
Remember me



Intraluminal tracheobronchial stents are used to treat airway obstruction because of both malignant and benign obstructive diseases of the trachea or bronchi.1,2 In conjunction with the standard management for the underlying primary disease, stents relieve dyspnea and improve overall functional status.3 Stents come in various shapes and sizes and are made of various biocompatible materials, each with unique insertion techniques.4,5 However, the search for an ideal stent is still ongoing.6 Stents are foreign objects and are not devoid of complications.5 These include malposition, stent fractures, stent migration, airway perforation, excessive granulation-tissue formation, hemorrhage, bacterial colonization resulting in stent-associated infections, stent obstructions because of tumor, granulation tissue, and/or mucostasis.5,7
These complications may be life-threatening and hence may justify surveillance bronchoscopy at an interval of 4–6 weeks after placement.7 Studies report stent migration rates between 20% and 50%, whereas few studies report a much lower rate (<5%).5,8,9 A mismatch between the size of the airway and the stent diameter is believed to be one of the factors resulting in stent migration.10 In this article, we present a unique case wherein the displacement of a stent leads to its inadvertent ingestion during a coughing episode. This case represents only the second reported instance worldwide of swallowing a tracheal stent during a coughing episode.
CASE REPORTA 48-year-old man with a medical history notable for hypertension, non–insulin-dependent diabetes mellitus, and morbid obesity (body mass index = 47 kg/m2) was diagnosed with coronavirus disease 2019 pneumonia. The patient had prolonged hospitalization for 6 months, during which the patient required mechanical ventilation and venovenous extracorporeal membrane oxygenation.
The hospital course was complicated by severe tracheomalacia and tracheal stenosis, requiring tracheal resection and reconstruction. After the failure of the initial reconstruction, a tracheal stent was placed with venovenous extracorporeal membrane oxygenation support. Follow-up bronchoscopy revealed stent fractures, necessitating temporization with balloon dilation and the placement of a Y-shaped silicone stent to cover the AERO stent (Merit Medical Systems, Inc., South Jordan, UT) fracture.
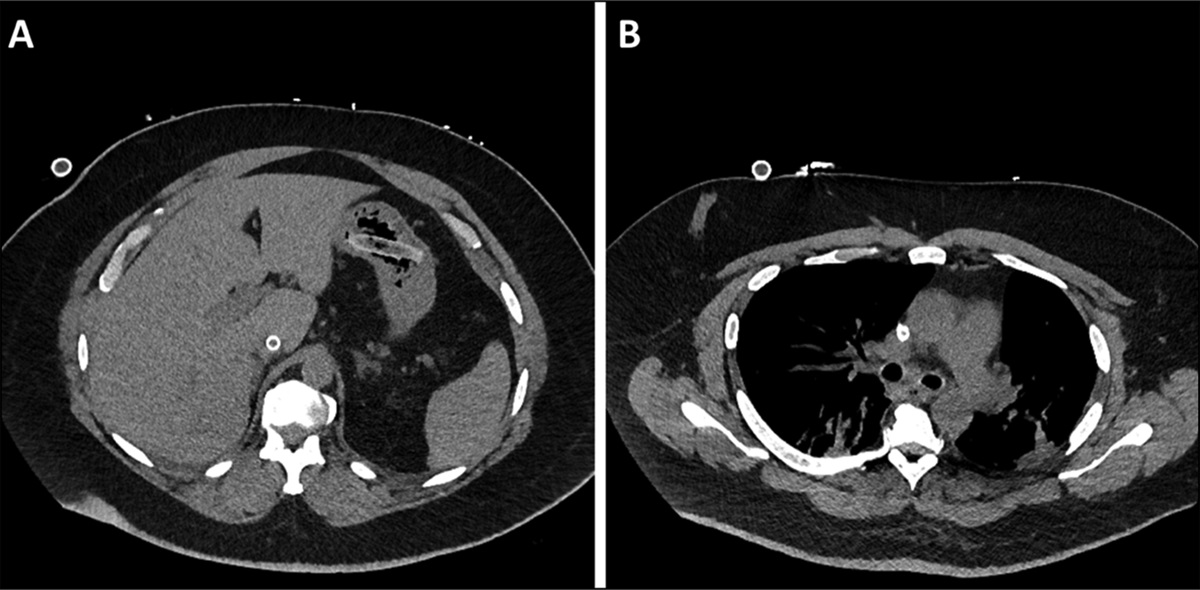
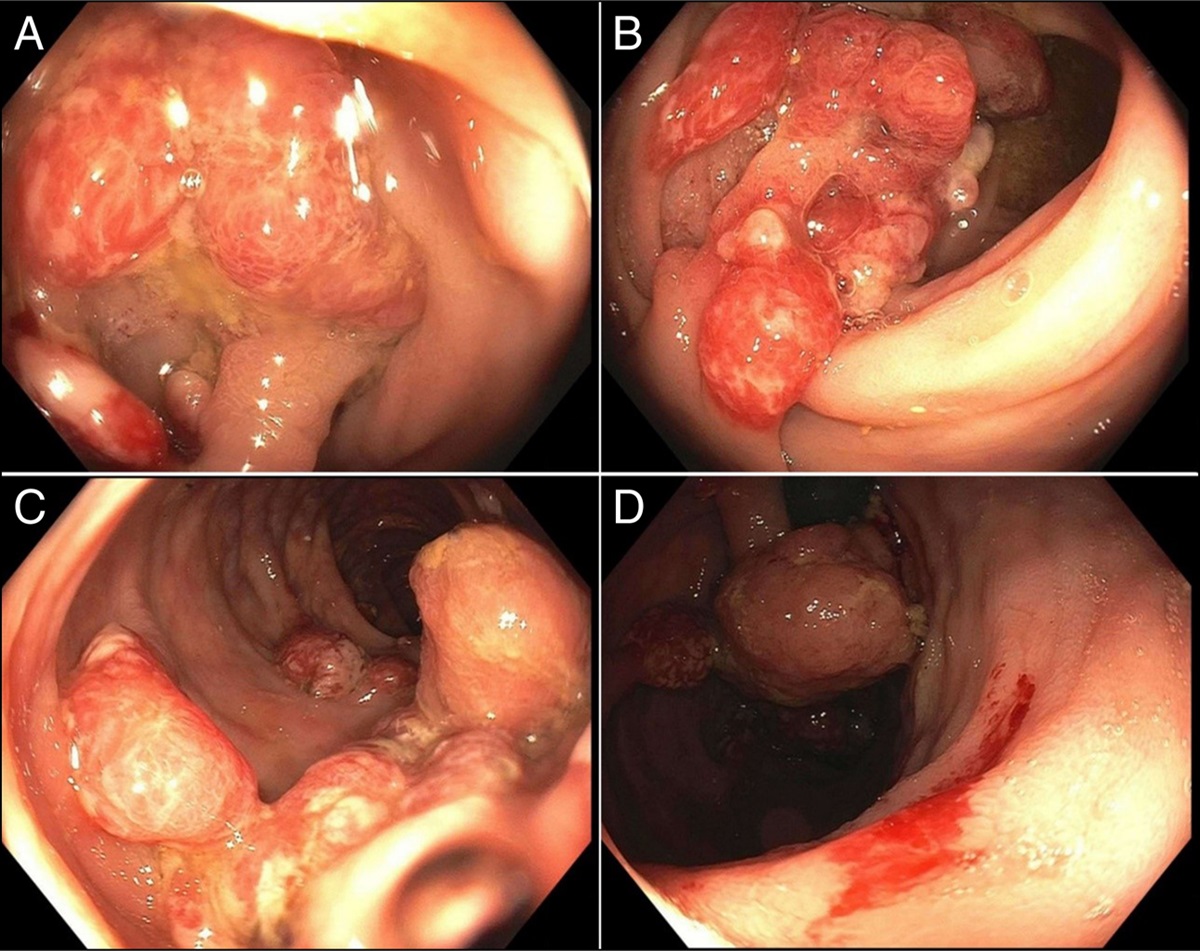
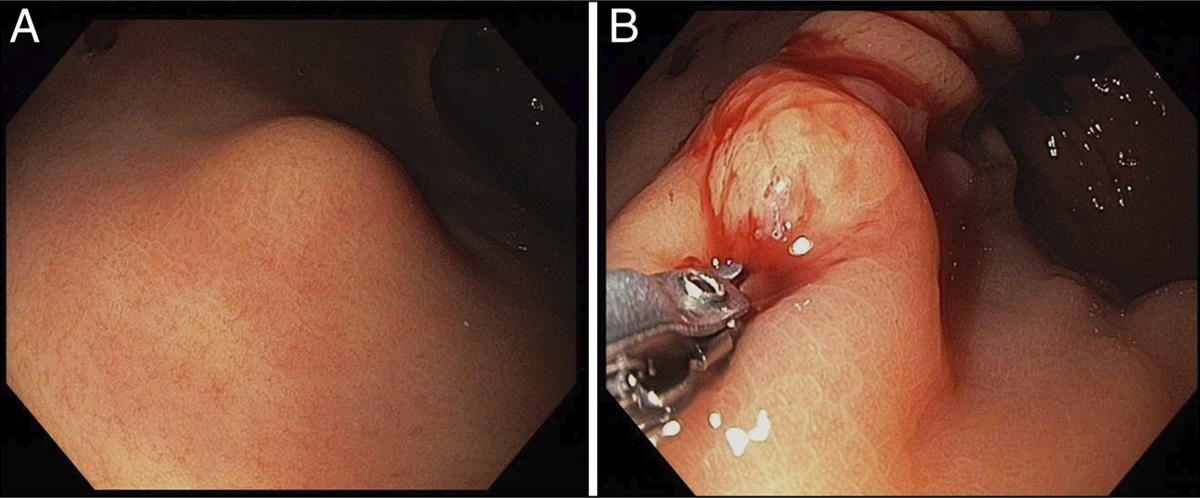
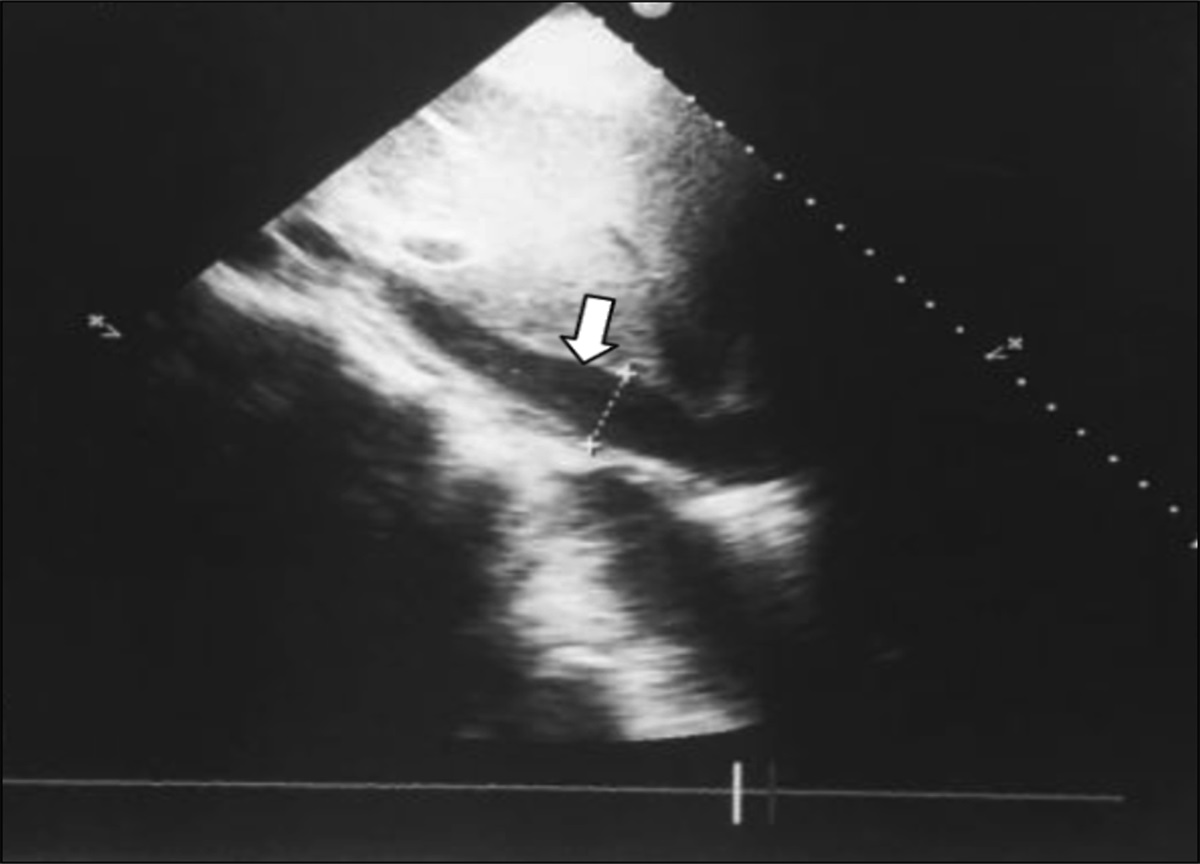
On admission to the hospital for stent exchange, rigid bronchoscopy demonstrated the absence of a tracheal stent. The patient reported experiencing a severe episode of coughing and choking before the bronchoscopy. However, he denies any difficulty in swallowing; there were concerns about the possibility of coughing up and swallowing the stent. An abdominal and pelvic computed tomography scan without contrast revealed the presumed ingested tracheal stent within the gastric fundus without evidence of perforation, as shown in Figure 1. In response, emergent upper gastrointestinal endoscopy was performed, with retrieval of the intact Y-shaped silicone stent from the gastric fundus using a Roth Net device (US Endoscopy [a subsidiary of Steris Corporation], Mentor, OH) (Figure 2). The patient underwent a successful replacement of a Y-tracheal stent the following day and was subsequently discharged from the hospital after recovery. There was no evidence of tracheoesophageal fistula based on computed tomography scan, bronchoscopy, and endoscopy.
 Figure 1.:
Figure 1.: Abdominal CT without contrast shows the presence of a stent in the stomach (A); chest CT without contrast shows an absence of a stent (B). CT, contrast tomography.
 Figure 2.:
Figure 2.: Y-shaped silicone stent in the gastric fundus.
DISCUSSIONThis case report outlines an uncommon and captivating occurrence involving the dislodgment of a tracheal stent during a coughing spell resulting in ingestion. Stents are broadly classified into 2 groups, including plastic (eg, silicone) and metallic stents (eg, stainless steel). Several complications of tracheal stents have been described (Table 1). The primary complications arising from human errors are typically associated with stent misplacement, incorrect sizing, and overly extended positioning.11 The most frequent complications related to stents include migration, fracture, patient intolerance, and the formation of granulation tissue around the stent.12 In our case, attempts to manage tracheal stenosis through stenting proved unsuccessful. The initial stent experienced a fracture, and during the second attempt, it dislodged and was subsequently swallowed into the stomach.
Table 1. - Types of stents, characteristics, complications, and notable features/innovative features Stent type Characteristics Risk factors Complications Notable features/innovations Plastic Silicone or other polymers Loose placementThe tendency for stents to migrate differs between different stent types.7,13,14 When silicone T-tube stents were modified to a straight tube, the design allowed easier endoscopic insertion, less incidence of secretion plugging, and the added benefit of being more esthetically acceptable to patients since a stoma was no longer needed.15 Silicone stents can be fixed to the airway to reduce the possibility of migration. However, this anchoring option is not feasible for self-expandable metal stents (SEMS) because of their rigid nature and lack of flexibility.16 Other risk factors for stent migration include using a loose stent or stenting a short segment (≤2.5 cm) with smooth mucosa.17,18 Cough is the most common symptom of stent migration.
The ideal stent should (i) be easy to install, (ii) easily retrievable by bronchoscopy, (iii) difficult to dislodge during maneuvers that increase airway pressures, (iv) allow unimpeded mucus clearance, and (v) incite little or no mucosal irritation.15 As of now, the ideal stent has yet to be developed that has all of the desirable qualities. Perhaps, this ultimate combination will never be found, but efforts are ongoing. The newer generation AERO stents have built-in features such as antimigration fins and larger diameters toward the proximal and distal ends.12,19 Our patient initially had an AERO stent placed, which unfortunately got fractured, and the patient had to get a silicone stent as a temporizing measure. The biodegradable stents represent an innovation in the future of stent technology and practices. It is made of degradable polymers such as polydioxanone, and these stents degrade without requiring any extraction. The Food and Drug Administration has not approved the use of biodegradable stents in North America. In addition, no product patents have been filed with the Food and Drug Administration by any stent manufacturers in North America for its experimental use. Thus, biodegradable stents are a novel idea, with much of its ongoing research focused in Europe.20 Migration of SEMS remains a problem. When dislodged, SEMS can be ingested or cause asphyxiation if remains trapped in the hypopharynx.
This case highlights the importance of a multidisciplinary approach to address stent migration, requiring collaboration between pulmonologists and gastroenterologists. By illuminating this rare but life-threatening complication, it enhances gastroenterologists' understanding of tracheal stent-related challenges, enabling them to anticipate and strategize the appropriate course of action.
DISCLOSURESAuthor contributions: F. Vikash: chart review and writing a manuscript draft and revisions. O. Osayande: chart review and manuscript revisions. M. Pang: manuscript critical review and is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Wood DE, Liu YH, Vallières E, Karmy-Jones R, Mulligan MS. Airway stenting for malignant and benign tracheobronchial stenosis. Ann Thorac Surg. 2003;76(1):167–74. discussion 173-4. 2. Sonett JR, Keenan RJ, Ferson PF, Griffith BP, Landreneau RJ. Endobronchial management of benign, malignant, and lung transplantation airway stenoses. Ann Thorac Surg. 1995;59(6):1417–22. 3. Ost DE, Ernst A, Grosu HB, et al. Therapeutic bronchoscopy for malignant central airway obstruction: Success rates and impact on dyspnea and quality of life. Chest. 2015;147(5):1282–98. 4. Lee P, Kupeli E, Mehta AC. Airway stents. Clin Chest Med. 2010;31(1):141–50. 5. Bolliger CT, Sutedja TG, Strausz J, Freitag L. Therapeutic bronchoscopy with immediate effect: Laser, electrocautery, argon plasma coagulation and stents. Eur Respir J. 2006;27(6):1258–71. 6. Hramiec JE, Haasler GB. Tracheal wire stent complications in malacia: Implications of position and design. Ann Thorac Surg. 1997;63(1):209–13. discussion 213. 7. Lee HJ, Labaki W, Yu DH, et al. Airway stent complications: The role of follow-up bronchoscopy as a surveillance method. J Thorac Dis. 2017;9(11):4651–9. 8. Fernandez-Bussy S, Akindipe O, Kulkarni V, Swafford W, Baz M, Jantz MA. Clinical experience with a new removable tracheobronchial stent in the management of airway complications after lung transplantation. J Heart Lung Transpl. 2009;28(7):683–8. 9. Saad CP, Murthy S, Krizmanich G, Mehta AC. Self-expandable metallic airway stents and flexible bronchoscopy: Long-term outcomes analysis. Chest. 2003;124(5):1993–9. 10. Stephens KE Jr, Wood DE. Bronchoscopic management of central airway obstruction. J Thorac Cardiovasc Surg. 2000;119(2):289–96. 11. Pang YK, Liam CK, Leow CH, Shyamala P, Zal AR. Tracheobronchial stenting is safe and effective in relieving upper airway obstruction. Med J Malaysia. 2006;61(2):147–50. 12. Folch E, Keyes C. Airway stents. Ann Cardiothorac Surg. 2018;7(2):273–83. 13. Dooms C, De Keukeleire T, Janssens A, Carron K. Performance of fully covered self-expanding metallic stents in benign airway strictures. Respiration. 2009;77(4):420–6. 14. Chin CS, Litle V, Yun J, Weiser T, Swanson SJ. Airway stents. Ann Thorac Surg. 2008;85(2):S792–6. 15. Mattison LE, Frye MD, Collop NA. Accidental ingestion of a tracheal stent. Chest. 1995;108(3):875–6. 16. Hohenforst-Schmidt W, Linsmeier B, Zarogoulidis P, et al. Transtracheal single-point stent fixation in posttracheotomy tracheomalacia under cone-beam computer tomography guidance by transmural suturing with the Berci needle—A perspective on a new tool to avoid stent migration of Dumon stents. Ther Clin Risk Manag. 2015;11:837–50. 17. Dumon JF. A dedicated tracheobronchial stent. Chest. 1990;97(2):328–32. 18. Bolliger CT, Probst R, Tschopp K, Solèr M, Perruchoud AP. Silicone stents in the management of inoperable tracheobronchial stenoses. Indications and limitations. Chest. 1993;104(6):1653–9. 19. Mehta AC. AERO self-expanding hybrid stent for airway stenosis. Expert Rev Med Devices. 2008;5(5):553–7. 20. Dutau H, Musani AI, Laroumagne S, Darwiche K, Freitag L, Astoul P. Biodegradable airway stents–bench to bedside: A comprehensive review. Respiration. 2015;90(6):512–21.
Comments (0)