
Remember me




A total of 44 participants were enrolled (31 women), mean age 47.27 ± (standard deviation) 12.94 years (Table 1). Participants were recruited from online advertisements (77.3%), primary care GP clinics (15.9%), and secondary care community mental health teams (6.8%). At baseline, mean MADRS and HAMD scores were 24.6 ± 2.64 and 20.0 ± 2.62, respectively. Mean duration of the current depressive episode was 0.95 ± 1.93 years (range 0.3 to 12 years). 97% of participants (n = 43) completed a minimum of 70% of sessions (15 tDCS sessions), mean 19.6 ± 1.9 sessions; 93.2% of participants (n = 41) completed the full 6-week course of treatment; and 72.7% of participants (n = 32) attended the 5-month follow up visit. 86.3% of participants (n = 38) were taking mood-stabilising medication, 2% of participants (n = 1) were taking antidepressant medication without mood-stabilising medication, 5 participants were not taking any pharmacological interventions, and 27.3% of participants (n = 12) were in psychotherapy (CBT or psychodynamic psychotherapy) in addition to taking medication.
In the follow up period, 24 participants continued using the tDCS device for some of the follow up period, and 16 participants continued to use the device at the 5-month visit.
Table 1 Demographic and clinical data at baselineClinical assessmentsFor all four time points (weeks 0, 2, 6 and 18), 73% of participants (n = 32) completed clinical questionnaires assessments at all time points and were included in the completers analysis. Data were missing from 27% of participants (n = 12) at the end of the follow up period (week 18).
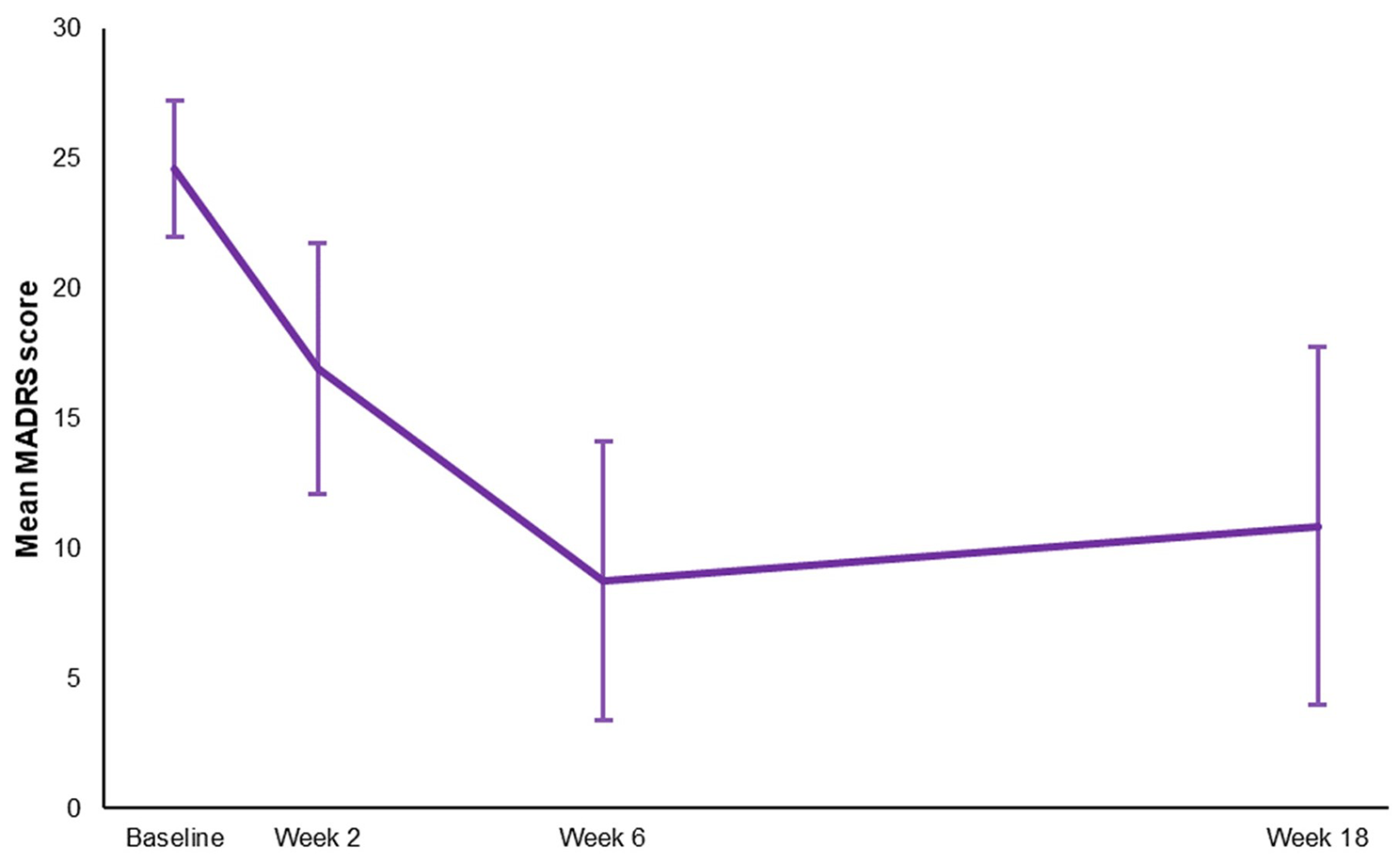
At week 6, mean MADRS score was 8.91 ± 5.56, in which 34 participants (77.3%) showed clinical response and 21 participants (47.7%) achieved clinical remission (Fig. 1). At week 2, following 10 tDCS sessions, seven participants (15.9%) showed an early response, one participant (2.3%) was in remission and mean MADRS score was 16.93 ± 4.82. At week 18, mean MADRS score was 10.86 ± 6.90, in which 20 out of 32 participants (62.5%) showed clinical response and 13 out of 32 participants (40.6%) achieved clinical remission. Repeated-measures analyses demonstrated significant clinical improvements in mean MADRS scores across time points in the ITT (F(2,88) = 120.51, p < 0.001) (Table 2) and completers (F(2,62) = 80.30, p < 0.001) analyses (Table 3). In the ITT analysis, post hoc tests revealed significant improvements between t(0), t(1), t(2), (p < 0.001) but no significant change between end of treatment week-6 (t(2)) and week-18 follow-up (t(3)) (p = 0.71) depressive symptom scores indicating that significant improvements were maintained at follow-up (Table 2). A similar pattern of results was evident in the completers analysis (Table 3).
Fig. 1
Mean Montgomery-Åsberg Depression Rating Scale (MADRS) scores from baseline to week-18 (intention-to-treat analysis). Error bars represent 1 standard deviation
Table 2 Clinical rating scale scores over the 6-week course of treatment and at the month 5 (18 week) follow up in the intension to treat analysisTable 3 Clinical rating scale scores over the 6-week course of treatment and at the month 5 (18 week) follow up in the completers analysisIn HDRS-17, there was a similar pattern of results. Mean HDRS-17 score was 6.77 ± 4.74 at week 6, in which 37 participants (84.1%) showed clinical response and 31 participants (70.5%) achieved clinical remission (Fig. 2). At week 2, 12 participants (27.3%) showed an early response, 3 participants (6.8%) were in remission and mean HDRS-17 score was 13.57 ± 4.14. At week 18, mean HDRS score was 8.59 ± 5.99, in which 19 out of 32 participants (59.4%) showed clinical response and 18 out of 32 participants (56.3%) achieved clinical remission. Significant clinical improvements in mean HDRS-17 scores were evident across time points in ITT (F(2,94) = 98.84, p < 0.001) and completers analyses (F(2,64) = 70.16, p < 0.001). In the ITT analysis, post hoc tests revealed significant improvements between t(0), t(1), t(2), (p < 0.001) but no significant change between end of treatment week-6 (t(2)) and week-18 follow-up (t(3)) (p = 0.76) depression scores, indicating that significant improvements were maintained at follow-up (Table 2). A similar pattern of results was evident for the completers analysis (Table 3).
Fig. 2
Mean Hamilton Depression Rating Scale (HDRS-17) scores from baseline to week-18 (intention-to-treat analysis). Error bars represent 1 standard deviation
In HAMA, YMRS, PHQ-9 and SDS scores, there were significant improvements from baseline, which were maintained from week 2 to week 6 (Tables 2 and 3). Mean HAMA score at baseline was 16.6 ± 5.26 (range 9–36), indicating mild to moderate severity of anxiety. Following treatment, the mean scores were 6.36 ± 4.10 at 6-weeks and 7.32 ± 4.85 at 18-weeks demonstrating mild anxiety (Fig. 3). Mean YMRS score at baseline was 2.20 ± 1.49 (range 0–7), indicating an overall absence of significant manic or hypomanic symptoms. Following treatment, the mean score decreased to 0.80 ± 1.09 at 6-weeks and 1.30 ± 1.37 at 18-weeks demonstrating a reduction from initial manic or hypomanic symptoms (Fig. 4). Mean PHQ-9 score at baseline was 16.8 ± 4.02, which improved following treatment (mean score at week 6 = 6.52 ± 4.69) and was maintained at follow up (mean score at week 18 = 8.34 ± 5.68) (Fig. 5). SDS rating of functional impairment was high at baseline (mean 20.77 ± 5.87) and significantly improved at the end of treatment (mean score at week 6 = 9.93 ± 7.85) and was maintained at follow up (mean score at week 18 = 11.16 ± 8.87) (Fig. 6).
Fig. 3
Mean Hamilton Anxiety Scale (HAMA) scores from baseline to week-18 (intention-to-treat analysis). Error bars represent 1 standard deviation
Fig. 4
Mean Young Mania Rating Scale (YMRS) scores from baseline to week-18 (intention-to-treat analysis). Error bars represent 1 standard deviation
Fig. 5
Mean Patient Health Questionnaire-9 (PHQ-9) scores from baseline to week-18 (intention-to-treat analysis). Error bars represent 1 standard deviation
Fig. 6
Mean Sheehan Disability Scale (SDS) scores from baseline to week-18 (intention-to-treat analysis). Error bars represent 1 standard deviation
Safety, acceptability, and tolerabilityThe most common side effects were tingling (83.5%), skin redness (40.6%), itching (29.3%) and burning sensation, (26.5%) (Table 4, supplementary material Table 1). 90.6% of adverse events related to tDCS were rated as mild, 9% were rated as moderate and 0.4% were rated as severe. These included one report each of tingling and burning sensation and two reports each of itching and skin redness.
Table 4 Total incidence of side effects out of 860 sessions during the 6-week treatment phase of the trialDuring the follow up period, common side effects were the same as during the trial (Supplementary Table 1). Two participants had experiences of dry skin and two participants who had continued to use the tDCS device reported experiencing hypomanic symptoms and had stopped using the device. Neither participant contacted the study team, and at the 5 month follow up visit hypomanic symptoms were not present for either participant, as indicated by YMRS assessment.
There was a significant increase in endorsement of acceptability as being “quite acceptable” at baseline and “very acceptable” post treatment and at follow up (t(0) Mdn = 6, IQR = 1; t(2) Mdn = 7, IQR = 0, t(3) Mdn = 7, IQR = 1) (X2F (2) = 15.7, p = < 0.001). Ratings for perceived effectiveness were endorsed as being “quite helpful” at baseline and post treatment, and “very helpful” at follow up with no significant change over time (t(0) Mdn = 6, IQR = 0.75; t(2) Mdn = 6, IQR = 1, t(3) Mdn = 7, IQR = 1) (X2F (2) = 4.17, p = < 0.13). Ethicality remained high at “very ethical” for all three time points, with no significant changes over time (t(0) Mdn = 7, IQR = 1; t(2) Mdn = 7, IQR = 0, t(3) Mdn = 7, IQR = 0) (X2F (2) = 4.2, p = < 0.12). The impact of side-effects showed a significant decrease from being “a bit unaffected/quite unaffected” at baseline to being “very much unaffected” post-treatment and “very much unaffected/quite unaffected” at follow up (t(0) Mdn = 2.5, IQR = 2.75; t(2) Mdn = 1, IQR = 1, t(3) Mdn = 1.5, IQR = 3.25) (X2F (2) = 15.7, p = < 0.001). There was also a significant decrease in the perceived amount of effort required which improved from “some more effort than usual” at baseline to “a little bit more effort than usual” post treatment and “a little bit less effort than usual” at follow up (t(0) Mdn = 2, IQR = 1; t(2) Mdn = 3, IQR = 3, t(3) Mdn = 5, IQR = 3.75) (X2F (2) = 33.9, p = < 0.001). At post treatment and at follow up participants “would very strongly recommend” tDCS to others with no significant differences over time (t(2) Mdn = 7, IQR = 1, t(3) Mdn = 7, IQR = 1) (Z = -0.52, p = 0.61) (Fig. 7).
Fig. 7
Percentage of participants who endorsed each response in the acceptability questionnaire at baseline (n = 44), end of treatment (n = 41) and follow up (n = 32)
Comments (0)