
Remember me








Ostomy surgery prevents mortality or significantly reduces morbidity in multiple malignant or benign conditions, but stoma formation also exposes patients to short- and long-term complications that may have negative effects on peristomal skin health and health-related quality of life (QoL).1-5 Living with an ostomy necessitates use of pouching systems (skin barrier and pouch) for safe collection of effluent from the ostomy. Since the inception of pouching systems in the 1950s, new features have gradually been implemented to better accommodate user needs,6 such as filters for odor control,7 skin barriers with different shapes for people with different peristomal body profiles,8 various kinds of accessories,9 and digital sensors for leakage control.10,11
Peristomal body profiles vary from person to person and may change over time. The abdominal topography around an ostomy may turn inward or outward, may bulge due to a parastomal hernia, or develop creases or folds.12 Proper assessment of the abdominal and peristomal body profile is important for selection of the most favorable pouching system to provide a secure seal and protect the peristomal skin.13 Choice of skin barrier type (flat, convex, or concave) depends on the shape of the peristomal area.12 Convex skin barriers have been designed for people with an inward peristomal body profile, where the peristomal area is settled below the surrounding abdomen, or where the ostomy is flush with the peristomal area, to create protrusion of the stoma. In contrast, concave skin barriers have been designed for people with an outward peristomal body profile, for example, people with a hernia, to ensure a better fit of the skin barrier on curved body shapes.8,14 In a large multinational study, approximately half the participants had a flat peristomal body profile, 35% had an outward peristomal body profile and 13% had an inward peristomal body profile.15
Improper fit between the skin barrier and peristomal area is a common reason for undermining and leakage among people living with an ostomy,16 and WOC nurses have rated body profiles and incorrect product usage as key reasons for experiencing undermining and leakage.17 Leakage of effluent has negative physical and psychological effects.2,18,19 Leakage may lead to embarrassing situations, leaving people with increased anxiety related to the possibility of leakage, and overall, it exerts a negative impact on QoL.2,19 Furthermore, effluent situated on the skin is a key determinant for development of peristomal skin complications (PSCs).18
Application of flat skin barriers on curved body shapes can result in the development of folds and wrinkles, enhancing the risk for undermining and leakage.8 People with an outward peristomal body profile have an increased risk of experiencing leakage incidents compared with people having a regular peristomal body profile.15 As a result, selection of a pouching system including the optimal skin barrier shape is important, and use of a body assessment tool for selection of the most favorable fitting pouching system led to significant reductions in the number of leakages and concomitant improvement in QoL in one study.16 Despite the increased risk of experiencing leakage for people with an outward peristomal body profile,15 we searched the literature and found a paucity of research evaluating the performance of concave skin barriers.
The primary aim of this randomized-controlled, cross-over trial was to compare body fit of a two-piece pouching system with a concave skin barrier to a two-piece pouching system with a flat skin barrier in individuals living with an ostomy and having an outward peristomal body profile. Secondary aims were to compare the concave and flat comparator pouching systems regarding degree of leakage, wear time and QoL.
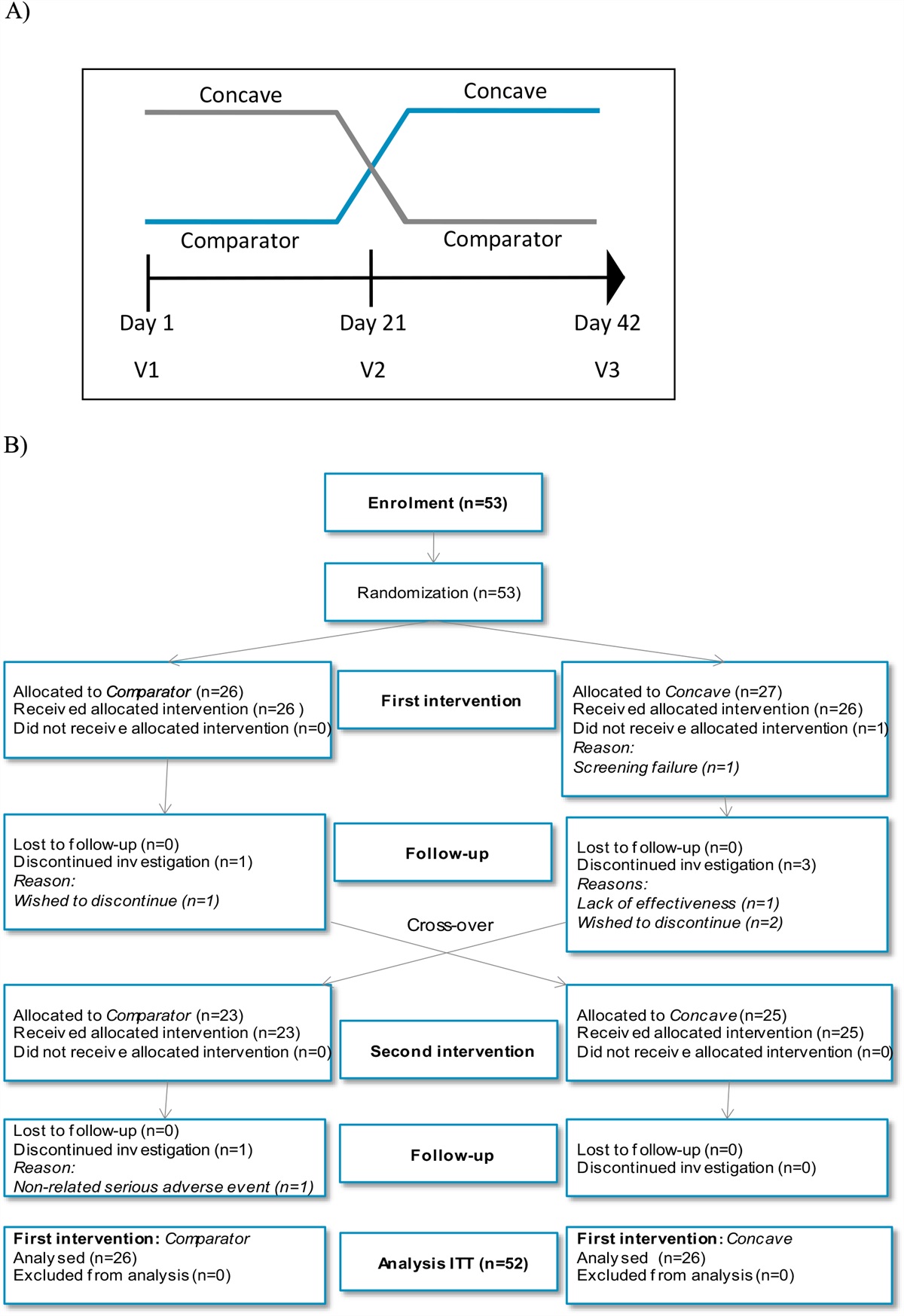
METHODSWe conducted a randomized, controlled, open-label (due to visual appearance of the test products), cross-over trial with two test periods and each period being 21 ± 3 days (Figure 1A and B). Data were collected from February 2015 to May 2015 in Denmark, Norway, Germany, and the Netherlands. The study is listed on www.ClinicalTrials.gov with ID NR: NCT02362360 and follows CONSORT guidelines.20 Figure 1.:
Figure 1.:
Overview of study and study flow-chart. (A) The study was designed as a randomized, controlled, open-label, cross-over investigation with two test periods, with each test period being 21 ± 3 days. Participants were randomized to use of either a concave two-piece pouching system or flat comparator two-piece pouching systems crossing over to the other solution at V2. Three study visits were scheduled (V1, V2, and V3). (B) Study flow-chart. Abbreviations: ITT, intention-to-treat.
Potential study participants were found via databases maintained by Coloplast A/S and were contacted by either letter, e-mail, or phone as first contact. All subjects who were interested and found eligible based upon study inclusion/exclusion criteria were consecutively enrolled into the investigation. Inclusion criteria were >18 years of age, living with an ileostomy or a colostomy for at least 3 months, self-managed ostomy pouching system, and used a two-piece flat product with mechanical coupling before enrollment. An additional inclusion was having an outward peristomal body profile. Having an outward area was operationally defined as having an ostomy located on a bulge on the abdomen (the bulge should be 6-30 cm in diameter and at least 2 cm in height). The outward area could be attributable to a parastomal hernia. Finally, eligible participants must have experienced leakage of fecal effluent underneath the skin barrier at least 3 times per 2 weeks. Exclusion criteria were having a loop stoma, experiencing severe PSCs resulting in bleeding and/or broken skin, or irrigation of their stoma. Additional exclusion criteria were currently receiving or history of chemotherapy or radiation therapy within the past 2 months, history of topical steroid treatment to the peristomal skin area in the past month, known hypersensitivity to any components of the concave or comparator ostomy pouching system, and females who were pregnant or breastfeeding. Study procedures were reviewed and approved by ethics committees or boards in Denmark (De Videnskabsetiske Komiteer; H-4-2014-126), Norway (Regionale komiteer for medisinsk og helsefaglig forskningsetik; 2014/2204 REK sør-øst D), Germany (Ethik-Kommision bei der Landesärtzekammer Baden-Würternberg; MP-2014-010-ff), and the Netherlands (Stichting Beoordeling Ethiek Biomedisch Onderzoek; NL51925.056.14).
Outcome Measures and InstrumentsThe primary objective of this trial was to investigate the body fit of 2 different skin barrier shapes (concave vs. flat) on individuals with an outward peristomal body profile. The primary end point was evaluated by the question “How was the skin barrier’s ability to fit to the body contours in the area around the ostomy?” after each test period. Evaluation of body fit was based on subjective perceptions of body fit of the pouching system without any intervention from study personnel. Participants provided their subjective evaluation on a 5-point Likert scale (very poor, poor, acceptable, good, and very good). The primary objective of this study was supported by additional patient-reported questions related to body fit of the pouching systems to body contours, since no objective measure has been developed to score how well a skin barrier fit to the peristomal area. Participants evaluated the question “Did the skin barrier fold/wrinkle at application?” on a 5-point Likert scale (very much, much, some, a little, and not at all) after each change of skin barrier. Finally, participants evaluated the question “How was the skin barrier’s ability to bend and stretch with the skin when moving the body?” on a 5-point Likert scale (very poor, poor, acceptable, good, and very good) after each test period. Secondary objectives were to compare the effect of flat versus concave skin barriers on leakage, wear time, and QoL.
The degree of leakage and undermining was measured using an objective 32-point leakage scale developed by Coloplast A/S (this tool has not undergone formal validation).21 At each change of skin barrier, the participant placed a petri dish imprinted with the 32-point scale over the used skin barrier and registered the distribution of feces. Each point corresponds to a specific area of the skin barrier covered with feces. The scale ranges from 0 to 32, where zero corresponds to no leakage on the skin barrier and 32 corresponds to the highest degree of leakage covering the entire skin barrier. All investigators and participants were trained to use the tool.
To estimate wear time, participants registered the time from application to removal of each skin barrier used during the entire study period. Participants furthermore registered the reason for change of each skin barrier based upon predefined response options (usual changing pattern, nice with clean product, in preparation of activity, detachment of entire skin barrier, detachment of the outer rim, detachment of the center part, afraid of detachment of skin barrier, area around the ostomy was itching, area around the ostomy was painful, leakage underneath and outside skin barrier, leakage underneath skin barrier, visit from investigator, and other).
QoL was evaluated after each test period using the validated Ostomy-Q tool, designed to measure QoL related to aspects of using an ostomy product.22 The questionnaire contains 23-item questions that have been grouped into 4 domains, concerning discreetness of an ostomy product, comfort related to wearing an ostomy product, confidence with an ostomy product, and how a product impacts social life and relationships. The discreetness, comfort, and confidence domains have scores ranging from 0 to 24, while the social life domain has a score ranging from 0 to 20. The scores of the domains can be summated into a total score ranging from 0 to 92. Higher scores correspond to better QoL. In the validation of the Ostomy-Q tool, the following intraclass correlation coefficients (ICC) for test–retest reliability were reported: discreetness (ICC: 0.751), comfort (ICC: 0.761), confidence (ICC: 0.830), social life (ICC: 0.741), and total (ICC: 0.909). End points related to use of accessories, feeling of security, comfort of product, and preference are presented as Supplemental Digital Content: Appendix: Comfort, Security, Preference (https://links.lww.com/JWOCN/A115).
Study ProceduresDuring the trial, participants used a concave two-piece pouching system (SenSura Mio Concave, termed SenSura Mio Convex Flip in the United States, Italy, Sweden and the Netherlands Coloplast A/S, Humlebæk, Denmark) and a two-piece flat pouching system (Comparator). Comparator pouching systems were differentiated for people with an ileostomy (FlexWear skin barrier; Hollister Incorporated, Libertyville, IL, USA) or a colostomy (SoftFlex skin barrier; Hollister Incorporated). The concave pouching systems were used with an open maxi size pouch having a mechanical coupling (Coloplast A/S). The flat comparator skin barrier was used together with an open maxi size pouch (Hollister Incorporated). The pouching systems for comparator were chosen to ensure homogeneity in products used and since the comparator products were among the most widely used two-piece flat pouching systems in several European markets. The sponsor (Coloplast A/S) provided both the Concave and Comparator pouching systems for all participants via the investigators to ensure that participants could adhere to their usual changing pattern.
Data were collected during two test periods of 21 ± 3 days each. Participants were randomly allocated to one of the products for the first test period before crossing over to the opposite treatment in the second test period (Figure 1A and B).
Written informed consent was obtained prior to entering the study. Participants were then randomized into one of 2 test sequences using a 1:1 group allocation ratio, via 2 centralized randomization lists generated using SAS (version 9.2) depending on whether the participant had an ileostomy or a colostomy. Patient demographics and pertinent clinical data were recorded at baseline (V1) by study investigators using a questionnaire specifically developed for the study. This questionnaire was used to document date of birth, sex, height, weight, duration of living with an ostomy, type of ostomy, reason for stoma creation, width of the outward area/bulge (in cm), height of the outward area/bulge (in cm), current ostomy pouching system, and QoL (scores from the Ostomy-Q). After the first study period, participants had a second visit with investigators (V2, cross-over), where the investigator assessed well-being and compliance of the participants and checked that the participants had filled out the patient-reported part of the case report form prior to the visit (see section Outcome Measures and Instruments).
After the second study period, participants completed a third visit with investigators (V3, termination). During this visit, the investigator assessed the well-being and compliance of the participants and checked that the participants had filled out the patient-reported part of the case report form prior to the visit (see section Outcome Measures and Instruments). Participants received a small gift voucher for participation in the study.
Study investigators received training in the procedure for reporting adverse events from the sponsor. During the investigation, all participants were asked about their health and problems, including anticipated adverse events related to peristomal skin irritation, mechanical trauma, and allergic reactions, by the investigator at every visit. Participants were also encouraged to contact the investigator in case of adverse events.
Sample Size and Data AnalysisBased on data from an exploratory clinical trial (NCT01995357), it was assumed that the likelihood of participants rating body fit of Comparator as being (“very poor + poor,” “acceptable,” “good,” and “very good”) would be (5%, 36%, 36%, and 23%) and that the corresponding distribution for the concave skin barrier would be approximately (1%, 19%, 35%, and 45%). Further, it was assumed that body fit observations would be correlated within subjects with a correlation equal to 0.5. To ensure a power above 85% to demonstrate improved body fit of concave skin barrier compared with Comparator and assuming a dropout of 20%, then 54 participants needed to be enrolled in the study.
Statistical analyses were performed using Proc Glimmix SAS version 9.2 (Cary, NC) and were performed according to the approved statistical analysis plan. The intention-to-treat (ITT) population constituted all randomized subjects with valid informed consent who had been exposed to at least one of the two test products and had reported on at least one end point (Full Analysis Set). The safety population constituted all subjects who had given informed consent and had been exposed to at least one product. All statistical analyses were based on the ITT population, whereas adverse events and device deficiency data were based on the safety population.
The primary end point was the ordinal end point body fit, which was analyzed using a proportional odds model with subjects included as a random component. Product (concave and the flat comparator), type of ostomy (ileostomy and colostomy), and test period (period 1 and period 2) were included as fixed effects. The categories “poor” and “very poor” were collapsed in the statistical analysis. From this model, the odds ratio between concave and comparator was estimated together with the corresponding 95% confidence interval. A test of no difference (odds ratio = 1) against the alternative of an odds ratio different from 1 was performed. Secondary ordinal end points were analyzed like the primary end point, except that no categories were collapsed in these analyses.
The degree of leakage and wear time outcomes were analyzed using a mixed repeated measures model with individual skin barrier observations as the observational unit. The model considered that observations corresponding to different subjects were independent, whereas observations corresponding to the same subject were correlated. The correlation between observations corresponding to the same product was allowed to be larger than observations corresponding to different products. Ostomy-Q scores were analyzed using a linear mixed model with subjects included as a random component. Ostomy-Q scores assessed at inclusion was included as a covariate. In both models, product (concave and the flat comparator), type of ostomy (ileostomy and colostomy), and test period (period 1 and period 2) were included as fixed effects. From these models, the difference in degree of leakage, wear time, or Ostomy-Q scores between concave and comparator were estimated together with the corresponding 95% confidence interval. A test of no difference (H0 = 0) was performed against the alternative (Ha ≠ 0).
RESULTSFifty-three participants were enrolled in the study, and all were randomized to a treatment sequence: comparator switching over to concave or vice-versa (Figure 1B). One participant was a screening failure and was not exposed to any of the test products (safety population, n = 52). Four participants discontinued participation in the study (Figure 1B). Three participants discontinued study participation while using the concave skin barrier in the first test period, and one discontinued while using comparator in the first test period. None were omitted from the ITT population, and data from the ITT population (n = 52) were included in the final analyses.
The average age of participants was 70.9 years (SD = 9.5, range 50-91), and 79% were male (Table 1). Thirty-seven percent had an ileostomy and 63% a colostomy. Ostomies were created due to cancer (50%), ulcerative colitis (21%), or Crohn’s disease (8%), while the remaining participants underwent ostomy surgery due to other causes (Table 1). Participants had lived with an ostomy for an average of 8.4 years (SD = 9.4, range 1-55) prior to study participation. The mean area of the outward peristomal area was 12.5 cm (SD = 4.6; range 6.0-30.0 cm) in diameter and 5.9 cm (SD = 3.6; range 2.0-20.0 cm) in height. All participants used flat two-piece pouching systems before study enrollment; multiple brands were used prior to study enrollment.
TABLE 1. - Baseline Characteristics of Intention-to-Treat Population ITT population, n = 52 Age in years, mean (SD; range) 70.9 (9.5; 50-91) Sex; females/males, n (%) 11 (21.2%)/41 (78.8%) BMI in kg/m2, mean (SD; range) 27.7 (4.2; 16-36) Type of ostomy; ileostomy/colostomy, n (%) 19 (36.5%)/33 (63.5%) Time since surgery (years), mean (SD; range) 8.4 (9.4; 1-55) Reason for ostomy surgery, n (%) Ulcerative colitis 11 (21.2%) Cancer 26 (50.0%) Crohn’s disease 4 (7.7%) Other 11 (21.2%) Outward area, n Diameter in cm, mean (SD; range) 12.5 (4.6; 6.0-30.0) Height in cm, mean (SD; range) 5.9 (3.6; 2.0-20.0)The primary end point was the skin barrier’s ability to fit body contours in the area around the ostomy. Body fit was rated significantly better for concave than for comparator (P < .001). Eighty-six percent of the participants rated the concave skin barrier to be “good” or “very good” at fitting body contours in the area around the ostomy, compared to 38% of the participants with comparator (Figure 2).
 Figure 2.:
Figure 2.:
Subjective evaluation of body fit of concave and flat comparator skin barriers. Q: How was the skin barrier’s ability to fit to the body contours in the area around the ostomy?
To support the primary objective of this study, participants answered two additional questions related to fit of the skin barrier to the peristomal area. When asked about whether the skin barrier folded or wrinkled at application, 97% of the participants stated that the concave skin barrier did “not at all” fold/wrinkle or only folded/wrinkled “a little”, compared to 69% for the comparator (Figure 3A). The adhesive of the concave skin barrier was also rated significantly better at bending and stretching with the skin compared to the adhesive of comparator (P < .001). Eighty-four percent of the participants stated that the ability of the adhesive to bend and stretch with the skin for concave skin barrier was “good” or “very Good”, compared with 47% of the participants stating this when using comparator (Figure 3B).
 Figure 3.:
Figure 3.:
Application of skin barriers and ability to bend and stretch with the skin. (A) Proportion of skin barriers folding/wrinkling at application of each barrier (concave: n = 421 skin barriers; comparator: n = 409 skin barriers). (B) Ability of the skin barrier to bend and stretch with skin when moving the body. (A) Q: Did the skin barrier fold/wrinkle at application? (B) Q: How was the skin barrier’s ability to bend and stretch with your skin when moving the body?
The degree of leakage underneath the skin barrier was significantly lower for the concave versus the comparator skin barrier (LS mean 8.15 vs. 9.99; LS mean difference = −1.84, 95% CI −3.31 to −0.37; P = .016; Figure 4A). Leakage was observed underneath 87.8% of the comparator skin barriers upon change compared with 74.1% of the concave skin barriers (P = .007; Figure 4B). Furthermore, participants recorded if leakage had progressed outside the skin barrier, which was the case for 26.8% of the comparator skin barriers compared with 13.0% of the concave skin barriers (Figure 4B).
 Figure 4.:
Figure 4.:
Degree of leakage when using concave and comparator skin barriers. (A) Leakage underneath skin barrier assessed on a 32-point scale. 0 = no leakage; 32 = leakage on whole skin barrier. (B) Proportion of skin barriers with leakage underneath or outside the barrier. P < .05 (★), P < .01 (★★), and P < .001 (★★★).
The mean wear time for concave versus comparator skin barrier was 51.4 versus 47.4 hours (LS mean difference = 4.0, 95% CI [−0.636; 8.694], P = .089). Participants were asked to record the main reason for pouching changes that incorporated the skin barrier (Table 2). A higher proportion of the concave skin barriers (55.7%, n = 236) were changed according to the participants’ usual changing pattern compared with the comparator (38.5%, n = 158). Findings indicate that comparator skin barriers were changed more often due to leakage underneath and outside the skin barrier, fear of skin barrier detachment, itching, and pain around the ostomy as compared with the concave skin barriers.
TABLE 2. - Reason(s) for Change of Skin Barrier Category Comparator (n = 410) Concave (n = 424) Usual changing pattern 158 (38.5%) 236 (55.7%) Nice with clean product 24 (5.9%) 51 (12.0%) In preparation of activity 14 (3.4%) 19 (4.5%) Detachment of entire skin barrier 12 (2.9%) 11 (2.6%) Detachment of the outer rim 28 (6.8%) 28 (6.6%) Detachment of the center part 39 (9.5%) 17 (4.0%) Afraid of detachment of skin barrier 41 (10.0%) 8 (1.9%) Area around the ostomy was itching 48 (11.7%) 27 (6.4%) Area around the ostomy was painful 36 (8.8%) 9 (2.1%) Leakage underneath and outside ȃskin barrier 87 (21.2%) 41 (9.7%) Leakage underneath skin barrier 106 (25.9%) 89 (21.0%) Visit from investigator 28 (6.8%) 26 (6.1%) Other 16 (3.9%) 24 (5.7%)QoL related to aspects of using an ostomy product was assessed using the validated Ostomy-Q tool.22 When using concave skin barriers, participants had a significantly higher total score than with comparator barriers (LS mean 67.2 vs. 53.0; LS mean difference = 14.3; 95% CI 9.4 to 19.2; P < .001, Figure 5). All four domains of the Ostomy-Q tool (confidence, comfort, discreetness, and social life) contributed to the increase observed in total score, and all four domains were significantly higher with concave versus comparator skin barriers.
 Figure 5.: Quality of life related to aspects of using an ostomy product. QoL was assessed using the validated Ostomy-Q tool containing 23 questions grouped in four domains.22 The range of each domain score is highlighted in the figure legend. Higher scores reflect improved QoL. PPP
Figure 5.: Quality of life related to aspects of using an ostomy product. QoL was assessed using the validated Ostomy-Q tool containing 23 questions grouped in four domains.22 The range of each domain score is highlighted in the figure legend. Higher scores reflect improved QoL. PPP
Twenty-one participants (40% of safety population) experienced one or more adverse events during the investigation. In total, n = 41 adverse events were recorded. Of these, 3 were serious adverse events (n = 1 with lung infection [recovered], n = 1 with compartment syndrome in the left lower leg [recovered], and n = 1 with renal failure [fatal]). All serious adverse events had their onset when participants used comparator; none were deemed to be “related” to study participation.
Thirty-eight adverse events occurred that were deemed nonserious. Adverse events that were classified as “unlikely related,” “possibly related,” “probably related,” and “definitely related” to concave or comparator were treated as “related.” Of the nonserious adverse events, 36 were related to the test products and 2 were not related to the test products. Fifteen of the nonserious adverse events were related to use of the concave skin barrier and 21 were related to use of comparator skin barrier. Most (n = 35) were PSCs with descriptions of skin damage, redness, pain, and/or itching. One participant experienced 2 events of ostomy bleeding that were categorized as “unlikely related” to the use of the comparator skin barrier. One participant was diagnosed with influenza while using concave skin barrier; this adverse event was registered as “unlikely related” to use of the product.
Two device deficiencies were reported during the study. One occurred in the comparator group; it was characterized as lack of adhesion when the skin barrier was applied to the peristomal skin. An unresolved device deficiency, leakage in a concave skin barrier was attributed to the coupling mechanism between the skin barrier and pouch. Neither device deficiencies were linked to serious adverse event and no corrective actions were required to be taken, except that participants changed the respective pouching systems to a new one.
DISCUSSIONThis randomized, controlled, cross-over clinical trial compared multiple outcomes among participants with an ostomy and outward peristomal body profile using a concave versus flat skin barrier. The primary outcome of the study was that the concave skin barrier provided a better fit to body contours than a comparator (flat) skin barrier. Participants reported that the concave skin barrier had a reduced risk of folding or wrinkling upon application of the skin barrier than the comparator. They indicated that the concave skin barrier was better able to bend and stretch with the skin when moving the body than the comparator. We hypothesize that the improved body fit of concave on individuals with an outward peristomal body profile likely provided a more secure seal between barrier and skin, leading to a lower degree of leakage seeping underneath the skin barrier and fewer episodes of leakage progressing outside the skin barrier. Despite improvements to leakage control with the concave vs comparator skin barriers, no significant difference in wear time between the two skin barrier shapes occurred. The reduction in leakage incidents when using the concave skin barrier compared with flat skin barriers was associated with a concomitant improvement in QoL. The improvement in the total Ostomy-Q score between concave and comparator (LS mean difference = 14.3) was higher than the minimal important difference (MID) for the total Ostomy-Q score of 8.75 (average of three MID estimation methods, assuming 25% reduction in leakage incidents onto clothes22), thus providing a meaningful improvement in QoL related to aspects of using an ostomy product. The improvements in scores between concave and comparator were also higher than the respective MIDs for the “discreetness,” “comfort,” and “confidence” domains but not for the “social life” domain (MID values: discreetness = 2.40, comfort = 3.05, confidence = 3.25, and social life = 2.43). Considered collectively, these results indicate that participants with an outward peristomal body profile using the concave skin barrier felt less worried about leakage and PSCs and had a higher confidence to spend a night away from home and to participate in physical activities.22
The shape of the concave skin barrier differentiates from the numerous skin barriers available in the market featuring a convex design. Convex skin barriers press into the peristomal skin to increase stomal protrusion and are intended to help individuals with inward peristomal body profiles and/or retracted stomas.8 Studies have shown that use of convex skin barriers can help people with such challenging peristomal areas and/or ostomies to obtain a better fit between skin and barrier and hence reduce the risk of leakage.21,23,24
For convex skin barriers, the depth of convexity can vary from shallow/light to deep and the area of the raised part of the skin barrier varies between brands. Since convex skin barriers press into the peristomal skin, they are used with caution in the presence of peristomal skin ulcers. Furthermore, it has been reported that patients with parastomal hernia should be assessed carefully before use of convex skin barriers, as the peristomal skin may already be stretched and at risk of breakdown if additional pressure is applied to the skin.25 The outcomes of this trial suggest that people with an outward peristomal body profile, such as those with parastomal hernias, may benefit from using skin barriers with a concave shape that better fit curved body contours and concomitantly reduces the risk of leakage. The abdominal topography around the ostomy varies considerably between individuals and may be accompanied with creases and folds that can make it difficult to secure a tight seal between skin and barrier. Proper assessment of the peristomal body profile is important for the selection of the most suitable pouching system for the individual needs.13,16 For example, the Peristomal Body Profile Assessment Tool is a multistep guide helping with the selection of pouching systems that in part is based on patient’s abdominal topography. When a group of nurses used this tool for selection of pouching systems, patients experienced significantly fewer leakage incidents and reported concomitant improvements in QoL.16
Leakage can be debilitating to experience for the individual as it may lead to embarrassing situations. Leakage has been associated with reductions in QoL,2,26 lower health states as determined in a time trade-off study,19 and an increased risk of social isolation.2 Use of a concave skin barrier was related to significantly fewer leakage episodes and higher ostomy-specific QoL in the present study and supports similar correlations between leakage reduction and QoL improvements reported by others.10,11,16,21,23 Not only does leakage have a significant physical and psychological impact on patients’ lives, it can also be costly to the health care system to not address leakage-related issues that people with an ostomy struggle with.27 People troubled with leakage of stomal effluent increase their use of pouching systems, accessory products, and more often consult with health professionals to mitigate the risk of future leakage incidents.2,27
Strengths and LimitationsThe results of this study should be interpreted considering strengths and limitations of the study design. A strength of this study is the randomized, cross-over design that may limit bias based on group allocation and sequencing of wearing a pouching system with a flat versus concave skin barrier. Moreover, the cross-over design allowed participants to serve as their own control. A limitation of the study design is that participants were not blinded due to the visual differences in the shapes of the test products. No attempts were made to blind the products. Absence of blinding could potentially bias the subjective evaluation of the test products, since 90% of participants used pouching systems from Coloplast at baseline. Finally, there was an overrepresentation of males in the study (79%), being higher than the reported distribution of males (57%) and females (43%) for people with an outward peristomal body profile among individuals living with an ostomy.28
CONCLUSIONFindings of this trial indicate that a skin barrier with a concave profile was perceived to provide a better fit to the peristomal area of people with an outward peristomal body profile. Specifically, the concave skin barrier reduced the risk of the skin barrier to fold or wrinkle upon application compared with a flat skin barrier. The concave skin barrier also reduced leakage, and participants reported concomitant improvements to QoL related to using an ostomy product. No significant difference in wear time between skin barrier shapes was reported. We recommend WOC nurses to consider a skin barrier with a concave feature for patients with an outward peristomal body profile and difficulty with obtaining a secure seal when using flat skin barriers.
ACKNOWLEDGMENTThe authors wish to express their sincere gratitude to all patients who participated in the study and to all health professionals involved in the study.
REFERENCES 1. Richbourg L, Thorpe JM, Rapp CG. Difficulties experienced by the ostomate after hospital discharge. J Wound Ostomy Continence Nurs. 2007;34(1):70–79. doi:10.1097/00152192-200701000-00011. 2. Jeppesen PB, Vestergaard M, Boisen EB, Ajslev TA. Impact of stoma leakage in everyday life: data from the Ostomy Life Study 2019. Br J Nurs. 2022;31:S48–S58. doi:10.12968/bjon.2022.31.6.S48. 3. Goldstine J, van Hees R, van de Vorst D, Skountrianos G, Nichols T. Factors influencing health-related quality of life of those in the Netherlands living with an ostomy. Br J Nurs. 2019;28(22):S10–S17. doi:10.12968/bjon.2019.28.22.S10. 4. Murken DR, Bleier JI. Ostomy-related complications. Clin Colon Rectal Surg. 2019;32(3):176–182. doi:10.1055/s-0038-1676995. 5. Burch J. Exploring the conditions leading to stoma-forming surgery. Br J Nurs. 2005;14(2):94–98. doi:10.12968/bjon.2005.14.2.17438. 6. Gill-Thompson NN, Erwin-Toth P, Krasner DL. Enterostomal Therapy Nursing: Growth & Evolution of a Nursing Specialty Worldwide. ISBN 0-9613805-9-4. 2020. 7. Virgin-Elliston T, Nonboe P, Boisen EB, Koblauch H. Evaluating the performance and perception of a stoma bag full-circle filter in people with a colostomy or an ileostomy—two randomized crossover trials. Healthcare. 2023;11(3):369. doi:10.3390/healthcare11030369 8. Harris G. Stoma care appliances: an overview. Gastrointest Nurs. 2021;19(Sup9):S14–S19. doi:10.12968/gasn.2021.19.Sup9.S14. 9. Boyles A. Keeping up to date with stoma care accessories: enabling informed choice. Gastrointest Nurs. 2010;8(6):24–38. doi:10.12968/gasn.2010.8.6.49020. 10. Brady RRW, Fellows J, Meisner S, Olsen JK, Vestergaard M, Ajslev TA. A pilot study of a digital ostomy leakage notification system: impact on worry and quality of life. Br J Nurs. 2023;32:S4–S12. doi:10.12968/bjon.2023.32.6.S4. 11. Ambe PC, Brunckhorst E, Hansen HD, Gotfredsen JL, Vestergaard M, Ajslev TA. Effect of a Novel Digital Leakage Notification System (Heylo) for Ostomy Care on Quality of Life and Burden of Living With an Intestinal Ostomy: the ASSISTER Trial, A Randomized Controlled Cross-Over Trial. Mayo Clin Proc. 2023;1:438–449. 12. Colwell JC, Bain KA, Hansen AS, Droste W, Vendelbo G, James-Reid S. International consensus results: development of practice guidelines for assessment of peristomal body and stoma profiles, patient engagement, and patient follow-up. J Wound Ostomy Continence Nurs. 2019;46(6):497–504. doi:10.1097/WON.0000000000000599. 13. Colwell JC. The importance of pouching system barrier fit. WCET. 2022;42:S5–S7. 14. Burch J. Stoma product selection: an update. Br J Community Nurs. 2023;28(4):188–192. doi:10.12968/bjcn.2023.28.4.188. 15. Martins L, Andersen BD, Colwell J, et al. Challenges faced by people with a stoma: peristomal body profile risk factors and leakage. Br J Nurs. 2022;31(7):376–385.doi:10.12968/bjon.2022.31.7.376. 16. Vendelbo G, Carlsson E, Tøndel LT, et al. Using peristomal body profile assessment to improve leakage-related quality of life for individuals with an ostomy. Br J Community Nurs. 2023;32(4):173–181.doi:10.12968/bjon.2023.32.4.173. 17. Down G, Vestergaard M, Ajslev TA, Boisen EB, Nielsen LF. Perception of leakage: data from the Ostomy Life Study 2019. Br J Nurs. 2021;30(22):S4–S12. doi:10.12968/bjon.2021.30.22.S4. 18. Voegeli D, Karlsmark T, Eddes EH, et al. Factors influencing the incidence of peristomal skin complications: evidence from a multinational survey on living with a stoma. Gastrointest Nurs. 2020;18(Sup4):S31–S38.doi:10.12968/gasn.2020.18.Sup4.S31. 19. Rolls N, Yssing C, Bøgelund M, Håkan-Bloch J, de Fries Jensen L. Utilities associated with stoma-related complications: peristomal skin complications and leakages. J Med Econ. 2022;25(1):1005–1014. doi:10.1080/13696998.2022.2101776. 20. Dwan K, Li T, Altman DG, Elbourne D. CONSORT 2010 statement: extension to randomised crossover trials. BMJ. 2019;366. doi:10.1136/bmj.l4378. 21. Kruse TM, Størling ZM. Considering the benefits of a new stoma appliance: a clinical trial. Br J Community Nurs. 2015;24(Sup22):S12–S18. doi:10.12968/bjon.2015.24.Sup22.S12. 22. Nafees B, Rasmussen M, Lloyd A. The Ostomy-Q: development and psychometric validation of an instrument to evaluate outcomes associated with ostomy appliances. Ostomy Wound Manage. 2017;63:12–22. 23. Walker H, Hopkins G, Waller M, Storling ZM. Raising the bar: new flexible convex ostomy appliance-a randomised controlled trial. WCET. 2016;36:S6–S11. 24. Rat P, Robert N, Fernandes I, Edmond D, Mauvais F. Evaluation of a one-piece soft convex ostomy appliance: a prospective, multicentre, open-label pilot study. Br J Nurs. 2018;27(16):S20–S28. doi:10.12968/bjon.2018.27.16.S20. 25. Perrin A, White M, Burch J. Convexity in stoma care: developing a new ASCN UK guideline on the appropriate use of convex products. Gastrointest Nurs. 2023;21(1):18–25. doi:10.12968/gasn.2023.21.1.18. 26. Hedegaard CJ, Ajslev TA, Zeeberg R, Hansen AS. Leakage and peristomal skin complications influences user comfort and confidence and are associated with reduced quality of life in people with a stoma. WCET. 2020;40:23–29. 27. de Fries Jensen L, Rolls N, Russell-Roberts P, Vestergaard M, Jensen ML, Boisen EB. Leakage of stomal effluent outside the baseplate leads to rise in product usage and health professional interactions. Br J Nurs. 2023;32(1):8–19. doi:10.12968/bjon.2023.32.1.8.
Comments (0)