Depression is a common psychiatric condition, and over 700,000 deaths by suicide occur worldwide annually [1]. In the USA, deaths from suicide are approaching 50,000 annually, with 12.3 million adults seriously considering suicide in just 1 year [2, 3]. Studies in the USA reveal that nearly half of those who died by suicide were seen in the health care system within the 4 weeks preceding their death, but the majority of these patients did not have a mental health diagnosis [4, 5]. Patients who die by suicide are more likely to have been treated by a primary care physician than a psychiatrist [6], indicating that training in suicide prevention should not be reserved for psychiatrists but should be accessible for all physicians, especially those in primary care. Unfortunately, depression and suicide remain stigmatized, creating barriers for both patients and health care providers to discuss it [7, 8]. Indeed, gaps in training about suicide prevention remain for many health care providers, and there is a need for implementation of evidence-based practices, such as the Zero Suicide Model [9]. Together, these findings indicate that the lack of provider comfort and competence is serious and pervasive.
Future physicians need better training for identifying and intervening with patients at risk of suicide. Guidelines on suicide prevention training from accrediting bodies are broad, leaving substantial flexibility to medical schools and residency programs in designing their objectives. For example, the word “suicide” is found neither in the Accreditation Council for Graduate Medical Education Program Requirements for Graduate Medical Education in Family Medicine nor in Internal Medicine [10, 11]. The same is true for the Liaison Committee on Medical Education guidelines, which emphasize the faculty of medical schools to define their own learning objectives, required clinical experiences, and competencies [12], providing opportunities for medical schools to customize such training for their learners. Some professional organizations, such as the Society of Teachers of Family Medicine, have a recommended clerkship curriculum that includes suicide risk assessment [13]; however, from our conversations with medical educators in this field, there is much room for improvement in depression and suicide prevention training in many programs. Indeed, previous work has highlighted the need for improved suicide prevention curricula in undergraduate medical education [14]. While teaching about suicide prevention is a necessary step, it alone is insufficient: examining medical students’ attitudes toward suicide and working to improve these attitudes is a critical component of training to promote compassionate and competent care [15].
The present study sought to fill this gap by developing, implementing, and evaluating a curricular thread on suicide prevention for pre-clerkship medical students. This curriculum was conceptualized from Kern’s six-step approach for curriculum development [16] and spiral curriculum [17] frameworks. An interdisciplinary team was formed with members from the disciplines of psychiatry, family medicine, psychology, neuroscience, wellness, and student life. This team consulted key stakeholders including administrators, faculty members, and students. The team discussed a variety of possibilities ranging from utilizing external programs to creating our own curriculum, dedicating a day to the topic versus weaving the topic throughout a curriculum, placing the content in a “doctoring” course versus biomedical science course, and positioning the content early versus later in the pre-clerkship curriculum. After evaluating the options, the team agreed for the course directors to create a suicide prevention thread (Table 1) integrated into a behavioral health course, the penultimate biomedical science course before clerkships. This later portion of the pre-clerkship phase specifically was chosen to build upon the foundational clinical skills training during the pre-clerkship phase and to equip students with necessary knowledge and skills for suicide prevention before they begin seeing patients in the clerkship phase of their medical training.
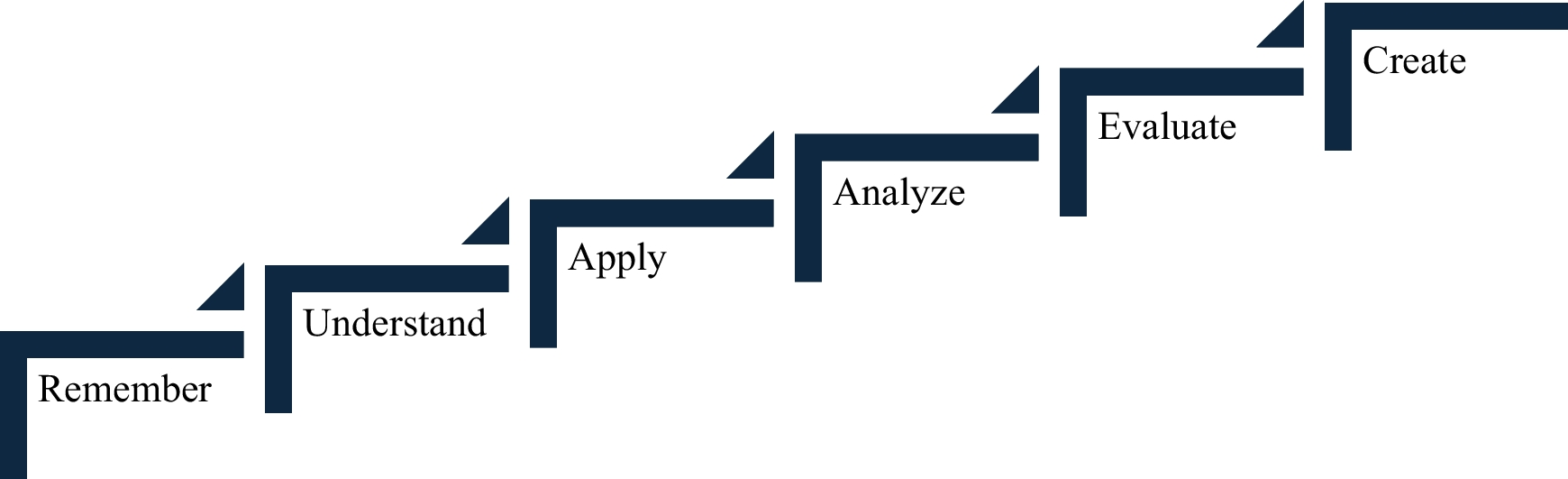
Table 1 Suicide prevention curricular thread. The curriculum included the following events weaved throughout a 4-week pre-clerkship behavioral health course. For additional information, readers are welcome to email the corresponding authorThe suicide prevention thread was designed through a spiral curriculum framework, whereby topics were revisited with increasing levels of difficulty so that new learning would build upon previous learning to increase students’ competence [17]. Earlier events focused on foundational knowledge and understanding (lower levels of Bloom’s taxonomy), whereas later events required case application, analysis, patient evaluation, and creation of a treatment plan (higher levels of Bloom’s taxonomy). The first event was an asynchronous guided independent learning module so that learners could complete it at their own pace and in the location of their choice; this was purposeful because the topics of depression and suicide can elicit strong emotions, especially in individuals with personal or family psychiatric histories. Building upon foundational mental health and suicide prevention training (delivered through the asynchronous guided independent learning module and lectures), students applied the concepts in case- and team-based learning events. The curricular thread culminated with learners combining their aforementioned training on depression and suicide prevention to interview and treat a standardized patient in the simulation center (Table 1). The goals of this curricular thread were to equip learners with clinically relevant knowledge, skills, and attitudes to increase their confidence identifying and treating patients at risk for suicide before beginning clerkships.



Comments (0)