
Remember me







Fibrotic posterior capsular opacification (PCO) is one of the major complications that impairs capsular transparency after cataract surgery with intraocular lens (IOL) implantation.1,2 Lens epithelial cells (LECs) are activated by an injury associated with phacoemulsification–IOL implantation surgery and transform their phenotype to myofibroblast, the major cellular component involved in capsular fibrosis. This process is called epithelial–mesenchymal transition.3 Besides the original extracellular matrix (ECM) components of lens capsule, for example, collagen type IV, laminin, and proteoglycan types, and LEC-derived myofibroblasts accumulate collagen types I and III, fibronectin, and other wound healing reaction-related ECM components. On the other hand, we routinely recognize that fibrotic tissue embeds and fixes the IOL haptics and the peripheral optic part of an IOL in the capsular bag.4
In the early 2000s, cases of dislocation of an IOL implanted in the capsular bag associated with a diaphanous and floppy capsular bag have been reported.5 The major finding in these cases included a floppy, transparent lens capsule in association with fewer fibrotic components. The dislocation of an IOL in these cases does not seem to be caused by an impairment of zonular fibers, such as in cases with pseudoexfoliation where zonular weakness is primarily observed.6,7 The pathology is observed in the later postoperative period postcataract surgery. Samuel Masket coined the term “dead bag syndrome (DBS).” An initial peer-reviewed report on this syndrome included 10 cases in which 7 patients received extraction of the complex capsular bag/IOL.5 Standard histological analysis of these extracted capsules was performed by using hematoxylin and eosin (HE) staining. The findings obtained by the examination on HE-stained samples indicated that the IOL was not well stabilized in the capsular bag that lacked fibrosis or regenerated lenticular structure of Soemmerring's ring. Splitting/delamination of the capsule was also seen in samples.5 However, HE staining histology has a limitation in analysis of ECM composition of the affected capsule. Performance of immunohistochemical analysis of diseased capsular bags from DBS cases may provide further insights into the pathological mechanism of this syndrome. Immunohistochemistry specifically visualizes distributions and amounts of certain molecules in the tissue, which may be involved in the pathogenesis, diagnosis, and treatment of diseases, using the specific antigen–antibody reaction. This technique is performed without destruction of histologic architecture, and thus, the assessment of the expression pattern of the molecules is possible in the context of microenvironment.8
This study represents an attempt to provide further information on the pathobiology of DBS. Therefore, we performed light microscopic immunohistochemistry in specimens previously analyzed by using HE staining as reported by Culp et al., as well as other DBS specimens received after publication of that study.5 The results indicated that the capsule of DBS is almost free from fibrous ECM and cellular debris.
METHODSA total of 9 capsular bag specimens from DBS cases obtained from 7 male and 2 female patients were included (Table 1). Six of the 9 samples had also been included in the first peer-reviewed report on the DBS, which only described findings of HE staining.5 The other 3 samples were received for analyses after publication of the above-mentioned article. The mean age of patients at explantation was 65 years (range, 56 to 72 years). Time between implantation and explantation was 9.25 ± 4.79 years. IOL types in each sample were 7 one-piece hydrophobic acrylic and 2 three-piece silicone. The samples of IOLs/capsular bags included in this study were explanted in 3 different locations by 4 different surgeons: Drs. Jason Jones (Sioux City, IA), Nicole Fram (Los Angeles, CA), Gregory Ogawa (Albuquerque, NM), and Sam Masket (Los Angeles, CA). Detailed information regarding the original IOL implantation procedure in each case (including performance of capsular polishing) is not available because the explanting surgeons did not perform the implantations; however, the procedures were described as uneventful.
Table 1. - Characteristics of the dead bag syndrome cases included in this study Casea 1 2 3 4 5 6 7 8 9 Patient age at explantation 72 70 66 62 56 60 71 66 66 Sex M F M M M F M M M Race/ethnicity Non-Hispanic White Non-Hispanic White Non-Hispanic White Non-Hispanic White Asian Non-Hispanic White Non-Hispanic White Asian Non-Hispanic White Eye Left eye Right eye Left eye Left eye Left eye Left eye Right eye Right eye Left eye IOL manufacturer and type Abbott Medical Optics (AMO) SI30 3-piece silicone lens with Prolene haptics Johnson & Johnson (J&J) TECNIS 1-piece with haptics hydrophobic acrylic lens AMO SI30 3-piece silicone lens with Prolene haptics J&J TECNIS 1-piece with haptics hydrophobic acrylic lens J&J TECNIS 1-piece with haptics hydrophobic acrylic lens Alcon AcrySof (SN60WF) 1-piece with haptics hydrophobic acrylic lens Alcon AcrySof (SN60WF) 1-piece with haptics hydrophobic acrylic lens Alcon AcrySof (SN60WF) 1-piece with haptics hydrophobic acrylic lens Alcon AcrySof (SN60WF) 1-piece with haptics hydrophobic acrylic lens Length of implantation (y) 13.75 7.8 16.5 4 3.7 8 b b 11 Explantation reason In-the-bag IOL dislocation Inferior in-the-bag IOL subluxation, and then in-the-bag IOL dislocation into the anterior chamber Subluxation of IOL In-the-bag IOL dislocation In-the-bag IOL dislocation, 3 mo after Nd:YAG laser posterior capsulotomy Nasal subluxation of IOL still in the bag through peripheral capsular defect. One haptic still in the bag; focal area of fibrosis in relation to its tip; remaining of the capsular bag was very clear. The other haptic and part of optic was out of the bag through peripheral defect In-the-bag IOL dislocation In-the-bag IOL dislocation Superior subluxation of IOLaThe hematoxylin and eosin findings of cases 1 to 6 were described in Culp C, Qu P, Jones J, Fram N, Ogawa G, Masket S, Mamalis N, Werner L. Clinical and histopathological findings in the dead bag syndrome. J Cataract Refract Surg 2022;48:177–184
bLength of implantation reported as “many years”
Two other capsular bag specimens were included as a control group. The first was from a 62-year-old man, who underwent phacoemulsification with IOL implantation in the left eye (3-piece hydrophobic acrylic lens, model X-70, manufactured by Santen GmbH) in 2015. The patient had a history of vitrectomy and scleral buckling for retinal detachment in the same eye. In-the-bag IOL dislocation then occurred in 2023, and the IOL/capsular bag complex was explanted. The second was from an 83-year-old woman, who underwent phacoemulsification with IOL implantation in the left eye (1-piece hydrophobic acrylic lens, model AF-1 NY-60, manufactured by Hoya Corp.) in 2012, and removal of the IOL/capsular bag complex in 2021 due to in-the-bag IOL dislocation after blunt trauma to the eye. The patient had a history of pseudoexfoliation. Both control cases were from the Department of Ophthalmology of the Wakayama Medical University School of Medicine; the patients were both Asian and were managed with scleral fixation of a new IOL. Explantation procedures were performed as part of standard of care; histopathological examination of the explanted IOL/capsular bag complexes received institutional review board approval.
Routine immunohistochemistry was performed according to our previous publication.9 In brief, after paraffin embedding, 2 slides containing 2 unstained sections each were obtained from the capsular bags. Each section was treated with a primary antibody that reacted with the target protein. After washing with phosphate buffered saline, the section reacted with a peroxidase-conjugated secondary antibody that reacted with the primary antibody, followed by another phosphate buffered saline wash. The brown color of the antibody complex was developed by treatment with diaminobenzidine solution containing hydrogen peroxide. Details of the primary antibodies used are summarized in Table 2.
Table 2. - Primary antibodies used for immunohistochemistry Antibody type Company Dilution ratio Anti-type IV collagen antibody (#1340-01) Southern Biotech, Birmingham, AL 1:200 Anti-laminin antibody (#L9393) Sigma-Aldrich, St. Louis, MO 1:25 Anti-vimentin antibody (C-20) (#sc-7557) Santa Cruz Biotechnology, Dallas, TX 1:100 Anti-type I collagen antibody (#1310-01) Southern Biotech, Birmingham, AL 1:200 Anti-fibronectin antibody (C-20) (#sc-6952) Santa Cruz Biotechnology, Dallas, TX 1:50In the DBS group, the capsular specimens showed a general lack of LECs, as well as fibrous tissue and proliferative/regenerative material (Soemmerring's ring) (Figure 1). We initially attempted to immunohistochemically detect collagen type IV and laminin, the original components of basement membrane, that is, lens capsule. The outer thinner part of the anterior capsule, separated from the thick inner part, exhibited more marked collagen type IV staining. The thinner posterior capsules also had areas that were type IV collagen positive.
 Figure 1.:
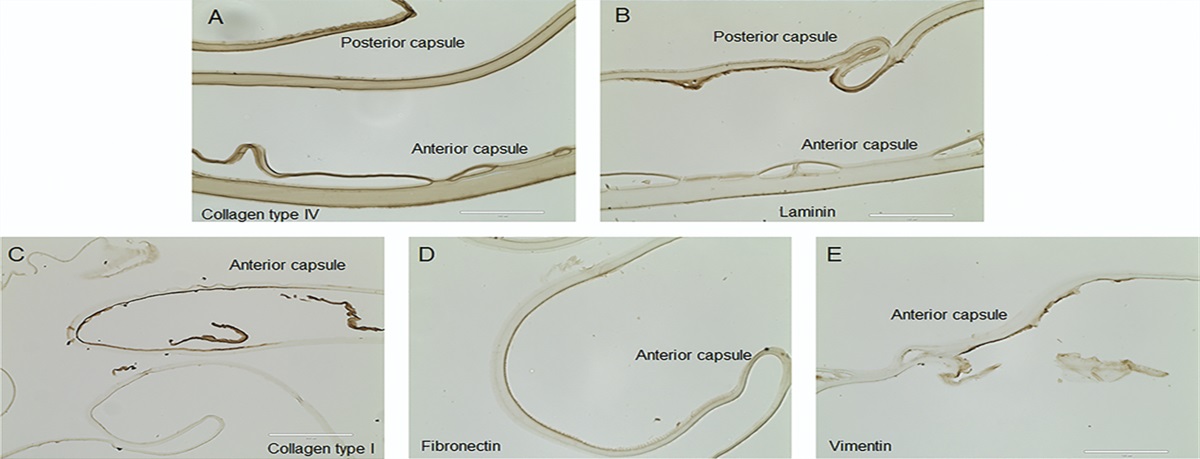
Figure 1.: Immunohistochemistry in dead bag syndrome. A: Collagen type IV and laminin, the original components of lens capsule are readily detected in capsular tissue. The outer thinner part of the anterior capsule, separated from the thick inner part, exhibited more marked collagen type IV staining. The thinner capsule is the posterior capsule with areas also type IV collagen positive (case 1). B: Staining pattern for laminin is similar to that seen in collagen type IV staining (case 1). C and D: Collagen type I and fibronectin are present, both of which are extracellular matrix components of fibrotic posterior capsular opacification. Both components are detected in small, restricted areas of sections devoid of lens epithelial cells in 2 samples. This suggests that lens epithelial cells were present, secreted collagen type I and fibronectin, and then died/detached (case 3). E: Vimentin is one of the original lens epithelial cell cytoskeletal components. Small positive staining without a cell body is detected in limited areas of sections from 2 samples. The finding indicates there were very limited amounts of cellular components present (presumably cell debris) (case 9). Bar: 100 µm.
We then checked for the presence or absence of collagen type I and fibronectin, both of which are ECM components of fibrotic PCO. Both components were detected in small, restricted areas of sections devoid of LECs in 2 samples. This suggests that LECs were present, secreted collagen type I and fibronectin, and then died/detached.
Finally, we immunostained sections with anti-vimentin antibody. Vimentin is one of the original LEC cytoskeletal components, and therefore, its immunoreaction indicates the presence of LECs or dead cell debris of LECs. Small positive staining without cell bodies was detected in limited areas of sections from 2 samples. The finding indicates there were very limited amounts of cellular components present on the capsule (presumably cell debris).
In the control group, the specimen from case 1 showed fibrous tissue, particularly around the capsulotomy edge and on the inner surface of the anterior capsule. LECs were observed on the inner surface of anterior and posterior capsules. Therefore, there was abundant detection of collagen type I, fibronectin, and vimentin in this specimen (Figure 2). The specimen from case 2 showed significant Soemmerring's ring formation. There was abundant fibrous tissue formation around the edge of the capsulotomy, as well as on the inner surface of anterior and posterior capsules and within the Soemmerring's ring, with LECs intermixed within the fibrous tissue. The inner surface of both capsules stained positive for collagen types IV and I. Fibronectin and vimentin were also both observed in the fibrous tissue on the inner surface of both capsules (Figure 3).
 Figure 2.:
Figure 2.: Immunohistochemistry in control case 1. A and B: Hematoxylin and eosin staining shows fibrous tissue formed around the edge of the anterior capsulotomy (A), but not on the inner surface of the posterior capsule (B). C and D: Collagen type IV was detected in capsular tissue in the anterior (C) and posterior (D) capsules. Staining pattern for laminin was similar to that seen in collagen type IV staining (not shown). E and F: Collagen type I was detected in the fibrous tissue on the inner surface of the anterior capsule (E), but not on the posterior capsule (F). Fibronectin (G and H) and vimentin (I and J) were observed in the fibrous tissue (G) and in the cells (I) on the inner surface of the anterior capsule, as well as on the posterior capsule inner surface (H and J). Bar: 100 µm.
 Figure 3.:
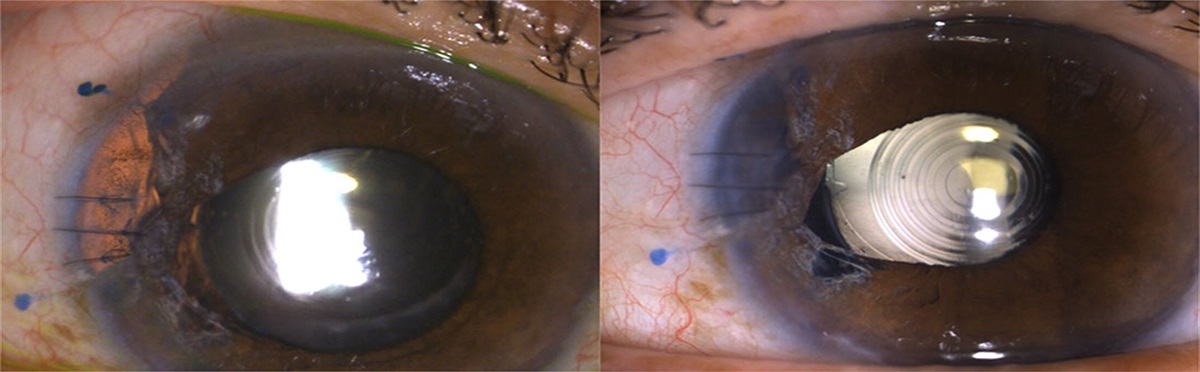
Figure 3.: Immunohistochemistry in control case 2. A: Gross photograph of the in-the-bag dislocated IOL showing that the peripheral area of the capsular bag is occupied by regenerated lens structure (Soemmerring's ring). B: Hematoxylin and eosin staining shows fibrous tissue formed around the edge of the anterior capsulotomy and lens fibers in Soemmerring's ring. The fibrous tissue on the inner surface of the anterior capsule (C, E) and posterior capsule (D, F) stained collagen types IV (C, D) and I (E, F). Fibronectin is very faintly observed in the fibrous tissue on the inner surface of the anterior capsule (G) and on the posterior capsule inner surface (H). Vimentin (I, J) was observed both in the fibrous tissue on the inner surface of the anterior capsule (I) and on the posterior capsule inner surface (J). Bar: 100 µm.
DISCUSSIONThe exact etiology of DBS is as of yet unknown, but we hypothesize that the potential mechanisms of the late postoperative zonular failure observed in this disease relate to capsule splitting/delamination occurring at the level of zonular attachments.5 In a previous study on DBS, the main feature of histopathology was capsular splitting or delamination.5 LECs were rarely seen or were completely absent from the inner surface of the capsule. Only 1 capsular bag specimen had mild amounts of anterior fibrous metaplasia, and another capsular bag contained a small amount of cortical material on microscopic examination. The above-mentioned findings were compared with those of capsules from 40 control cases of in-the-bag IOL dislocation, including 26 cases with evident pseudoexfoliation material.7 LECs and Soemmerring's ring formation were observed in all 40 cases; capsulorhexis phimosis was also a relatively common finding, while capsular splitting/delamination was only found in 1 control specimen.
In the present immunohistochemical study, the 2 control capsular bags included also had abundant fibrocellular tissue attached to the inner surface of the capsule, as well as Soemmerring's ring formation (Figures 2 and 3). Collagen type I and fibronectin are related to wound healing processes, and therefore cumulated, as expected, within the fibrocellular tissue observed in these specimens. This tissue also shows vimentin, which is a cytoskeletal component of LECs. However, although the majority of DBS capsule samples were devoid of LECs and fibrous tissue, positive staining for collagen type I, fibronectin, and vimentin was observed in these areas, suggesting that LECs were present after surgery, secreted components of fibrotic posterior capsule opacification (collagen type I and fibronectin), and later died/detached. The samples included are likely representative of the severe end of the spectrum of DBS.
The first peer-reviewed report on this syndrome, which only included HE findings, suggested that the mechanisms of development of DBS include split of the capsule.5 Capsular splitting/delamination occurring at the level of the zonular attachments leads to in-the-bag IOL dislocation. The literature indicates there is also capsular splitting/delamination in true exfoliation syndrome. However, in this condition, which is generally associated with chronic exposure to intense heat or infrared radiation, there may be already a thin membrane of delaminated capsule on the anterior surface of the crystalline lens before cataract surgery.10 In the DBS, the capsule is not tightly shrink-wrapped around the IOL, which might allow the aqueous humor to continue the influx within the inner capsular bag compartment.11 The exact cause of the separation of the lens capsule into 2 layers remains to be investigated. However, more intense immunoreactivity for type IV collagen in the outer portion of the capsule, not observed in the control samples, might be related to the separation of the capsule (Figure 1).
Findings from this study suggest a minor number of LECs were present after surgery and secreted collagen type I and fibronectin before they underwent the cell death process. It has been reported that continuous exposure of LECs to aqueous humor accelerates cell death on the residual postcataract surgery lens capsule.12 On the other hand, it is known that LEC proliferation and tissue fibrosis at an adequate level are beneficial to stabilize the IOL within the capsular bag.4
There has been a recent emphasis on polishing techniques to prevent capsular bag opacification.13–16 However, even extensive polishing cannot completely remove all LECs, and polishing is usually not performed at the capsular bag equator because this region is not readily visible. Therefore, even after well-performed polishing of the capsular inner surface, LECs continue to deposit ECM and lens capsule components at their basal ends, which contributes to the fibrotic thickening of the capsule throughout life, as well as maintaining its integrity.17 Furthermore, there are many apparent dead bag cases that were not associated with extensive polishing, and even in these cases, the capsular bag is floppy and almost free from LECs.5
Although as noted above, LECs are important for the formation of the capsule, this structure represents an anchor point for the basal surfaces of epithelial and fiber cells, also providing necessary signals for proper lens cell proliferation, migration, and differentiation.18 In the DBS, another possibility is that the initial problem is in the capsule itself, which would initiate a cycle of LEC damage with further damage to the capsule.
There are many unanswered questions not only about the etiology of this syndrome, but also in its manifestations. Management is therefore advised on a case-by-case basis, depending on presentation, as well as the status of zonular support. The findings described in this study confirm that scarce or no LECs were present in the capsular bag specimens from DBS cases (limited vimentin), and they suggest that cells were present after surgery, secreted collagen type I and fibronectin, and later died/detached. Further studies are necessary to ascertain the causes of the cell damage leading to LEC disappearance.WHAT WAS KNOWN In the severe end of the spectrum, capsular bags in dead bag syndrome are floppy and devoid of lens epithelial cells and fibrotic changes.
WHAT THIS PAPER ADDS Immunohistochemistry confirmed that scarce or no lens epithelial cells were present in the capsular bags from dead bag syndrome cases and suggested that cells were present after surgery, secreted components of fibrotic posterior capsule opacification, and later died/detached. REFERENCES 1. Apple DJ, Werner L. Complications of cataract and refractive surgery: a clinicopathological documentation. Trans Am Ophthalmol Soc 2001;99:95–107 2. Saika S. Relationship between posterior capsule opacification and intraocular lens biocompatibility. Prog Retin Eye Res 2004;23:283–305 3. Saika S, Yamanaka O, Flanders KC, Okada Y, Miyamoto T, Sumioka T, Shirai K, Kitano A, Miyazaki K, Tanaka S, Ikeda K. Epithelial-mesenchymal transition as a therapeutic target for prevention of ocular tissue fibrosis. Endocr Metab Immune Disord Drug Targets 2008;8:69–76 4. Spalton DJ, Russell SL, Evans-Gowing R, Eldred JA, Wormstone M. Effect of total lens epithelial cell destruction on intraocular lens fixation in the human capsular bag. J Cataract Refract Surg 2014;40:306–312 5. Culp C, Qu P, Jones J, Fram N, Ogawa G, Masket S, Mamalis N, Werner L. Clinical and histopathological findings in the dead bag syndrome. J Cataract Refract Surg 2022;48:177–184 6. Werner L, Zaugg B, Neuhann T, Burrow M, Tetz M. In-the-bag capsular tension ring and intraocular lens subluxation or dislocation: a series of 23 cases. Ophthalmology 2012;119:266–271 7. Liu E, Cole S, Werner L, Hengerer F, Mamalis N, Kohnen T. Pathologic evidence of pseudoexfoliation in cases of in-the-bag intraocular lens subluxation or dislocation. J Cataract Refract Surg 2015;41:929–935 8. Kim SW, Roh J, Park CS. Immunohistochemistry for pathologists: protocols, pitfalls, and tips. J Pathol Transl Med 2016;50:411–418 9. Saika S, Kawashima Y, Miyamoto T, Okada Y, Tanaka SI, Ohmi S, Minamide A, Yamanaka O, Ohnishi Y, Ooshima A, Yamanaka A. Immunolocalization of prolyl 4-hydroxylase subunits, α-smooth muscle actin, and extracellular matrix components in human lens capsules with lens implants. Exp Eye Res 1998;66:283–289 10. Teekhasaenee C, Suwan Y, Supakontanasan W, Tulvatana W, Ritch R. The clinical spectrum and a new theory of pathogenesis of true exfoliation syndrome. Ophthalmology 2016;123:2328–2337 11. Kramer GD, Werner L, Mamalis N. Prevention of postoperative capsular bag opacification using intraocular lenses and endocapsular devices maintaining an open or expanded capsular bag. J Cataract Refract Surg 2016;42:469–484 12. Kurosaka D, Nagamoto T. Inhibitory effect of TGF-β2 in human aqueous humor on bovine lens epithelial cell proliferation. Invest Ophthalmol Vis Sci 1994;35:3408–3412 13. Wang SB, Quah XM, Amjadi S, Tong J, Francis IC. Hydropolish: a controlled trial on a technique to eradicate residual cortical lens fibers in phacoemulsification cataract surgery. Eur J Ophthalmol 2015;25:571–574 14. Liu Z, Cao Q, Qu B, Wang W, Ruan X, Zheng D, Jin G, Tan X, Jin L, He M, Congdon N, Lin H, Luo L, Liu Y. Fluid-jet technique to polish the posterior capsule for phacoemulsification surgeries: efficacy and safety evaluation. J Cataract Refract Surg 2020;46:1508–1514 15. Luft N, Kreutzer TC, Dirisamer M, Priglinger CS, Burger J, Findl O, Priglinger SG. Evaluation of laser capsule polishing for prevention of posterior capsule opacification in a human ex vivo model. J Cataract Refract Surg 2015;41:2739- 2745 16. Menapace R, Di Nardo S. Aspiration curette for anterior capsule polishing: laboratory and clinical evaluation. J Cataract Refract Surg 2006;32:1997–2003 17. Danysh BP, Duncan MK. The lens capsule. Exp Eye Res 2009;88:151–164 18. Oharazawa H, Ibaraki N, Lin LR, Reddy VN. The effects of extracellular matrix on cell attachment, proliferation and migration in a human lens epithelial cell line. Exp Eye Res 1999;69:603–610
Comments (0)