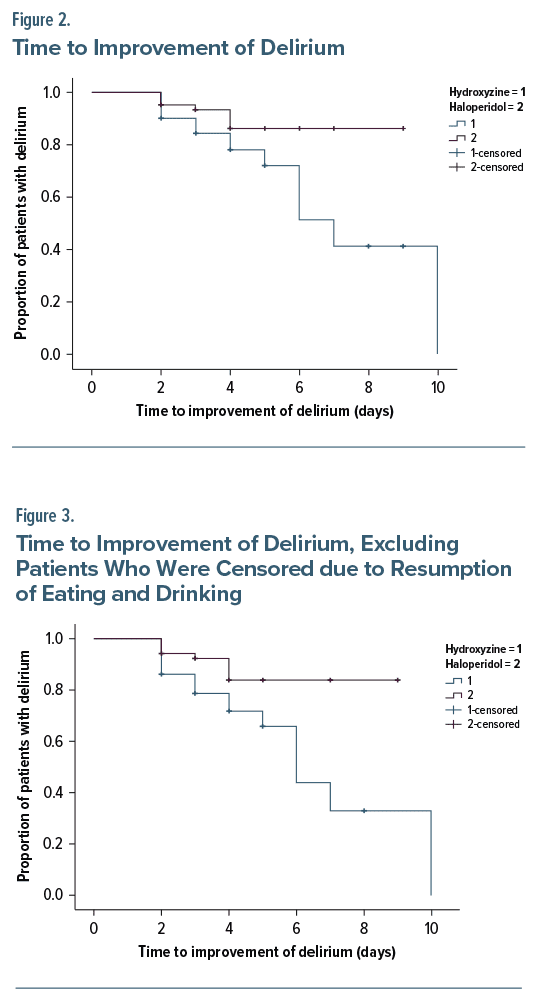
The time to delirium improvement was numerically in favor of hydroxyzine (mean, 7.0 days; 95% CI, 5.7–8.3 days) over haloperidol (mean, 8.2 days; 95% CI, 7.6–8.8 days), despite no significant difference (P = .059) by a log-rank test. The hazard ratio by the Cox regression analysis was 0.45 (95% CI, 0.18–1.11) with no significant difference between the 2 groups (P = .081) (Figure 2). On the other hand, the rates of delirium improvement were 23.9% (n = 17) for hydroxyzine and 8.5% (n = 7) for haloperidol, with a significantly higher improvement rate in the hydroxyzine group (P = .009). The mean doses of hydroxyzine and haloperidol on the first day were 29.9 mg/d and 3.3 mg/d, respectively. The mean maximum doses of hydroxyzine and haloperidol were 36.1 mg/d and 4.1 mg/d, respectively (Table 1).
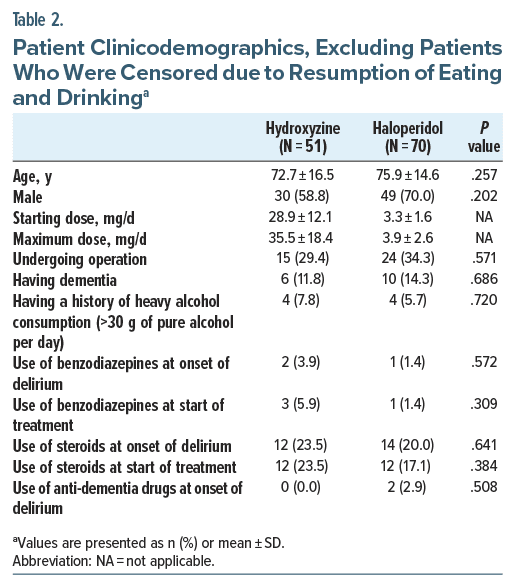
A total of 20 patients in the hydroxyzine group and 12 patients in the haloperidol group were identified as cases with switching to other drugs due to resumption of eating and drinking. Thus, 51 cases in the hydroxyzine group and 70 cases in the haloperidol group were included in the additional analysis (Table 2). The time to delirium improvement significantly differed between the hydroxyzine group (mean, 6.5 days; 95% CI, 5.2–7.8 days) and the haloperidol group (mean, 8.1 days; 95% CI, 7.4–8.8 days), with the hydroxyzine group improving more difference between the 2 groups (P =.055) (Figure 3). Also, the rates of delirium improvement were 33.3% (n=17) for hydroxyzine and 10.0% (n=7) for haloperidol, with a significantly higher improvement rate in the hydroxyzine group (P=.001).
This is the first study to examine the effect of intravenous monotherapy of hydroxyzine for treating delirium, showing that hydroxyzine had a significantly higher rate of delirium improvement than haloperidol, with no significant difference in the time to delirium improvement. Given that the time to delirium improvement was numerically in favor of hydroxyzine, a larger sample size may have resulted in a significantly shorter time to delirium improvement with hydroxyzine than haloperidol. These findings suggest that hydroxyzine could be a promising alternative to antipsychotics for treating delirium.
Hydroxyzine is a first-generation antihistamine that crosses the blood-brain barrier and affects the tuberomammillary nucleus in the posterior hypothalamus, an arousal center.24 A study using positron emission tomography revealed that hydroxyzine 30 mg occupied approximately 70% of histamine H1 receptors,25 which is almost equivalent to quetiapine 25 mg and olanzapine 2.5 mg, as known as sedative antipsychotics. This pharmacologic feature of hydroxyzine may be associated with its sedative and anxiolytic effects. Indeed, a meta-analysis found that hydroxyzine improved sleep onset and overall sleep quality for insomnia in adults.18 Another meta analysis showed that hydroxyzine improved anxiety symptoms better than placebo in generalized anxiety disorder.19 Although the exact mechanism of hydroxyzine for delirium is unknown, the sedative and anxiolytic effects may contribute to improvement of delirium.
It is well known that first-generation antihistamines, such as diphenhydramine,26 have anticholinergic effects, which could induce or exacerbate delirium. However, whether hydroxyzine also has anticholinergic effects has to be judged based on solid scientific evidence. The Beers criteria, widely used as a guide for drug use in the elderly, have long recommended avoiding hydroxyzine due to its strong anticholinergic effect.27 The Anticholinergic Risk Scale,28 Anticholinergic Cognitive Burden,29 and Anticholinergic Drug Scale30 all classify hydroxyzine as the highest point or level of 3, indicating a strong anticholinergic effect. Additionally, the US package insert for hydroxyzine notes that it has an anticholinergic effect. On the other hand, surprisingly, several studies have indicated a very low binding affinity of hydroxyzine to muscarinic receptors. One in vitro study found that Ki value of hydroxyzine at 100 mg/kg to muscarinic receptors was >10,000.31 Other studies showed hydroxyzine’s Ki value of 3,800 vs diphenhydramine 20) in bovine cerebral cortex and 4,600 (vs diphenhydramine 310) in human caudate nucleus.32,33 Also, cetirizine, the major active metabolite of hydroxyzine, has a high selectivity for histamine H1 receptors and almost no binding to other receptors.34 Thus, the evidence clearly demonstrates negligible anticholinergic effects in hydroxyzine. Considering that quetiapine, which has a very low affinity for dopamine D2 receptors and a high affinity for histamine H1 receptors, is effective for delirium,5 the primary mechanism of pharmacologic treatment for delirium may involve the sedative action associated with blockade of histamine H1 receptors, not only dopamine D2 receptors. Especially in the elderly, dopamine D2 receptor blockade should be avoided because of the risk of extrapyramidal symptoms,6 which can cause falls and fractures as well as dysphagia and pneumonia.35,36 Our results suggest that blockade of histamine H1 receptors may be important in the treatment of delirium; in addition to hydroxyzine, drugs with high affinity of histamine H1 receptor, such as trazodone and mianserin,37 may be candidates for the treatment of delirium shown in a recent study.17
Previous reports suggest that hydroxyzine has low adverse events. A meta-analysis of RCTs found no significant difference in study discontinuation due to side effects or side effects between hydroxyzine and placebo in patients with generalized anxiety disorder.19 Another systematic review of hydroxyzine for insomnia found that only 1 of 5 studies reported adverse events of hydroxyzine18; the study was an RCT in which hydroxyzine, prazosin, and placebo were administered for insomnia with posttraumatic stress disorder and showed no significant adverse events between hydroxyzine and placebo, despite the dose of hydroxyzine being as high as 100 mg/d.38 In contrast, haloperidol can induce various adverse events, including extrapyramidal symptoms.39 Moreover, some studies revealed that haloperidol caused cognitive impairment in healthy adults even at single doses of 3–5 mg.40–42 However, as this study did not examine adverse events, investigation is needed to examine the safety of hydroxyzine in patients with delirium.
This study has several limitations. First, this is a retrospective study, which could have confounding bias. The choice of hydroxyzine or haloperidol may have been biased by the doctor’s arbitrary decision based on their preferences and experiences. The type of severity of physical diseases is also not considered. However, as shown in Supplementary Table 1, the periods during which haloperidol was administered and those during which hydroxyzine was administered were differentiated after the algorithm was introduced. Regardless of the severity of delirium, before the introduction of the algorithm, haloperidol was the first choice for the treatment of delirium at Keio University Hospital, but it was replaced by hydroxyzine after the introduction of the algorithm. Second, among the total 5,555 patients, only 71 patients (1.3%) for hydroxyzine and 82 patients (1.5%) for haloperidol were included in the analysis. The subjects may not represent the overall population of delirium. Third, we did not investigate the adverse effects of hydroxyzine. Caution is advised regarding the occurrence of drowsiness when hydroxyzine is used for elderly patients. Thus, the findings should be considered preliminary and prospective studies are warranted to examine the efficacy and safety of hydroxyzine monotherapy in the treatment of delirium.
Despite these limitations, we first showed that intravenous hydroxyzine monotherapy was not inferior for the time to delirium improvement and superior for the rate of delirium improvement to intravenous haloperidol monotherapy. Considering that hydroxyzine is relatively safe with few side effects, including anticholinergic effects, and can be administered intravenously, intramuscularly, or orally, it can be a viable option for delirium as an alternative to antipsychotics.
Article InformationPublished Online: January 6, 2025. https://doi.org/10.4088/JCP.24m15569
© 2025 Physicians Postgraduate Press, Inc.
Submitted: August 18, 2024; accepted October 7, 2024.
To Cite: Kubo K, Takehara M, Hirata M, et al. Effects of intravenous hydroxyzine versus haloperidol monotherapy for delirium: a retrospective study. J Clin Psychiatry. 2025;86(1):24m15569.
Author Affiliations: Department of Neuropsychiatry, Keio University School of Medicine, Tokyo, Japan (Kubo, Huh, Uchida, Takeuchi); Division of Drug Informatics, Keio University Faculty of Pharmacy, Tokyo, Japan (Takehara, Hirata); Department of Nursing, Keio University Hospital, Tokyo, Japan (Kawano).
Corresponding Author: Hiroyoshi Takeuchi, MD, PhD, Department of Neuropsychiatry, Keio University School of Medicine, 35 Shinanomachi, Shinjuku-ku, Tokyo 160-8582, Japan ([email protected]).
Author Contributions: Concept and design: (Takeuchi); data extraction: (Kubo, Kawano, Takehara, Hirata); acquisition, analysis, or interpretation of data: (Kubo, Huh, Takehara, Takeuchi); drafting of the manuscript: (Kubo, Huh, Takehara, Takeuchi); critical revision of the manuscript for important intellectual content: (Uchida); statistical analysis: (Kubo, Takehara); administrative, technical, or material support: (Takeuchi); supervision: (Takeuchi).
Relevant Financial Relationships: Dr Kubo has received a grant from Inogashira Hospital; speaker fees from Sumitomo Pharma; and manuscript fees from Wiley. Dr Kawano has received speaker fees from Eisai. Dr Uchida has received grants from Daiichi Sankyo, Eisai, Mochida, Otsuka, and Sumitomo Pharma; speaker fees from Boehringer Ingelheim, Eisai, Lundbeck, Meiji Seika Pharma, MSD, Otsuka, and Sumitomo Pharma; and consulting from Boehringer Ingelheim, Lundbeck, Sumitomo Pharma, and Takeda. Dr Takeuchi has received grants from Daiichi Sankyo, Novartis Pharma, and Otsuka; speaker fees from EA Pharma, Eisai, Janssen, Kyowa, Lundbeck, Meiji Seika Pharma, Mitsubishi Tanabe Pharma, MSD, Otsuka, Sumitomo Pharma, Takeda, and Yoshitomiyakuhin; and consulting fees from Boehringer Ingelheim, Janssen, Mitsubishi Tanabe Pharma, Ono, and Sumitomo Pharma. Mss Takehara and Hirata and Mr Huh declare no conflicts of interest.
Funding/Support: None.
Use of AI-Assisted Technologies: In the writing of this manuscript, the authors used AI for proofreading the manuscript. The authors have reviewed the content and take full responsibility for the content of the publication.
Supplementary Material: Available at Psychiatrist.com.
Comments (0)