
Remember me
English physician and anatomist Nathaniel Highmore (1614-1685), Danish anatomist Thomas Bartholin (1616-1680) and Genovese Theophile Bonet (1620-1689) reported on various cases of “fatal black tumor”.[12–14] In 1775, Pervicall Pott (1714-1788) made surgical observations relative to the cancer of the scrotum. He was the first scientist to demonstrate that a cancer may be caused by environmental carcinogen. He identified soot as the cause of chimney sweeps scrotal cancer, later called testicular cancer.[15] In 1820, William Norris was the figure to describe the first instance of melanoma and mentioned the relation of melanoma with heredity. He surgically removed a mole of a 59 years old male between umbilicus and the pubes. Unfortunately, the lesion recurred 6 weeks later. The father of this man died of a similar disease about 30 years ago and the youngest son had the same sign in the same spot where the disease in his father initially appeared.[16] French anatomist Gilbert Breschet (1784-1845) made during 1821 a series of clinical observation on melanoma, stating that is a disease appearing to other species too, mentioning the dog, the cat, the rabbit, the rat, the mouse and the horse.[17] In 1834, David Williams described a melanoma as a shoulder’s black spot, developing first horizontal and then vertical.[18,19] Robert Carswell (1793-1857), professor of pathology at the University College of London, described the post-mortem findings of an old man brought to the Hotel Dieu of Paris (Figure 2).[20] In 1838 Isaac Patrish documented the first North American case of melanoma which was a tumor on the foot. In 1838, Scottish expert in pathological anatomy Robert Carswell (1793-1857) introduced the term melanoma in the medical nomenclature in his book “Illustrations of the elementary forms of disease”. He classified the lesions of melanoma in true melanosis and spurious melanosis. He illustrated melanoma metastasis form a cutaneous melanoma of a 70 years old male patient with metastasis in the brain and Ileum after autopsy.[18,19,21,22] In 1844, English surgeon Samuel Cooper (1780-1848) who was coined with the term “melanotic cancer”, highlighted that “the only chance for cure of melanoma depend upon the early removal of the disease, so that to prevent any metastasis”.[19] In 1853, James Paget (1814-1899) recorded 25 cases of “melanoid cancer” and noted once more the development of superficial to vertical spread of melanoma. In 1857, Jonathan Hutchinson (1828-1913), a British surgeon who described melanotic freckle, which is now known as lentigo maligna. In 1885, melanuria was described by Tennent.[23] In 1858, Oliver Pemberton (1825-1897) stated the color changes that a melanoma causes in the skin (Figure 3). He had also recorded that the available on the era treatments were ineffective.[24,25] Surgeon Maurice Henry Collins (1824-1869) in 1864 classified melanosis in fibrinous or simple, cancerous and cystic, noting that not all cases belong to cancer or all fatal (Figure 4).[26] Ten years after Pemberton, in 1868, German pathologist, physiologist and biologist Paul Langerhans (1847-1888) published a description of “branched cells of the skin” that stained with gold chloride.[27] American surgeon John Ashhurst (1839-1900) in 1871 noted that melanotic cancer usually occurs as a separate mass instead of an infiltration, having as favorite localities the skin and the subcutaneous tissue.[28] In 1873, Thomas Bryant (1828-1914) suggested that melanotic cancer always grows from a part which naturally contains pigment.[29] Scottish pathologist William Aitken (1825-1892) said that melanotic cancer consists of encephaloid or soft cancer, with the addition of black or brownish pigment.[30] In 1886, American physician Austin Flint (1812-1886) suggested that most melanotic cancers were in reality melanotic sarcomata.[31] In 1887 German Dieterich P. gave a detailed statistical review of 145 patients reported between the years 1864 to 1881.[32] In the 20th century, advances in microscopy, pathology, immunology, genetics, and molecular biology enabled more accurate and detailed diagnosis of melanoma. In 1903, Eve Frederick Samuel (1853-1916) advocated in far or of wide excision and elective regional node dissection. In 1905, William Sampson Handley (1872-1962) recommended the excision of subcutaneous fat of melanoma for about 2 inches in all directions. In 1911, Rous Sarcoma Virus (RSV), a retrovirus that causes tumors in chickens had been used as a model for studying cancer. The discovery or RSV by American pathologist at the Rockefeller University Francis Peyton Rous (1879-1970) in 1910 opened the field of tumor virology and led to the discovery of oncogenes.[25]
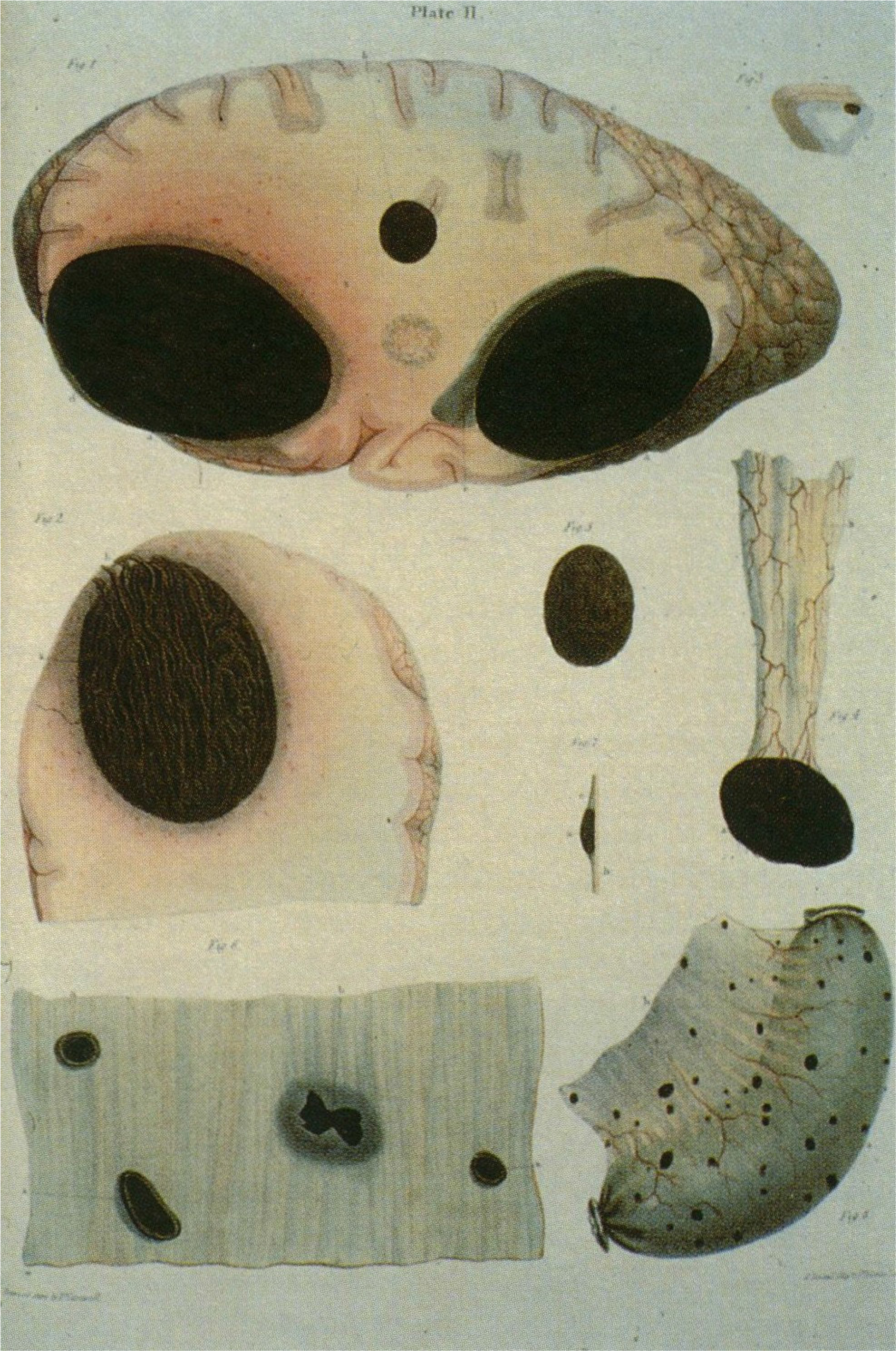
Figure 2:
Breschet’s illustrations of post-mortem finding of a metastatic melanoma case, from within “Considerations sur une alteration organique apelde degenerescence noire milanose, cancer milani”, 1821.

Figure 3:
Melanoma of the face in a 53 years old male from Pemberton’s on Melanosis, 1858.
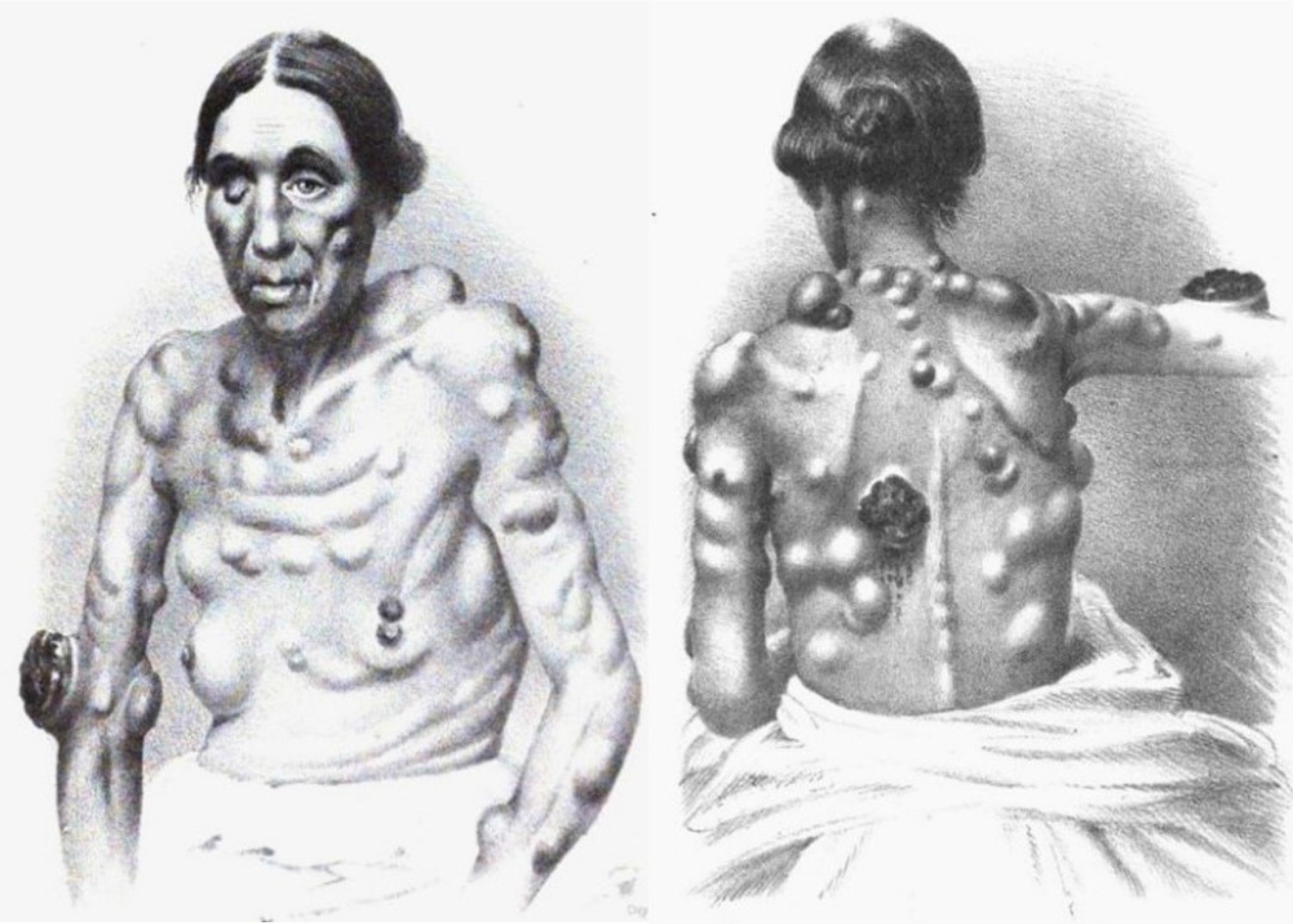
Figure 4:
Female patient with melanotic cancer from Maurice Henry Collins’ on the diagnosis and treatment of cancer and the tumours analogous to it, 1864.
Surgeon and historian Walter George Spencer (1858-1940) from the Westminster Hospital, delivered in November 1923 the Bradshaw Lecture “On melanosis”, reviewing current thinking on the chemical formation of melanin, adding though the in vogue clinical management of the disease.[33] In 1956, Henry Lancaster made a series of observations in Caucasians and reported the relation of sunlight and the incidence of melanoma. Nelson and Lancaster exposed the interaction of 5 skin characteristics, skin color, texture, hair color, eye color and reaction to sun in melanoma expression.[25] Wallace Clark (1924-1997) was an American dermatologist and pathologist who is best known for the description of the “Clark’s level”, or “Clark level system” for classifying the seriousness of a malignant melanoma skin cancer based on its microscopic appearance. The method measures the depth of penetration of a melanoma into the skin according to anatomic layer, categorizing 5 Clark levels of invasion.[20] Alexander Breslow was a pathologist at George Washington University medical center who first reported depth of invasion as a prognostic factor in melanoma in 1970. In recognition of his contribution, the depth of invasion of melanoma is referred to by the eponym Breslow’s depth.[34] Dr. Donald L. Morton was a pioneer in the field of oncology and made significant contributions to the management of cancer patients worldwide. One of his major contributions was the development of the sentinel node biopsy for melanoma, which improved the staging of the disease in 1977. Morton and his colleagues at UCLA medical center developed the first lymphoscintigraphy technique using radio-labeled colloidal gold.[35]
Comments (0)