Numerous studies haves identified correlations between ARHE/SCAF and stroke or systemic embolism [12, 14,15,16,17,18, 28]. However, the degree of correlation varies between studies and definitions differ. Table 1 summarises the details of key studies of ARHE/SCAF and systemic embolism, including which definition of AHRE/SCAF was applied.
Table 1 Key studies in AHRE/SCAF and thromboembolic risk, excluding those conducted solely in patients with preexisting atrial fibrillationMultiple meta-analyses including the studies in Table 1 have associated the presence of AHRE/SCAF with increased thromboembolic risk. The presence of AHRE confers a two-to-three fold increased risk of thromboembolic events [29, 30]. This increased risk has been found to persist after adjustment for CHA2DS2-VASc score [17]. Belkin et al. [30]. also found thromboembolic risk to be higher in patients with adjudicated atrial electrograms (RR 3.60; 95% CI: 2.06–6.30; P < 0.001) when compared with non-adjudicated device detected atrial tachyarrhythmia (RR 2.05; 95% CI: 1.06–3.97; P = 0.03). This variation highlights the clinical significance of differing AHRE and SCAF definitions and the need for consensus if we are to adequately address these risks.
Additional observational studies have sought to establish a burden-dependent relationship between device detected atrial tachyarrhythmia and thromboembolic risk. The TRENDS study demonstrated that increased burden of device detected AF is associated with higher ischaemic stroke risk in a cohort of patients with and without a history of paroxysmal AF at enrolment [13]. This analysis included patients both receiving and not receiving anticoagulation. After adjusting for stroke risk factors and anticoagulation use, the risk of ischaemic stroke, transient ischaemic attack (TIA), or systemic embolism in patients with less than 5.5 h of device detected atrial arrhythmia per day (defined as time spent in mode switch triggered by an atrial rate > 175 bpm lasting ≥ 20 s) was similar to that of patients with zero daily atrial tachycardia/AF burden (1.1% annual incidence in both groups; HR 0.98; 95% CI: 0.34 to 2.82; P = 0.97). Conversely, the annual incidence in patients with > 5.5 h of device detected atrial arrhythmia was higher at 2.4% (HR compared with the zero AT/AF burden group: 2.20; 95% CI: 0.96 to 5.05; P = 0.06). This may suggest that thromboembolic risk is significantly higher in patients with greater device detected atrial arrhythmia burdens – however, 5.5 h was arbitrarily chosen as the median burden in this particular study and may therefore not be reflective of all patients. It should be noted that confidence intervals were wide and some p-values were borderline in this study, but this analysis raises questions regarding the benefit of anticoagulation in patients with low daily burdens of device detected atrial tachyarrhythmias.
A 2014 meta-analysis of 10,016 patients included in observational studies, including TRENDS, further characterised thromboembolic risk in patients with device detected atrial tachyarrhythmias with specific regard to the total daily burden [31]. As with TRENDS, this meta-analysis included patients with and without history of AF, and both receiving and not receiving anticoagulation. After adjusting for CHADS2 score and anticoagulation use, Boriani et al. found statistically significant increases in the risk of ischaemic stroke or TIA in patients with ≥ 5 min of daily device detected atrial tachyarrhythmia burden (defined as the maximum time spent in atrial tachyarrhythmia over a single day during follow up) when compared with < 5 min daily burden (HR 1.76; 95% CI: 1.02–3.02; P = 0.041), and for patients with ≥ 1 h of daily device detected atrial tachyarrhythmia when compared with < 1 h (HR 2.11; 95% CI: 1.22–3.64; P = 0.008). Of note statistical significance was not achieved performing the same analysis when stratifying patients based upon daily burden thresholds of 6 h, 12 h, or 23 h. This may suggest a daily AF burden of just 5 min increases thromboembolic risk, although statistical significance at this threshold was borderline (p = 0.041). The 1 h threshold was more convincingly positive, with an estimated two-fold increase in risk.
Analysis of AHRE/SCAF episode duration, rather than total burden, has drawn slightly differing conclusions concerning the amount of arrhythmia deemed to increase thromboembolic risk. The ASSERT trial (Asymptomatic atrial fibrillation and Stroke Evaluation in pacemaker patients and the atrial fibrillation Reduction atrial pacing Trial) included 2,580 patients with implanted cardiac devices and no prior history of AF, and investigated the relationship between the duration of SCAF episodes and ischaemic stroke or systemic embolism [15]. Patients with an episode lasting > 24 h were found to have a significantly increased risk of stroke or systemic thromboembolism when compared with patients with no SCAF (HR 3.86, 95% CI: 1.91–7.78; P ≤ 0.001) [32]. This finding persisted after adjustment for age, sex, cardiovascular disease and prior stroke/TIA (HR 3.24, 95% CI: 1.51–6.95; P = 0.003).
In contrast to the aforementioned meta-analysis conducted by Boriani et al. [31]. , ASSERT found no significant increase in the risk of ischaemic stroke or systemic thromboembolism in patients with SCAF episodes lasting between 6 min and 24 h when compared with patients with zero episodes. This finding persisted when including patients with subclinical AF lasting ≤ 6 min in the zero SCAF group. Although direct comparison is not possible as ASSERT measured SCAF duration whereas TRENDS and others assessed total daily burden, these results still prove discordant. On one hand ASSERT found no increased thromboembolic risk for SCAF episodes lasting less than 24 h, yet Boriani et al. found a daily burden of just 5 min to represent a significant thromboembolic risk. It is also important to note the differing populations between these trials; the meta-analysis by Boriani et al. included patients with and without known AF and had no minimum stroke risk profile for inclusion (although stroke risk was adjusted for in analysis), whereas ASSERT did not include patients with known AF and used inclusion criteria of hypertension and age of ≥ 65 years, equating to a minimum CHA2DS2-VASc score of 2 for males and 3 for females.
The RATE Registry trial provided additional study of the association between AHRE/SCAF duration and thromboembolic risk, with a focus on shorter episodes [18]. In a study of 5,379 patients with a permanent pacemaker (PPM) or implantable cardioverter defibrillator (ICD) with no documented AF in 3 months prior to enrolment, Swiryn et al. defined atrial tachycardia/atrial fibrillation (AT/AF) as ≥ 3 consecutive premature atrial contractions, short AT/AF as an episode with onset and termination in the same device electrogram recording (typically < 15–20 s), and long AT/AF as an episode without both onset and termination within the same device electrogram recording. A random sample of 600 patients (300 with PPMs, 300 with ICDs) had their electrograms adjudicated by a physician and device clinical engineer, in addition to all patients with an AF-related adverse event (AF hospitalisation, heart failure hospitalisation, stroke/TIA, syncope, VT hospitalisation, and all-cause death). No statistically significant association was found between long or short AT/AF episodes and stroke in univariate or multivariate analysis adjusting for cardiovascular history and anticoagulant use in either PPM or ICD groups. This is more in keeping with the findings of ASSERT, in that using a low threshold in AHRE/SCAF episode duration did not associate with a statistically significant increase in thromboembolic risk.
Taken altogether, a positive correlation between AHRE/SCAF burden and thromboembolic risk exists for some level of arrhythmia burden and/or episode duration, however the differing results of observational studies and the non-uniform nature of AHRE/SCAF definitions implies that further, more standardised research is required. It is important to note that this does not necessarily imply causality, as increased AHRE/SCAF burden may be a surrogate for various diseases, lifestyle factors, or inflammation that can also contribute to increased thromboembolic risk [33].
An important consideration when determining stroke risk associated with AHRE/SCAF is the presence of other thromboembolic risk factors. In a study of 343 patients, including patients with paroxysmal AF but omitting those with persistent AF, Kawakami et al. found AHRE to be associated with ischaemic stroke or systemic embolism only in patients with a CHADS2 score of > 2 (HR 3.73; 95% CI: 1.06–13.1; P = 0.04), and no association between AHRE and stroke/systemic embolism in patients with CHADS2 score of 0–2 [34]. Though not limited to patients without clinical AF, this strengthens the suggestion that thromboembolic risk in AHRE/SCAF is a product of device detected arrhythmia in the context of an already raised thromboembolic risk profile. However, in a study of 594 patients limited to those without prior AF, Li et al. found that CHA2DS2-VASc score was independently associated with thromboembolic events, but that the presence of AHRE was not associated with higher thromboembolism rates in populations with low (< 2 for males, < 3 for females) or high (≥ 2 for males, ≥ 3 for females) CHA2DS2-VASc score [21].
Neither study stratified patients by AHRE burden or duration. Considering the findings of studies on AHRE/SCAF burden/duration and thromboembolic risk, subgroup analysis of patients grouped by both arrhythmia burden/duration and CHA2DS2-VASc score may provide valuable insights into the group(s) most at risk. To complexify matters further, studies have shown that thromboembolic events do not always temporally associate with arrhythmia episodes [35,36,37]. This suggests that higher arrhythmia burden may not itself be the cause of thromboembolism, but instead a marker of elevated risk.
Anticoagulation in AHRE/SCAF
Two large randomised controlled trials of anticoagulation in AHRE/SCAF were recently published. The ARTESiA trial was a double blind randomised controlled trial including 4,012 patients with SCAF randomised to receive apixaban or aspirin. The investigators found a significant reduction in stroke or systemic embolism in the apixaban arm (0.78% vs. 1.24% per patient year; HR 0.63; 95% CI 0.45–0.88; P = 0.007), but a higher risk of major bleeding (1.71% vs. 0.94% per patient year (HR 1.80; 95% CI 1.26–2.57; P = 0.001) [27].
The NOAH-AFNET 6 trial was also a double blind randomised controlled trial of 2,536 patients with AHRE randomised to receive edoxaban or placebo, but was terminated early at a median follow-up of 21 months for futility of edoxaban in preventing a combined endpoint of cardiovascular death, stroke or systemic embolism, in combination with an increase in safety events (all cause death or major bleeding) in the edoxaban arm (5.9% vs. 4.5% per patient year; HR 1.31; 95% CI 1.02–1.67; P = 0.03) [26]. At termination, systemic embolism events were less frequent with edoxaban (0.5% vs. 1.1% per patient year; HR 0.51; 95% CI: 0.27–0.96; p = ns), however stroke incidence was similar between edoxaban and placebo (0.9% vs. 1.1% per patient year respectively; HR 0.79; 95% CI: 0.45–1.39). This may be due to underpowering related to early termination [38].
It was also noted in both trials and meta-analyses that the ischaemic stroke risk in the untreated arms was less than expected [26, 27, 39] when compared with ischaemic stroke rates in prior trials such as ELDERCARE-AF [40] or AVERROES [41]. Various reasons have been suggested for this, including relatively low arrythmia burden and improved treatment of concomitant cardiovascular diseases [26, 39]. It is unlikely that the absence of symptoms in SCAF/AHRE is a factor, as meta-analysis has found no difference in mortality, cardiovascular death, or thromboembolism between symptomatic and asymptomatic clinical AF [42]. Regardless of cause, a key message is that AHRE/SCAF has a distinct, lower risk profile for ischaemic stroke when compared with clinical AF, and the decision to anticoagulate is not straightforward.
The differing findings of ARTESiA and NOAH-AFNET 6 in relation to stroke risk reduction prompts detailed comparison of the two trials. There are key differences between the two, particularly in terms of arrhythmia definition, inclusion criteria, control group treatment, and primary outcome measure. These are discussed below and summarised in Table 2.
Table 2 Key differences between the ARTESiA and NOAH-AFNET 6 trialsA Comparison of ARTESiA and NOAH-AFNET 6
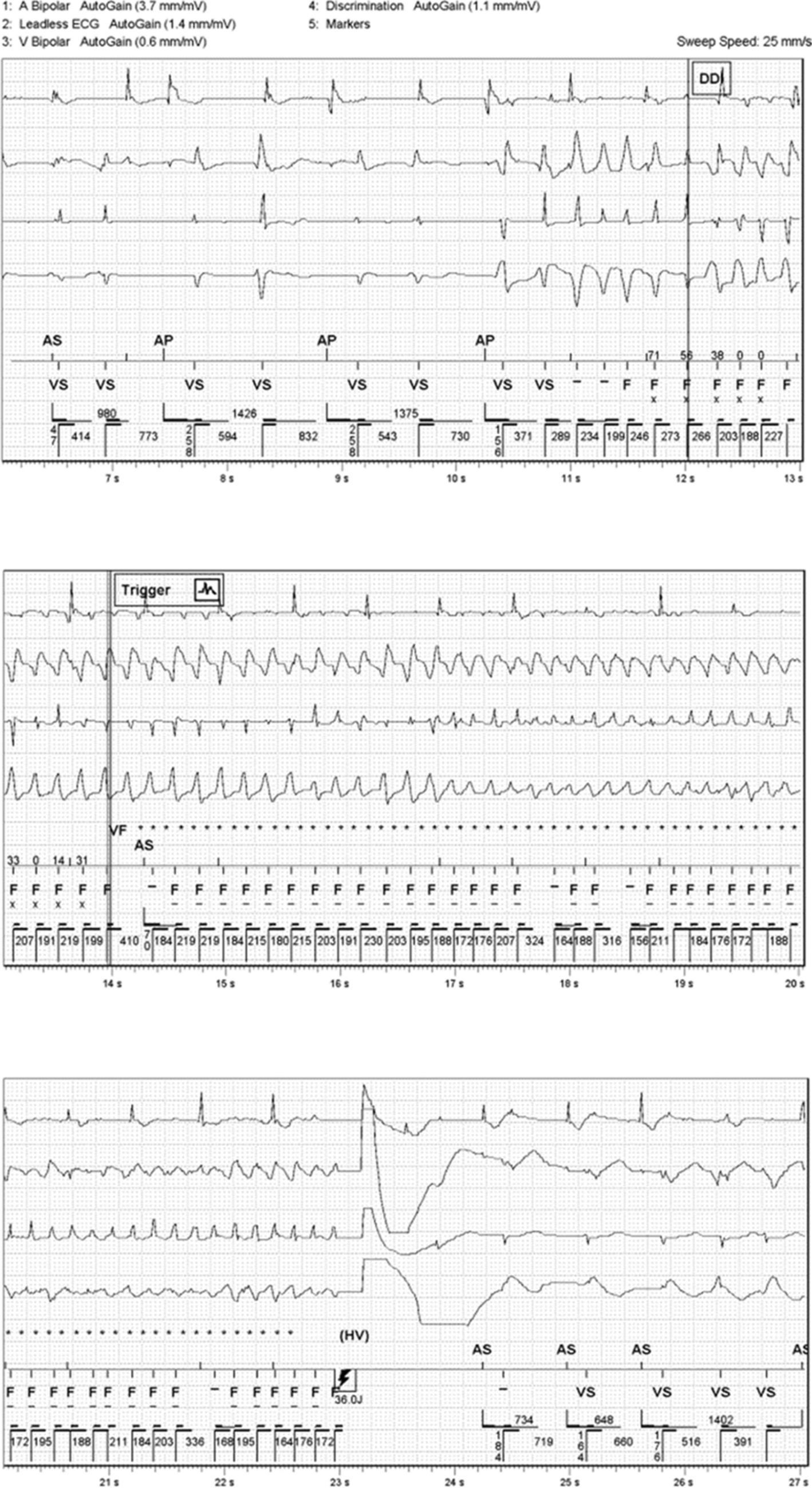
The criteria for device detected arrhythmia differed between ARTESiA and NOAH-AFNET 6 in both arrhythmia definition (AHRE vs. SCAF) and length. ARTESiA included patients with SCAF, which must be confirmed with electrogram review unless ≥ 6 h in duration, and included patients with SCAF episodes ≥ 6 min in duration but excluded patients with a single episode > 24 h in duration at any time prior to enrolment [39]. In contrast, NOAH-AFNET 6 used AHRE rather than SCAF (the distinction between these entities is illustrated in Fig. 1) – specifically with an atrial rate of ≥ 170 beats per minute and ≥ 6 min duration as inclusion criteria, with no upper bound for AHRE duration (Fig. 2).
Both the arrhythmia definition and duration are important when interpreting the differing results of ARTESiA and NOAH-AFNET 6. With regard to arrythmia definition, it should be noted that using SCAF as inclusion criteria may lead to a higher baseline risk when compared with AHRE, as AHRE not confirmed by electrogram review may include supraventricular arrhythmias not associated with thromboembolic risk. When considering arrhythmia duration, the exclusion of patients in the ARTESiA trial with episodes > 24 h in length is significant as some studies, such as the ASSERT trial, have identified this group as being at the highest risk [15]. However, as previously discussed, the significance of episodes less than 24 h in duration differs in various trials [14, 15, 17].
Baseline thromboembolic risk also differed between the two trials. NOAH-AFNET 6 used age ≥ 65 years with modified CHA2DS2-VASc score ≥ 2 [26], whereas ARTESiA used inclusion criteria amounting to CHA2DS2-VASc score ≥ 2 in one category, or aged ≥ 55 years with CHA2DS2-VASc score ≥ 3 [27].
Control group treatments also differed. The control arm of ARTESiA received aspirin 81 mg once daily, whereas NOAH-AFNET 6 utilised either aspirin 100 mg once daily or placebo, based on the presence or absence of a recognised indication for aspirin. This resulted in 54% of control patients in NOAH-AFNET 6 receiving aspirin. Concerns over dampening of relative bleeding risk in ARTESiA have been noted for this reason, with the inherent bleeding risk of antiplatelet therapy mandated for the control group leading to an underestimation of relative bleeding risk with oral anticoagulant use in patients who would otherwise receive no anticoagulants or antiplatelets [38].
Finally, outcomes measures differed between the two trials. ARTESiA had a primary outcome of ischaemic stroke or systemic embolism [27], whereas NOAH-AFNET 6 used a composite of cardiovascular death, stroke, or systemic embolism [26]. However, NOAH-AFNET 6 did report ischaemic stroke and systemic embolism as a secondary outcome, thus facilitating comparison with ARTESiA.
Despite these differences, a meta-analysis of ARTESiA and NOAH-AFNET 6 reported a significant reduction in ischaemic stroke with oral anticoagulation (RR 0.68, 95% CI 0.50–0.92) with minimal heterogeneity (I2 = 0%) [39].
The fact that ARTESiA found benefit of anticoagulation whilst excluding the group (by arrhythmia duration) that some studies have deemed at highest risk, whereas NOAH-AFNET 6 found no benefit despite including patients with longer duration AHRE, suggests that other factors may outweigh the correlation between AHRE/SCAF duration and embolic risk. In particular, the differing baseline thromboembolic risk profiles of the two populations and differing arrhythmia definition (SCAF in ARTESiA versus AHRE in NOAH-AFNET 6) may have influenced results. It is also possible that apixaban is superior to edoxaban for prevention of thromboembolism, as suggested by some studies [43], although a head-to-head trial is needed to confirm this.
At present ESC guidelines recommend a combination of arrythmia duration/burden and underlying thromboembolic risk profile is used when considering anticoagulation in the AHRE/SCAF population, which falls in line with the results of ARTESiA and NOAH-AFNET 6, in addition to aforementioned studies on stroke risk in this population [12, 14,15,16,17,18, 28]. Further studies grouping patients by both thromboembolic risk and arrythmia burden/duration are required to more accurately risk stratify these patients, and thus lead to better informed decision-making around anticoagulation.
Regarding major bleeding, the magnitude of risk observed in both ARTESiA and NOAH-AFNET 6 trials is consistent with previous trials of DOAC therapy in patients with AF [40, 41, 44, 45], suggesting that, while the ischaemic stroke risk profile of AHRE/SCAF may be distinct from that of clinical AF, the risk of anticoagulation-related bleeding with apixaban or edoxaban is not.
Preventing Progression to Clinical Atrial Fibrillation
AHRE/SCAF has been observed to confer a significant risk of progression to clinical AF [15, 17, 29], with hazard ratios varying from 2.35 over a median follow up of 4.6 years [17] to 5.56 over a median follow up of 2.5 years [15]. Despite the well-established practice of using antiarrhythmics to maintain sinus rhythm in patients with clinical AF [46], and the fact that rhythm control may delay progression of clinical AF [47,48,49], there has been no research performed to assess the role of antiarrhythmic therapy in preventing progression of AHRE/SCAF to clinical AF. However, the current literature on antiarrhythmic use in patients with clinical AF suggests that a similar strategy is unlikely to confer overall benefit if used in the AHRE/SCAF populations. In patients with clinical AF, comparisons of rate versus rhythm control strategies have largely shown no benefit to rhythm control in reducing mortality or stroke [50,51,52,53,54], and have also raised concerns regarding the recognised risk of serious adverse events and increased hospitalisation with rhythm control [50, 51, 55,56,


Comments (0)