
Remember me
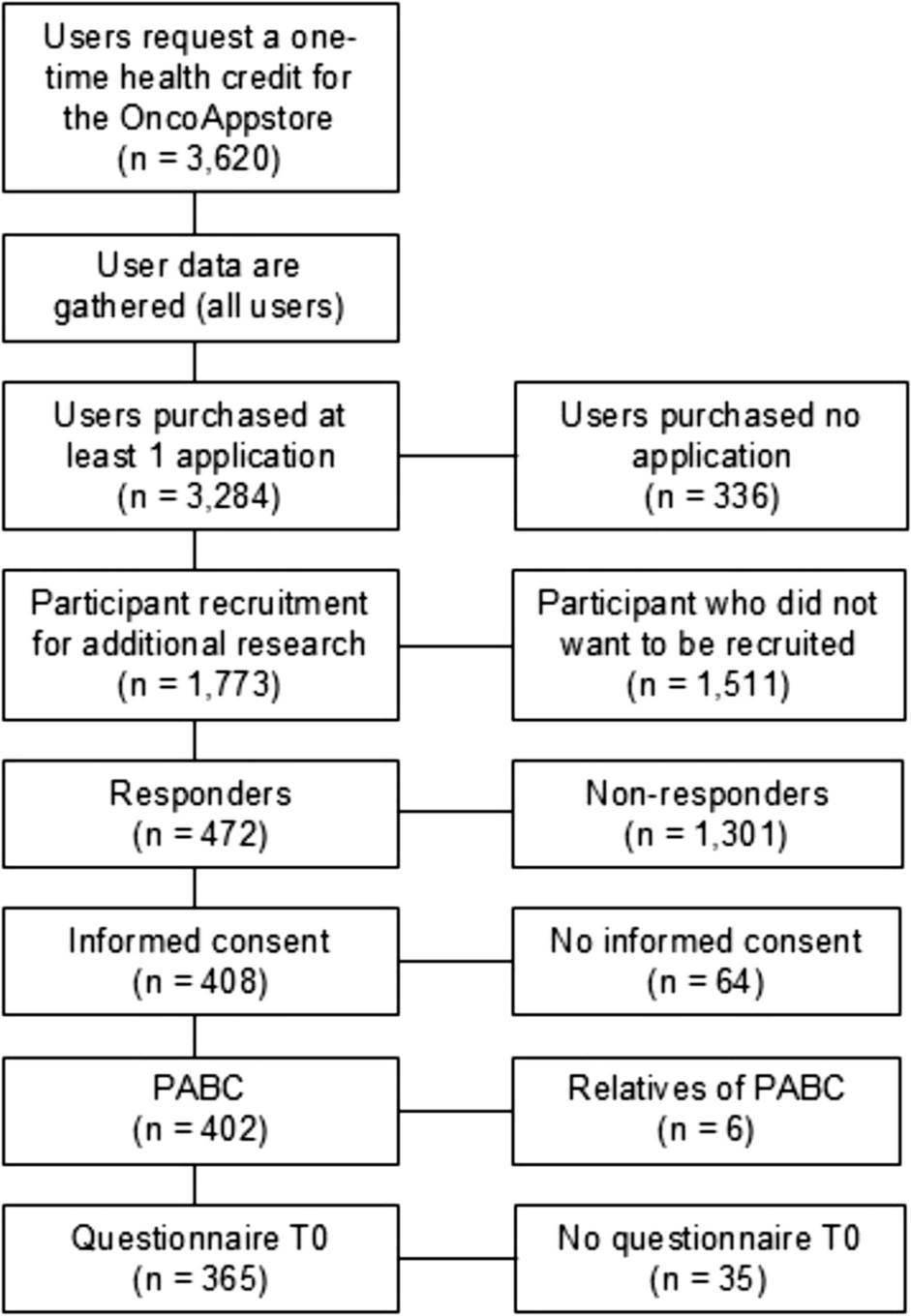
The design of both the PACT and PACES trials has been published previously [14,15,16]. Both trials were performed between 2009 and 2013 in the Netherlands and included patients with a histologically confirmed non-metastatic breast cancer diagnosis who were scheduled to receive chemotherapy. The most important exclusion criteria included any contra-indications for physical activity and not being able to read or understand Dutch [11, 12] (Online Resource 1 contains an overview of the complete in- and exclusion criteria). In the PACT trial (N = 204), recruited patients were randomized to (1) a moderate- to high-intensity, supervised exercise programme or (2) a usual care control group [11, 15]. In the PACES trial (N = 230), patients were randomized to (1) a moderate- to high-intensity, supervised exercise programme, comparable to the PACT study; (2) a home-based, low-intensity exercise programme (Onco-Move), which is excluded from the current analysis due to incomparability with the PACT study (N = 77); or (3) a usual care control group [11, 12]. The two trials combined thus included a total of 357 patients with breast cancer (PACT N = 204; PACES N = 153) (excluding PACES trial participants randomized in the Onco-Move group), of whom 178 were randomized to a moderate- to high-intensity, supervised exercise intervention (PACT N = 102; PACES N = 76) and 179 to usual care (PACT N = 102; PACES N = 77) (Fig. 1) [11, 12].
Fig. 1
Flow chart of the patient flow of the Pact-Paces-Heart study. *=Participants who were randomized into the PACES Onco-Move intervention are not shown as they were excluded from the analyses in this paper
Exercise programmePatients allocated to the supervised intervention arm in the PACT and PACES trials followed a moderate- to high-intensity, combined aerobic and resistance exercise programme, tailored to the participant’s fitness level and guided by a specialized physical therapist [11, 12, 14, 15]. In both trials, patients attended two supervised 1-h training sessions per week and were encouraged to be physically active for 5 days per week for at least 30 min (Online Resource 2). The intervention in the PACT trial incorporated principles of Bandura’s social cognitive theory (i.e. stimulating self-efficacy via mastery experience, observational experience and verbal persuasion) to encourage maintenance of physical activity after completion of the trial [15]. In the PACES trial, physical activity maintenance was stimulated through the use of the ‘active living’ method and the distribution of written information about physical activity tailored to the stage of change of participants [14]. Neither intervention included additional psychological support. Timing of the interventions differed slightly between the studies. In the PACT trial, participants exercised for 18 weeks, which overlapped, at least partly, with their chemotherapy. In the PACES trial, participants started the exercise programme at the first cycle of chemotherapy and continued until 3 weeks after the last cycle (on average 16 weeks). Patients in the control group in both studies received usual care as specified by hospital guidelines and were asked to maintain their regular physical activity level throughout the study period [9, 17,18,19]. Given that the PACT and PACES supervised exercise groups followed similar exercise programmes, their data were combined in the current analysis, as were the data from the two usual care control groups.
Pact-Paces-Heart studyFor the current follow-up study, all patients with breast cancer who participated in either the PACT or PACES trial and were still alive were eligible for recruitment. Participants were excluded if they were deemed ineligible by their treating physician (e.g. too mentally burdensome or severe neuropathy); had declined to be invited for future studies; were treated with chemo-, targeted, or thoracic radiotherapy for recurrent breast cancer; or were treated with systemic or thoracic radiotherapy for other malignancies than breast cancer (excluding non-melanoma skin cancer) after completion of the initial trial (Online Resource 1).
The participants in the 4-year follow-up PACT study [9] who had provided consent to be approached for future follow-up studies were, after screening for eligibility, directly approached by the research team for participation in the current study. The remaining original PACT participants, if they had not declined to be invited for future studies, and all PACES trial participants were approached by their treating physician. Eligible participants were invited for a study visit at the University Medical Centre Utrecht for informed consent procedures and outcome assessments including online questionnaires thereafter. The study was approved by the Medical Ethics Committee of the University Medical Centre Utrecht (METC 18/136).
Outcome measuresThe primary endpoints of the Pact-Paces-Heart study were cardiovascular outcomes to assess the long-term cardiotoxicity of chemotherapy treatment and are reported in a separate paper [13]. The follow-up time of approximately 8 years was chosen to allow enough time for the development of possible cardiac damage. Here, we report on the simultaneously assessed PROs, including fatigue, anxiety and depression and HRQoL, together with the combined PRO results from earlier timepoints.
In the PACT trial, outcomes were assessed at baseline (T0), post-intervention (i.e. after 18 weeks, T1) and 36 weeks post-baseline (T2). Outcomes were assessed at similar timepoints in the PACES trial, namely at baseline (T0), after completing chemotherapy (T1) and 6 months after chemotherapy completion (T2). Additionally, in a 4-year post-baseline follow-up study, fatigue and HRQoL, but not anxiety and depression, were again assessed for 110 patients from the PACT trial (exercise N = 59; usual care N = 51) (T3) [9]. PROs were assessed using the same questionnaires as used in both the PACT and PACES trials (i.e. the Multidimensional Fatigue Inventory (MFI) for fatigue, the Hospital Anxiety and Depression Scale (HADS) for anxiety and depression and the European Organisation for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire (QLQ-C30) for HRQoL). For the analysis of fatigue, only the general and the physical fatigue subscales from the MFI were used, because of their reported reliability [20] and a hypothesized probable effect of exercise, respectively [11, 12].
In addition to measurements of PROs at the 8-year follow-up, physical activity levels were also assessed. The validated Short Questionnaire to Assess Health-enhancing physical activity (SQUASH) was used for this assessment [21].
Baseline characteristicsSociodemographic data (i.e. sex, age and educational level), data regarding cancer (i.e. receptor status) and treatment characteristics (i.e. radiotherapy (yes/no)) were recorded at baseline in both the PACT and PACES trials via medical record examination. Physical activity levels at baseline were assessed via questionnaires, i.e. the SQUASH for PACT trial participants and the Physical Activity Scale for the Elderly in the PACES trial participants. Baseline characteristics for both the study sample that completed the 8-year follow-up for the Pact-Paces-Heart study and the sample that did not complete the follow-up will be presented, to allow for assessment for possible selective loss-to-follow-up.
Statistical analysesAll statistical analyses were performed using R (version 4.2.2) and Rstudio (Version 2023.06.0; Rstudio Inc., Boston, MA). Baseline characteristics of the 8-year follow-up study sample and of those women from the original trials who did not participate in the follow-up study were summarized using descriptive statistics. For the HADS anxiety and depression scores, both mean values and categorical threshold values were calculated, with a score of 0–7 corresponding to ‘non-case’, 8–10 to ‘doubtful case’ and 11–21 to ‘probable case’ [22]. Frequencies of each category per treatment arm and timepoint were reported. To gain insight into fatigue and quality of life in the study sample, as compared to the general population, MFI and EORTC QLQ-C30 outcomes were compared to available reference values based on German and Dutch general population samples, respectively, stratified by age and sex [23, 24].
To analyse the potential short- and long-term effect of the exercise intervention on the PROs, we used intention-to-treat, linear mixed-effects models with a random intercept and unstructured covariance structure. Questionnaire scores from participants with data of at least two timepoints were entered in the model. We adjusted the models for education level (low, middle or high), age, initial study (PACT or PACES), tumour receptor status (triple negative; Her2Neu + and oestrogen receptor (ER) + or progesterone receptor (PR) + ; Her2Neu + ER/PR − ; Her2Neu − ER/PR +) and the respective baseline PRO scores. Time and group assignment were entered in the model both separately and as an interaction term. With the mixed models, marginal means for the questionnaire scores at all timepoints were estimated for the pooled exercise and usual care groups. Between-group differences at all post-baseline timepoints with corresponding 95% confidence intervals were calculated to assess any significant difference between the exercise and usual care groups. Standardized effect sizes (ESs) were calculated per timepoint by dividing the adjusted between-group differences by the pooled standard deviations at baseline. Using Cohen’s interpretation, ESs < 0.2 correspond to ‘no difference’, ESs between 0.2 and 0.5 to ‘small differences’, 0.5–0.8 to ‘moderate differences’ and ESs > 0.8 correspond to ‘considerable differences’ [25].
To assess selective loss-to-follow-up in the combined study sample, mean PRO scores at baseline, T1 and T2 were compared between the groups that were successfully recruited into the Pact-Paces-Heart study and the groups that were not. The statistical significance of the difference between the means was assessed with unpaired t-tests. For all analyses, p-values smaller than 0.05 were considered statistically significant.
Comments (0)