
Remember me









Our findings revealed that the EZ invariably contained lesions and surrounding cortices in patients with LEATs. However, when it came to the TPO area, especially with a long history of epilepsy and other abnormalities on MRI, such as hippocampal sclerosis and focal cortical dysplasia. SEEG could be useful in evaluating whether distant brain tissues (particularly mesial temporal structures) were included in the EZ.
In patients with LEATs, glioneural origin is thought to produce a predominant direct effect through hyperexcitable regions of dysplastic neurons inside the tumor itself. Gliomas do not have intrinsic neural components; hence, epileptogenesis must be caused by tumor infiltration into the surrounding cortex, which indirectly affects the surrounding neural networks [18]. There is good evidence to suggest that “solitary” glioneural tumors are correlated with localized cortical dysplasia [11]. The interictal discharges of LEATs have been demonstrated to be more extensive than those in other lesions, such as hippocampal sclerosis, and can extend to the contralateral side [19]. There are three viewpoints on the relationship between LEATs and the adjacent dyslaminated or dysplastic cortex: the first is that the tumor and adjacent dysplasia are the same lesion, the second is that the tumor and the putatively dyslaminated surrounding cortex are separate lesions (dual pathology), and the third is that only the solid tumor is the lesion with the adjacent cortex being irrelevant [20].
In this study, all tumors were located in the temporal lobe, and the patients underwent extended resection with the guidance of SEEG. Why did we perform an extended resection? The following were the reasons to support our view: epilepsy surgery relied on clinical, anatomical, and EEG features to identify the EZ. To date, there has been no consensus on the definition of the EZ. The most widely used definition has been “the minimum amount of cortical tissue that must be resected to produce seizure-freedom”. EZ is not a static area, but can change with time; specifically, EZ contains actual ictal-onset zone and the potential ictal-onset zone. French/Italian researchers assumed that cortical cortex involved in early spreading area are part of the potential seizure-onset zone and therefore, should be resected. Currently, it has been recognized that intracranial EEG during seizures is still the gold standard for locating EZ. [21, 22].
The surgical strategy for LEATs is still debatable, and no prospective study specifically examining the role of tumor resection has been conducted. Total resection of the EZ is necessary for successful surgical treatment of epilepsy, and the EZ often contains tumors, varying amounts of surrounding tissue, and even remote areas [12]. Ghareeb and Duffau [23] pointed out that hippocampal resection allowed seizure control in patients with intractable epilepsy generated by a paralimbic grade II glioma, even if the tumor did not invade the hippocampus. As a result, according to the SEEG monitoring results, we resected areas including seizure onset and early spreading areas. If the lesions were not adjacent to functional areas, the likelihood of being seizure-free was maximized.
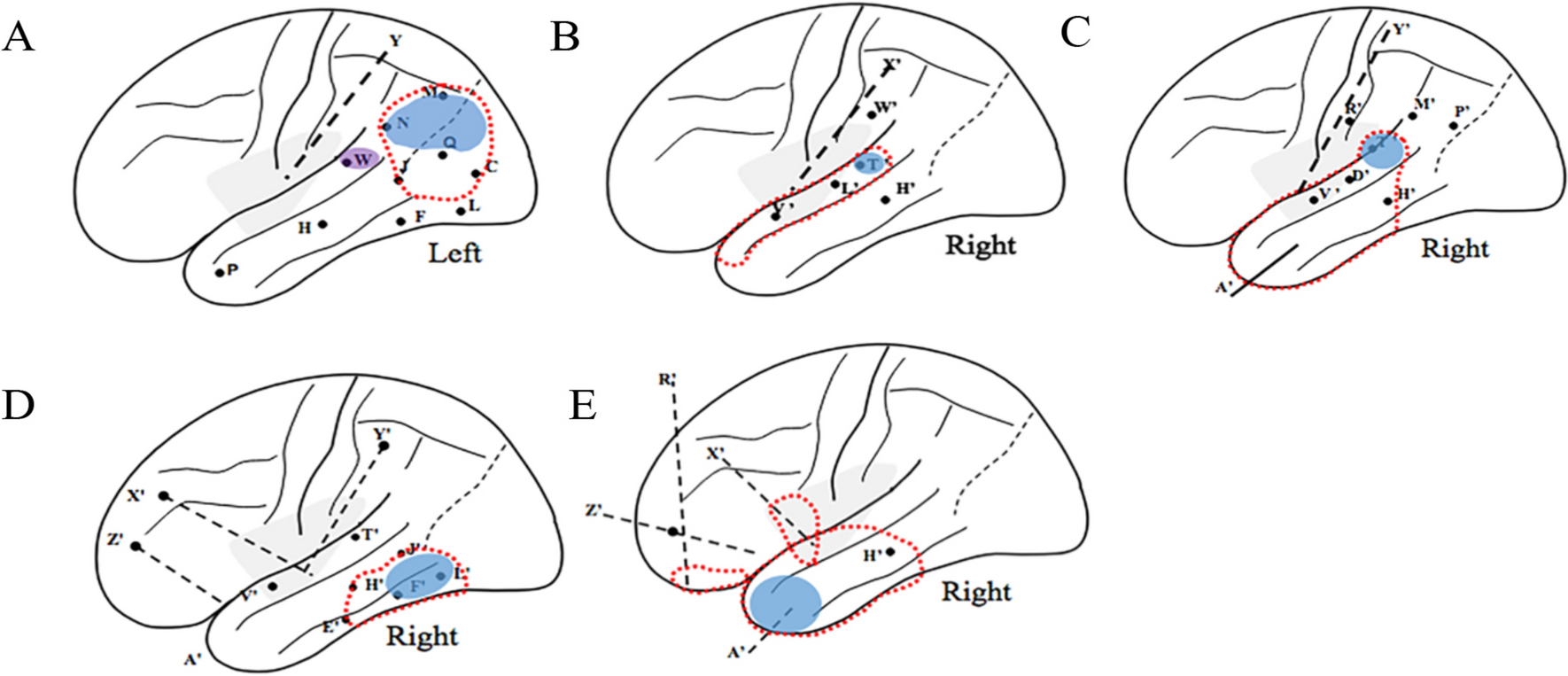
Our experience of LEATsIn case 5 (Table 1, Fig. 2), a temporal pole lesion was found on MRI, and the daily seizures caused the patient’s melancholy. Because of the extensive hypometabolic area on 18F-FDG PET scan and high signals in the hippocampus, amygdala, posterior orbital frontal cortex, and anterior insular cortex, which prevented doctors from identifying the boundary of the EZ, we implanted electrodes into suspected areas. SEEG monitoring revealed that before clinical seizure, A '10–14 (temporal pole)/H' 10–13 (middle temporal neocortex)/X '1–5 (anterior insular cortex)/Z' 1–5 (posterior orbitofrontal cortex) were initiated simultaneously, but the A '10–14 showed nearly continuous intermittent discharge during the preictal phase, which was more prominent. Therefore, both anterior insular cortex and posterior orbitofrontal cortex should be included in the EZ. Second, based on cytoarchitectonic analyses, the insula has been subdivided into “granular”, “dysgranular” and “agranular” sectors. Posterior orbital frontal cortex, anterior insular cortex and anterior medial temporal part were homologous in cortical development and all of them were classified as agranular cortex. In fact, there was no specific boundary between the ventral insula and orbital cortex. The so-called temporal, insular, and frontal lobes were only classified according to gross anatomy, and it was quite possible that epileptic lesions existed across the cerebral lobes [24,25,26,27], we confirmed that the lesion, hippocampus, amygdala, anterior insular cortex, and posterior orbital frontal cortex were involved in the EZ. After complete resection of the EZ, the patient remained seizure-free for 24 months.
Fig.2
Tumor was in the temporal pole, but epileptogenic zone involved temporal structures, anterior insular cortex and orbitofrontal cortex (case 5). A 15-year-old boy suffered from intractable epileptic seizures since 10 years old. MRI showed that the tumor was located in the temporal pole and the hippocampus presented higher signal than the contralateral side. Stereoelectroencephalography (SEEG) revealed the seizure onset was in the lesion (A’10–14). After seizure onset, the discharge spread quickly into the amygdala (A’1–5), the hippocampus (H’1–3), the insular cortex (X’1–5) and the orbital frontal cortex (Z’1–5), and then the neocortex of the lateral temporal lobe (H’10–13) was also involved. A, B Preoperative MRI; C, D Preoperative 18F-FDG PET in interictal period; E, F Postoperative MRI; G Ictal SEEG; H 3D brain map
In case 3 (Table 1, Fig. 3), MRI revealed that the tumor was located in the right superior temporal gyrus, with hippocampal sclerosis in the medial temporal lobe. SEEG monitoring results showed that the seizure onset zone was in the right hippocampus, with the anterior insular cortex and the lesion being an early spreading area. The patient denied any history of febrile convulsion, and the resection range included the lesion, temporal cortex, hippocampus, and anterior insular lobule. Finally, the patient remained seizure-free for 25 months postoperatively. In cases 1 and 2, however, the lesion was also in the TPO regions, but the EZ only contained the lesion and the adjacent cortex. We hypothesized that hippocampal ischemia caused by a long history of epilepsy (30 years) renders it a secondary EZ, with the formation of a new epileptogenic network [28].
Fig.3
Tumor was in the right superior temporal gyrus, but epileptogenic zone involved mesial temporal structures and anterior insular cortex (case 3). A 45-year-old man suffered from intractable epileptic seizures since 10 years old. MRI showed that the lesion was located in the right superior temporal gyrus, with high signal in hippocampus. Stereoelectroencephalography (SEEG) revealed the seizure onset was in the amygdala (A’1–5) and the hippocampus (H’1–3). After seizure onset, the discharge spread into the anterior insular cortex (V’1–5) and the tumor (T’3–6). A, B Preoperative MRI; C, D Preoperative 18F-FDG PET in interictal period; E, F Postoperative MRI; G Ictal SEEG; H 3D brain map
Electrocorticogram (ECoG) and SEEG: when and how we choose?Although ECoG-guided resection might increase the likelihood of long-term seizure-free status [29, 30], others argued that ECoG did not increase the probability of seizure freedom in children when compared with lesionectomy alone [31, 32]. Because the intraoperative ictal activity is rarely recorded while utilizing ECoG, resection margins are usually determined using interictal data [33]. Some researchers have reported that gross total resection was a significant predictor of good outcomes [34,35,36,37,38]. Therefore, SEEG is essential for identifying the resection boundaries in complicated cases. The question is when we need to use SEEG to identify the EZ. Rosenow et al. [11] believed that intracranial EEG was necessary only if the lesion could not be completely resected due to an adjacent or overlapping eloquent cortex. In our perspective, the treatment of LEATs should be considered as epilepsy surgery, and the following are the indications for SEEG based on our experience: First, the data on the location of the tumor as well as the anatomical, electrophysiological, and clinical data, implied that the EZ might far beyond the scope of the lesion. For example, in case 3, the lesion was located in the right superior temporal gyrus with hippocampal sclerosis on MRI. Moreover, the lesion, parietal operculum, insular lobe, and medial and lateral temporal lobes showed hypometabolism on the interictal 18F-FDG PET scan, the scalp EEG demonstrated only the right hemisphere, while we could not differentiate the origin of epilepsy (insular lobe, lesion, temporal lobe, or parietal operculum). Therefore, we decided to perform SEEG electrode implantation on the patient. In addition, the lesion was adjacent to eloquent areas, such as the primary motor area or language area. Finally, when the tumor is located in the neocortex of the temporal lobe (especially the TPO area), with a long clinical history (> 1 year), abnormalities on MRI, such as hippocampal sclerosis and focal cortical dysplasia, and extensive hypometabolism area on18F-FDG PET scan [39], it is difficult to decide whether mesial temporal structures should be included in the resection, particularly in the dominant hemisphere.
LimitationsOur retrospective single-center approach has inherent limitations. The limited sample size precludes definitive results, and it is possible that the results found here do not generalize to a broader population of relevant patients. Large-sample prospective investigations are required to determine the association between EZ and LEATs. Moreover, the aim of this study was not only to address the efficacy of SEEG for some special LEATs, but also establish proof-of-concept for a new treatment approach for LEATs. The new framework presented in this article could advance and enhance the mechanism understanding and treatment of LEATs. Some studies have demonstrated that epileptogenicity can affect remote regions which are distant from the lesion site in patients with FCD or tumors [12, 13]. Although this is accordance with our findings, more cases are needed to verify the conclusions. However, because of the high medical costs and risk of electrode implantation, every case is valuable in china, the sample size of patients continues to increase slowly.
Comments (0)