

Remember me
Podcasts continue to increase in popularity as a resource for entertainment and knowledge acquisition.1 Use has spread across countries, specialties, and learner levels, with increasing formal incorporation into medical student and residency curricula.2–4 This use has paralleled the increase in free open-access medical education and asynchronous learning in residency education.5 Approximately 90% of residents listen to podcasts regularly, which serve as both a primary source of information and a major resource for reviewing the medical literature.6–8 Residency training is demanding and time intensive; therefore, learners often seek methods in which to multitask to ensure successful completion of their responsibilities. One particular efficiency strategy is to listen to podcasts while completing other tasks (e.g., driving, exercising, and cleaning).9
Despite the increasing popularity of this approach, the impact of such multitasking on acquisition and retention of learned podcast content in graduate medical education remains limited.10–12 The phenomenon of cognitive-motor interference (CMI) occurs when simultaneous performance of a cognitive task (e.g., listening to a podcast) and a motor task (e.g., exercising) impairs or enhances performance measures for one or both tasks, relative to the performance of each task separately.13,14 Given the broad and nuanced nature of this topic, studies investigating CMI have largely yielded conflicting results.15
Several different types of theories offer insight into the mixed effects of CMI on long-term memory.15 Arousal theories postulate that the dual increase in metabolic activity and physical activity during exercise impacts neuromodulation, and such theories hypothesize that exercise-induced arousal enhances mental performance with moderate, but not high, levels of arousal.15 Attention theories contend that attention selectively allows sensory information to enter consciousness and impacts its processing via working memory.15 Similarly, cognitive theories suggest a limited operational capacity of working memory.16 Consequently, competing information in short-term working memory may impede long-term memory storage.15,16
Because podcast learning is a relatively new phenomenon, these theoretical influences on learning have yet to be extensively tested in health professions education. Given the prominent use of podcasts among learners, it is imperative to critically explore their use. The primary objective of this study was to examine whether physical activity in the form of exercise influences knowledge acquisition and retention from podcasts when compared with sitting undistracted in a room. A secondary objective was to examine learner perception of knowledge acquisition when exercising compared with sitting in a room without distraction.
Method Study settingThis multicenter, randomized, crossover trial compared knowledge acquisition and retention after listening to a podcast while exercising compared with being seated undistracted in a room. This study was conducted at 5 emergency medicine (EM) residency training programs located within the United States from September 2022 to January 2023. These study sites were intentionally selected to represent a range of locations and program types to increase the generalizability of the findings. Rush University Medical Center is an urban academic postgraduate year (PGY)–1 to PGY-3 residency program located in Chicago, Illinois. Geisinger Medical Center is a rural community–academic PGY-1 to PGY-3 residency program located in Danville, Pennsylvania. The Ohio State University Wexner Medical Center is an urban academic PGY-1 to PGY-3 residency program in Columbus, Ohio. The University of Michigan is an urban academic PGY-1 to PGY-4 residency program in Ann Arbor, Michigan. The University of Southern California Keck School of Medicine is an urban county PGY-1 to PGY-4 residency program in Los Angeles, California. We recruited all PGY-1 to PGY-4 EM residents who were interested in participating at each study site. We excluded residents who were unable to exercise for at least 30 continuous minutes. Participation was optional, and residents received $75 for completion of the study. This study was approved by the local institutional review board at each study site.
Study designThis study was conducted in accordance with best practice recommendations and adhered to the Consolidated Standards of Reporting Trials guidelines extension for randomized, crossover trials.17 Residents were block randomized by PGY and site into the exercise group or the seated group. The exercise group listened to a 30-minute podcast while continuously exercising for 30 minutes. The exercise group could perform any form of indoor aerobic exercise (e.g., stationary bike, running, stair-climbing, and elliptical) but could not listen while weightlifting, attending an aerobic class, or exercising outdoors. They were instructed not to split up the podcast across multiple exercises. The seated group listened to the same 30-minute podcast while seated at home and without performing other activities.
After listening to the podcast, each group completed an identical 20-item test assessing immediate recall of the podcast information. They also completed a self-assessment of perceived knowledge retention using a 100-point scale. Learners were asked to complete the knowledge acquisition test and self-assessment of knowledge acquisition within 30 minutes of listening to each podcast. Learners were explicitly told that they should not consult any resources (including relistening to the podcast or reading the articles discussed in the podcasts) before or during any of the tests.
The groups then crossed over (i.e., the seated group became the exercise group and vice versa). Each group subsequently listened to a different 30-minute podcast and completed a 20-item test based on this second podcast, allowing each group to serve as their own control. We did not use a washout period because the topics were different between the 2 podcast groups. Finally, we assessed delayed recall at 30 days after completing both podcasts using a third question set that comprised 40 new questions (20 questions per podcast group allocation).
Podcast creationEach 30-minute podcast consisted of a discussion of 5 journal articles, with each article being presented during a 6-minute segment. All 5 journal article segments were then combined with audio instructions as a complete podcast. The selected podcast segments were used (with permission) from previous years of an originally produced medical education podcast in which 2 hosts discuss up to 30 EM-relevant journal articles per month (Emergency Medicine Abstracts; https://www.emrap.org/ema). This podcast was chosen because it was realistic, represented existing podcasts in the marketplace, was hosted by experienced podcasters, and did not have an extensive reach among EM residents.
Articles (and their corresponding podcast segments) were selected by the investigators based on their relevance to EM. Articles were screened by all study investigators to ensure that they were not previously discussed in any of the respective residency program curricula or journal clubs. Podcasts that were syndicated on major EM podcast programs, published in an EM journal, or discussed on social media (defined as appearing within the first 10 results on www.googlefoam.com) were excluded.
Question developmentTo assess the effect of listening to podcasts while exercising versus listening while seated without distractions, the research team developed two 20-item tests to assess immediate recall and one 40-item test to assess delayed recall. Each test consisted of multiple-choice items with 4 options that were listed alphabetically with a single best answer, following best practices in test-item creation.18 As previously described, 101 questions were drafted by experienced EM physicians with extensive experience writing test questions.9 The questions included both recall of specific study characteristics (e.g., study location, study population, and specific interventions) and overarching main conclusions (i.e., key take-home points from the study) drawn from each of the podcasts. Questions were piloted among 10 EM resident physicians with at least 2 resident physicians from each institution and from each PGY level. The resident physicians involved in the pilot study were not associated with the subsequent study. Feedback was sought regarding the wording, difficulty, and format by using read-aloud and cognitive interviewing strategies.19 The internal consistency of each test was established during the pilot phase of the study using the Cronbach α.20 Two examination performance measures were used to conduct item analysis: item difficulty and discrimination index. Questions with high difficulty (< 0.4) and a low discrimination index (< 0.2) were removed, yielding 80 total questions (40 per podcast). The final Cronbach α values for test 1 and test 2 were 0.70 and 0.71, respectively. The test difficulty was set at approximately 0.76 for each version. The final test included 31 pure recall questions (38.8%) and 49 conceptual questions (61.2%), which were distributed relatively evenly between the 2 versions. In addition, residents were asked to rate what percentage of information they believed that they retained using a 0% to 100% visual analog scale immediately before initiation of each test, with 0% indicating no retention and 100% indicating complete retention. All surveys were distributed through REDCap, version 13.6.1 (Vanderbilt University, Nashville, Tennessee).
Statistical analysisBasic demographics were presented using descriptive statistics. The mean (SD) scores were calculated for each group. A paired-sample t test was used to analyze the differences in knowledge retention between the 2 conditions. To examine the role of self-perceived knowledge retention, we used Pearson correlation and a paired-sample t test. We excluded PGY level as a potential covariate in all analyses because the Pearson correlation coefficients did not reach statistical significance in any conditions. The analyses were conducted using SPSS software, version 28.0 (IBM Corp, Armonk, New York).
An a priori power calculation was performed for sample size estimation. On the basis of a review of the literature, to achieve a moderate effect size measured by the Cohen d (d = 0.18), with an α = 0.05 and power of 0.95, the sample size needed for this study was 45. To account for potential dropouts and loss to follow-up, we aimed to recruit at least 90 residents.
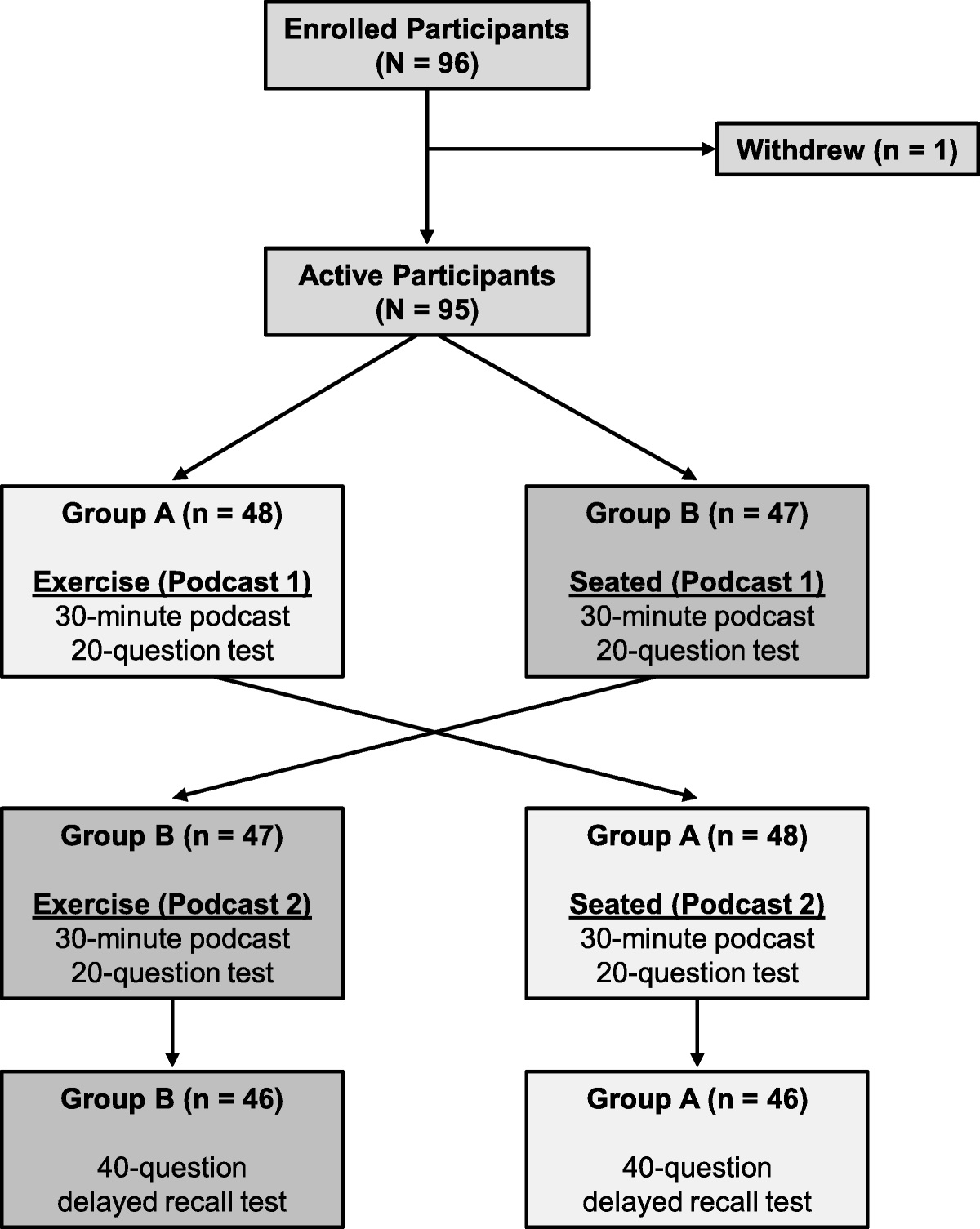
ResultsNinety-six residents were recruited for the study. One resident dropped out before completing the initial podcasts and was excluded from the study, leaving a total of 95 residents (99.0%) in the study. All 95 residents completed the immediate recall surveys and were analyzed for this outcome. Three residents did not complete the 30-day delayed recall test, leaving 92 residents (97.0%) who were able to be analyzed for delayed recall (Figure 1). There were relatively equal distributions of residents from all 5 sites across PGY levels (Table 1).
 Figure 1:
Figure 1: Flow diagram of emergency medicine residents through enrollment, initial assessment, and delayed recall assessment in the podcast study.
Table 1 - Demographic Characteristics of the Emergency Medicine Residents Who Participated in the Podcast Exercise Study, September 2022 to January 2023 Characteristic No. of participants Study site Geisinger Medical Center 19 Rush University Medical Center 21 The Ohio State University Wexner Medical Center 16 University of Michigan 24 University of Southern California Keck School of Medicine 15 Postgraduate year 1 43 2 27 3 21 4a 4aOnly 2 sites included postgraduate year 4 residents.
In the immediate recall groups, residents achieved a mean (SD) score of 74.4% (11.8%) in the exercise group and 76.3% (12.6%) in the seated group. The difference in scores was not significant (d = −0.12; 95% CI, −0.33 to 0.08; P = .12). The mean (SD) scores on the delayed recall survey were 52.3% (12.5%) in the exercising group and 52.5% (14.7%) in the seated group. The difference in scores did not reach statistical significance (d = −0.01; 95% CI, −0.22 to −0.19; P = .46). Among the 92 residents who completed both the immediate and delayed recall surveys, the mean (SD) score decreases from immediate recall to delayed recall were 21.9% (15.4%) for the exercising group and 23.8% (16.5%) for the seated group. The difference in score loss between the 2 conditions (exercising and seated) did not reach statistical significance (d = 0.09; 95% CI, −0.12 to 0.29; P = .21).
When examining the pattern of the effect at the individual resident level (unit of measurement), the decrease in their delayed recall score affected them equally in both conditions, meaning their performance on the delayed recall test was not a function of how they did on the immediate recall test (Figure 2). In this crossover design, we also examined whether the order of conditions in which the residents listened to the podcast (i.e., seated condition first vs seated condition second) affected their performance on delayed recall testing. The pattern of performance illustrated in Figure 3 demonstrates that the order did not influence recall in either the immediate or delayed recall testing group.
 Figure 2:
Figure 2: Comparison of changes in emergency medicine resident scores in the group that listened to one 30-minute podcast while seated compared with the group that listened to a 30-minute podcast while engaging in 30 minutes of continuous aerobic exercise. A. Seated versus exercising recall decline between immediate and delayed testings. The parallel line plot in the center of this hybrid graph plots individual residents’ score changes from immediate to delayed recall in both the seated and exercising conditions. The 2 box plots adjacent to the parallel line plot compare group means between immediate and delayed recall in both conditions. B. Comparison of score changes between seated and exercising conditions. The box plot to the right of the graph shows the mean score differences (delayed recall minus immediate recall) between the seated and exercising conditions.
 Figure 3:
Figure 3: Comparison of sitting versus exercising on immediate recall (A) and delayed recall (B) scores in emergency medicine residents in a group that listened to one 30-minute podcast while seated compared with a group that listened to a 30-minute podcast while engaging in 30 minutes of continuous aerobic exercise.
When examining residents’ perceived knowledge acquisition in each condition, residents reported a higher mean (SD) percentage of knowledge retention in the seated group (67.0% [14.0%]) than in the exercising group (64.0% [13.0%]), with a mean difference of 3.6% (95% CI, 0.4%–6.8%). The magnitude of the difference had a moderate effect size (d = 0.23; 95% CI, 0.02–0.43; P = .02). In both the exercising and seated conditions, there was a moderate and statistically significant relationship between self-assessed knowledge acquisition and tested knowledge recall. This relationship had a moderate effect size under the seated condition (r = 0.36; 95% CI, 0.17–0.52; P < .001) and a small effect size under the exercising condition (r = 0.25; 95% CI, 0.05–0.43; P = .01).
DiscussionIn this multicenter, randomized, crossover trial comparing EM residents’ knowledge acquisition and retention after listening to a podcast while exercising compared with being seated and undistracted in a room, we found no important differences in immediate or delayed recall between the 2 listening conditions. Although a small effect size was found in the knowledge retention group, the educational impact of this difference is not meaningful (i.e., < 1 question difference).
These findings are consistent with a prior crossover trial by Gottlieb et al9 that randomized residents to listen to a podcast while driving versus while sitting undistracted. The authors found no statistically significant difference between the driving and undistracted conditions on both initial recall (74.2% vs 73.3%) and delayed recall (52.2% vs 52.0%). Although both studies assessed CMI, the current study introduced the variable of metabolic activity and removed the cognitive load necessary for driving. Despite these methodological differences, they generated strikingly similar results.
The 2 leading factors theorized to influence the exercise-cognition relationship explored in the current study are arousal and attention.21 Arousal theories suggest that there is an optimal level of arousal during exercise that can contribute to cognitive preservation or facilitation and, as metabolic activity increases with physical activity, alterations in brain neuromodulation occur.22 The relationship between arousal and cognitive function is complex, with data suggesting that a combination of exercise and learning may negatively impact long-term memory.15 Previous findings, however, suggest mental performance can actually be enhanced with moderate, but not high, levels of arousal from exercise.23 In general, the cognitive benefits of exercise are maximized in moderate-intensity exercise, such as ergometer cycling, that lasts at least 20 minutes.21 The fact that we did not see a decrease in knowledge gained during exercise could stem from the type of exercise that residents did while listening. Rather than controlling for the mode, duration, and intensity of exercise in a laboratory, we opted for a pragmatic study of the real-world habits of EM residents. Given the length of the podcasts in this study and the popularity of moderate-intensity exercise, such as cycling,24 many participants may have been performing exercise that falls within the narrow window of optimal metabolic arousal. Such exercises may have balanced out any negative effects of other forms of exercise, thereby resulting in a net neutral effect when evaluated in aggregate.
Attention theories might also explain our findings. These theories assume that attention, not arousal, functions as a gate that determines which sensory experiences enter our consciousness and how they are manipulated into memory. Cognitive overload among items held in short-term working memory can theoretically compromise transfer into long-term memory.15,25 Exercise demands attention, and therefore only residual attention may be left to dedicate to cognition. Exercises such as stair climbing, which require substantial attention to balance, form, and moving steps, can result in decreased cognitive capacity. On the other hand, activities such as recumbent cycling require minimal attention and result in no change in cognition.21 Again, it is possible that our participants engaged in exercises that required little motor movement planning or corrections. Because complex outdoor activities, such as hiking and bouldering, were not allowed in this study, there may have been fewer factors that competed with the ability to process cognitive tasks and thus minimal effect on the encoding of information from a podcast.
Residents perceived that they had greater knowledge acquisition when listening while seated as opposed to during exercise despite no difference in their actual acquisition and retention. This finding is consistent with another podcast study that found discordance between perceived and actual knowledge acquired with driving versus being seated and undistracted.9 When examining perception versus actual knowledge at the individual level, learners had reasonable ability to predict this, with effect sizes ranging from small to moderate. This finding may suggest a perceived bias among learners that exercise decreases knowledge acquired.
Given the competing priorities associated with residency training, podcast use will likely remain prevalent. Therefore, these findings should assuage residents who worry that listening to podcasts while engaging in other activities, such as aerobic exercise, is less effective despite perceptions from our participants and in other work.1 Those who listen to podcasts while exercising can take away 2 key points: (1) their learning is likely no worse than if they listened at home, and (2) they are likely to retain approximately half of what they hear, regardless of whether the listening occurred during exercise or at rest (accounting for potential enhanced long-term retention in this study due to the testing effect from the immediate posttest). These long-term effects are consistent with other studies of podcast retention among EM residents.9,26
Podcast creators should also note the retention rates, as well as the notable decay in retention over time, mirroring the rates seen with other passive learning strategies. Incorporating active learning strategies into podcasts (e.g., pause procedures, encouraging note taking, concept maps, and end-of-podcast quizzes) may mitigate this effect and serve as an area of continued future study to maximize the impact of this popular instructional medium.26,27
Future studies might investigate the impact of how different types and durations of exercise influence learning. In addition, assessing participants’ heart rates during exercise may provide a more nuanced understanding of the optimal conditions for learning from podcasts. Research should also assess which strategies can improve retention at 30 days.
LimitationsThis study has several important limitations. This study was performed among EM residents, and outcomes may not reflect other specialties or levels of learner. In addition, the Hawthorne effect may have increased active engagement among participants. Although instructions provided guidance as to the type of eligible exercise, we did not track exercise type or degree of intensity, which may have influenced knowledge acquisition or retention. It is also possible that CMI may have caused the exercise task to suffer while sparing a decrease in retention, but physical performance was not measured. This possibility may matter for those residents pursuing an exercise goal or training for a physical challenge that depends on sustained or measured exercise performance. Although residents were asked to listen to the podcast continuously for a single exercise or seated session and complete the test within 30 minutes of completion, we did not track this, and it is possible that some participants did not adhere to the instructions. Moreover, some residents may have previously seen the articles despite attempts to minimize this likelihood by ensuring no included articles were covered in existing residency curricula, published in EM journals, or prominently featured online. Randomization with stratification by site and learner level as well as the use of a crossover design with each resident serving as their own control further lower this risk. Finally, we limited our knowledge retention assessment to 30 days, and future research is needed to determine whether there may be a difference in retention beyond this period.
ConclusionsThis multicenter, randomized, crossover study demonstrated that listening to a podcast while exercising did not meaningfully impact immediate knowledge acquisition or delayed knowledge retention. Educators and learners may consider using podcasts as an asynchronous learning resource during activities, such as exercising.
AcknowledgmentsThe authors would like to thank all the emergency medicine residents at the corresponding institutions who participated in the study.
Funding/SupportThis study was funded by an unrestricted educational grant from Emergency Medicine: Reviews and Perspectives. The sponsor did not have any involvement in the design, data collection, or decision to publish the study.
Other disclosuresNone reported.
Ethical approvalThis study was approved by the Rush University Medical Center institutional review board (IRB), November 11, 2021 (#21110509-IRB01); the Geisinger Medical Center IRB, April 12, 2022 (#2022-0216); The Ohio State University Wexner Medical Center IRB, December 14, 2021 (#2021H0408); The University of Michigan IRB, December 14, 2021 (#HUM00208906); and the University of Southern California Keck School of Medicine IRB, March 29, 2022 (#UP-21-01080).
References 1. Riddell J, Robins L, Brown A, Sherbino J, Lin M, Ilgen JS. Independent and interwoven: a qualitative exploration of residents’ experiences with educational podcasts. Acad Med. 2020;95(1):89–96. 2. Kelly JM, Perseghin A, Dow AW, Trivedi SP, Rodman A, Berk J. Learning through listening: a scoping review of podcast use in medical education. Acad Med. 2022;97(7):1079–1085. 3. Estes M, Gopal P, Siegelman JN, Bailitz J, Gottlieb M. Individualized interactive instruction: a guide to best practices from the council of emergency medicine residency directors. West J Emerg Med. 2019;20(2):363–368. 4. Yilmaz Y, Chan TM, Thoma B, et al. Identifying social media competencies for health professionals: an international modified Delphi study to determine consensus for curricular design. Ann Emerg Med. 2022;79(6):560–567. 5. Chan TM, Stehman C, Gottlieb M, Thoma B. A short history of free open access medical education: the past, present, and future. ATS Sch. 2020;1(2):87–100. 6. Mallin M, Schlein S, Doctor S, Stroud S, Dawson M, Fix M. A survey of the current utilization of asynchronous education among emergency medicine residents in the United States. Acad Med. 2014;89(4):598–601. 7. Purdy E, Thoma B, Bednarczyk J, Migneault D, Sherbino J. The use of free online educational resources by Canadian emergency medicine residents and program directors. CJEM. 2015;17(2):101–106. 8. Riddell J, Swaminathan A, Lee M, Mohamed A, Rogers R, Rezaie SR. A survey of emergency medicine residents’ use of educational podcasts. West J Emerg Med. 2017;18(2):229–234. 9. Gottlieb M, Riddell J, Cooney R, King A, Fung CC, Sherbino J. Maximizing the morning commute: a randomized trial assessing the effect of driving on podcast knowledge acquisition and retention. Ann Emerg Med. 2021;78(3):416–424. 10. Lang A. Defining audio/video redundancy from a limited-capacity information processing perspective. Commun Res. 1995;22(1):86–115. 11. Lang A, Basil M. Attention, resource allocation, and communication research: what do secondary task reaction times measure anyway? Ann Int Commun Assoc. 1998;21(1):443–458. 12. Lang A. The limited capacity model of mediated message processing. J Commun. 2000;50(1):46–70. 13. Plummer P, Eskes G, Wallace S, et al. Cognitive-motor interference during functional mobility after stroke: state of the science and implications for future research. Arch Phys Med Rehabil. 2013;94(12):2565–2574.e6. 14. Abernathy B. Dual-task methodology and motor skills research: some applications and methodological constraints. J Hum Mov Stud. 1988;14(3):101–132. 15. Tomporowski PD, Qazi AS. Cognitive-motor dual task interference effects on declarative memory: a theory-based review. Front Psychol. 2020;11:1015. 16. Paas F, Sweller J. An evolutionary upgrade of cognitive load theory: using the human motor system and collaboration to support the learning of complex cognitive tasks. Educ Psychol Rev. 2012;24(1):27–45. 17. Dwan K, Li T, Altman DG, Elbourne D. CONSORT 2010 statement: extension to randomised crossover trials. BMJ. 2019;366:l4378. 18. Gottlieb M, Bailitz J, Fix M, Shappell E, Wagner MJ. Educator’s blueprint: a how-to guide for developing high-quality multiple-choice questions. AEM Educ Train. 2023;7(1):e10836. 19. Hill J, Ogle K, Gottlieb M, Santen SA, Artino AR. Educator’s blueprint: a how-to guide for collecting validity evidence in survey-based research. AEM Educ Train. 2022;6(6):e10835. 20. Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ. 2011;2:53–55. 21. Zabriskie HA, Heath EM. Effectiveness of studying when coupled with exercise-induced arousal. Int J Exerc Sci. 2019;12(5):979–988. 22. McMorris T, Hale BJ. Is there an acute exercise-induced physiological/biochemical threshold which triggers increased speed of cognitive functioning? A meta-analytic investigation. J Sport Health Scie. 2015;4(1):4–13. 23. McMorris T, Graydon J. The effect of incremental exercise on cognitive performance. Int J Sport Psychol. 2000;31:66–81. 24. Curry D. Peloton revenue and usage statistics (2023). Accessed March 6, 2023. https://www.businessofapps.com/data/peloton-statistics/. 25. Sweller J. Measuring cognitive load. Perspect Med Educ. 2018;7(1):1–2. 26. Weinstock M, Pallaci M, Aluisio AR, et al. Effect of interpolated questions on podcast knowledge acquisition and retention: a double-blind, multicenter, randomized controlled trial. Ann Emerg Med. 2020;76(3):353–361. 27. Wolff M, Wagner MJ, Poznanski S, Schiller J, Santen S. Not another boring lecture: engaging learners with active learning techniques. J Emerg Med. 2015;48(1):85–93.
Comments (0)