
Remember me




Serious consequences often occur in invasive infections caused by multidrug resistant Gram-positive bacteria, especially methicillin-resistant Staphylococcus aureus (MRSA). Although many therapeutic options are available for the treatment of systemic Gram-positive bacterial infections in children (eg, vancomycin, clindamycin, trimethoprim-sulfamethoxazole, linezolid, daptomycin, ceftaroline, and dalbavancin), several have notable drawbacks, particularly for the treatment of central nervous system (CNS) infections. For example, although vancomycin was recommended as the first-line option for patients with invasive MRSA infections given limited options a decade ago,1 its use in children has been associated with a variety of concerns, primarily renal and ototoxicity, particularly at dosages required for CNS infections. Other concerns include the emergence of heteroresistant MRSA that demonstrates decreased susceptibility to vancomycin, as well as concerns for efficacy in invasive MRSA infection compared with other MRSA-active antibiotics.2
Ceftaroline fosamil (Teflaro [AbbVie, USA]/Zinforo [Pfizer, Ireland), hereafter referred to as ceftaroline, is a US Food and Drug Administration (FDA)– and European Medicines Agency (EMA)–approved fifth-generation cephalosporin. The indications for ceftaroline listed in the FDA-approved label are treatment of acute bacterial skin and skin structure infections in adult and pediatric patients down to 34 weeks' gestational age and 12 days' postnatal age, and for community-acquired bacterial pneumonia in adult and pediatric patients 2 months of age and older.3 According to the EMA-approved summary of product characteristics for ceftaroline, it is indicated for the treatment of complicated skin and soft tissue infections and community-acquired pneumonia in neonates, infants, children, adolescents, and adults.4 This antibiotic shows high levels of in vitro activity against common clinical isolates encountered in children, including MRSA and methicillin-resistant Staphylococcus epidermidis (MRSE).5–7 Additionally, ceftaroline has been used by clinicians to treat infections not prospectively studied by the marketing authorization holder and presented to the FDA for approval, including osteomyelitis, endocarditis, bacteremia, ventriculoperitoneal shunt infection, and epidural abscesses (Bradley, personal communication).8–13 Pharmacokinetic (PK) data regarding ceftaroline penetration into cerebrospinal fluid (CSF), from animal model and preliminary experiences in adults, showed that the actual drug dosing regimens can provide CSF unbound, free drug concentrations at least 50% of the time above the minimum inhibitory concentration (MIC) of the dosing interval and resulted in successful clinical outcome with no identified adverse outcomes.11,14–17 Protein binding of ceftaroline is approximately 20%.3,4
Bacterial infections in the CNS may arise from primary bacteremia, including meningitis and brain abscess, as well as CNS infections that represent extensions of infections in other tissue sites such as maxillary, ethmoid, or frontal sinusitis causing epidural abscess and subdural empyema, or spinal epidural abscesses arising from intervertebral disc space infections or vertebral osteomyelitis. In addition, CNS infections associated with neurosurgical intervention18 can arise from implanted foreign materials, including ventricular shunt infections (ventriculoperitoneal [VP], ventriculoatrial, external ventricular drain [EVD]) and baclofen intrathecal pump infections.19–21
At present, ceftaroline is not approved for the treatment of CNS infections; however, there is a significant level of interest in assessing the safety and efficacy of ceftaroline for such infections primarily caused by MRSA and methicillin-resistant coagulase negative staphylocci, compared with vancomycin, which has been the standard of care. A recent publication by Dalla Costa et al22 based on CSF concentrations of ceftaroline in neurosurgical patients provides support for use of ceftaroline in CNS infections. Herein, we describe what is known about the PK and pharmacodynamic (PD) properties of ceftaroline in children, including limited published data on treatment of CNS infections in adults, and discuss the need for prospective evaluation for potential use as a treatment for CNS infections in children.
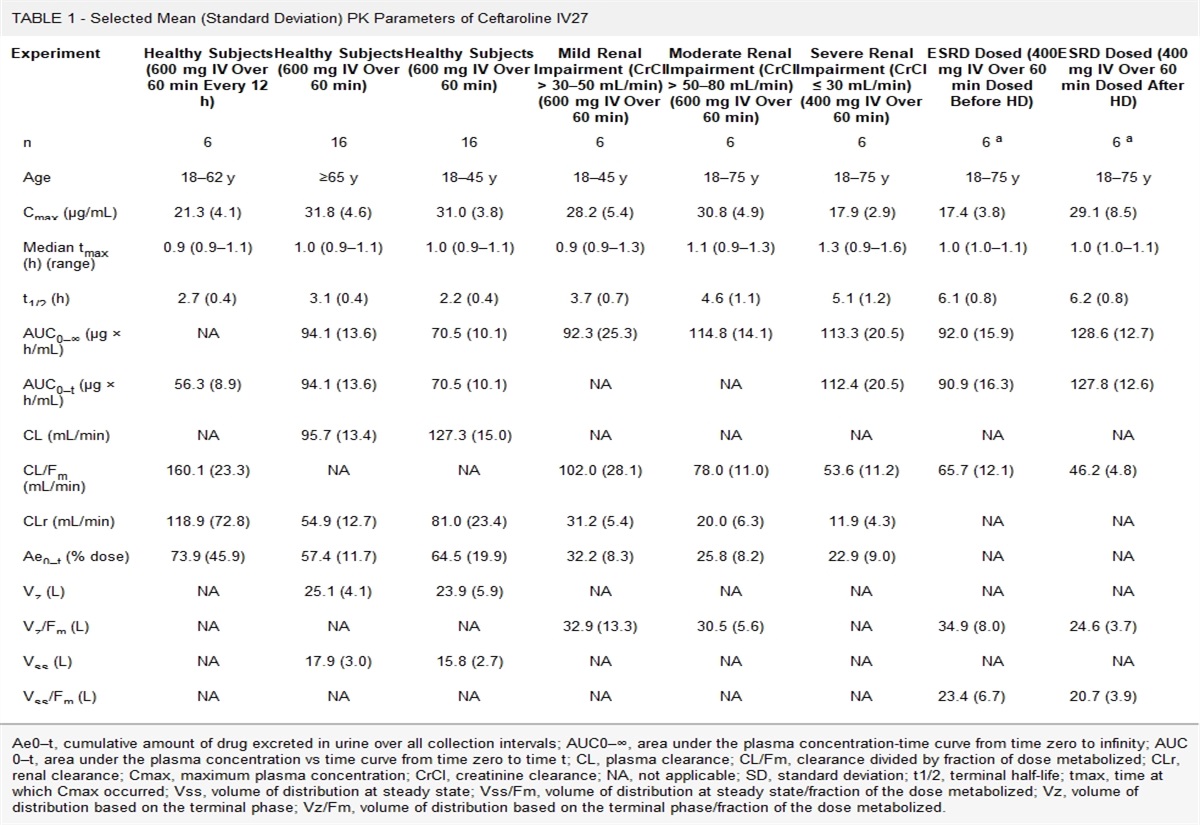
CEFTAROLINE PK/PD DATACeftaroline was first studied in adults before investigation in children.23–26 Selected PK data shown in Table 1 were derived from a series of 6 studies conducted by Riccobene et al27 involving both healthy adults and special populations of interest (ie, healthy elderly adults, adults with renal impairment, and adults with end-stage renal disease [ESRD] on intermittent hemodialysis) prior to approval for use by the FDA and EMA. Selected results from several studies conducted to assess the concentrations of ceftaroline in various tissues from patients and healthy volunteers are shown in Table 2.16,27–31
TABLE 1 - Selected Mean (Standard Deviation) PK Parameters of Ceftaroline IV27 Experiment Healthy Subjects (600 mg IV Over 60 min Every 12 h) Healthy Subjects (600 mg IV Over 60 min) Healthy Subjects (600 mg IV Over 60 min) Mild Renal Impairment (CrCl > 30–50 mL/min) (600 mg IV Over 60 min) Moderate Renal Impairment (CrCl > 50–80 mL/min) (600 mg IV Over 60 min) Severe Renal Impairment (CrCl ≤ 30 mL/min) (400 mg IV Over 60 min) ESRD Dosed (400 mg IV Over 60 min Dosed Before HD) ESRD Dosed (400 mg IV Over 60 min Dosed After HD) n 6 16 16 6 6 6 6 a 6 a Age 18–62 y ≥65 y 18–45 y 18–45 y 18–75 y 18–75 y 18–75 y 18–75 y Cmax (μg/mL) 21.3 (4.1) 31.8 (4.6) 31.0 (3.8) 28.2 (5.4) 30.8 (4.9) 17.9 (2.9) 17.4 (3.8) 29.1 (8.5) Median tmax (h) (range) 0.9 (0.9–1.1) 1.0 (0.9–1.1) 1.0 (0.9–1.1) 0.9 (0.9–1.3) 1.1 (0.9–1.3) 1.3 (0.9–1.6) 1.0 (1.0–1.1) 1.0 (1.0–1.1) t1/2 (h) 2.7 (0.4) 3.1 (0.4) 2.2 (0.4) 3.7 (0.7) 4.6 (1.1) 5.1 (1.2) 6.1 (0.8) 6.2 (0.8) AUC0–∞ (μg × h/mL) NA 94.1 (13.6) 70.5 (10.1) 92.3 (25.3) 114.8 (14.1) 113.3 (20.5) 92.0 (15.9) 128.6 (12.7) AUC0–t (μg × h/mL) 56.3 (8.9) 94.1 (13.6) 70.5 (10.1) NA NA 112.4 (20.5) 90.9 (16.3) 127.8 (12.6) CL (mL/min) NA 95.7 (13.4) 127.3 (15.0) NA NA NA NA NA CL/Fm (mL/min) 160.1 (23.3) NA NA 102.0 (28.1) 78.0 (11.0) 53.6 (11.2) 65.7 (12.1) 46.2 (4.8) CLr (mL/min) 118.9 (72.8) 54.9 (12.7) 81.0 (23.4) 31.2 (5.4) 20.0 (6.3) 11.9 (4.3) NA NA Ae0–t (% dose) 73.9 (45.9) 57.4 (11.7) 64.5 (19.9) 32.2 (8.3) 25.8 (8.2) 22.9 (9.0) NA NA Vz (L) NA 25.1 (4.1) 23.9 (5.9) NA NA NA NA NA Vz/Fm (L) NA NA NA 32.9 (13.3) 30.5 (5.6) NA 34.9 (8.0) 24.6 (3.7) Vss (L) NA 17.9 (3.0) 15.8 (2.7) NA NA NA NA NA Vss/Fm (L) NA NA NA NA NA NA 23.4 (6.7) 20.7 (3.9)Ae0–t, cumulative amount of drug excreted in urine over all collection intervals; AUC0–∞, area under the plasma concentration-time curve from time zero to infinity; AUC0–t, area under the plasma concentration vs time curve from time zero to time t; CL, plasma clearance; CL/Fm, clearance divided by fraction of dose metabolized; CLr, renal clearance; Cmax, maximum plasma concentration; CrCl, creatinine clearance; NA, not applicable; SD, standard deviation; t1/2, terminal half-life; tmax, time at which Cmax occurred; Vss, volume of distribution at steady state; Vss/Fm, volume of distribution at steady state/fraction of the dose metabolized; Vz, volume of distribution based on the terminal phase; Vz/Fm, volume of distribution based on the terminal phase/fraction of the dose metabolized.
ELF, epithelial lining fluid; % penetration, based on the ratio of AUC0–τ in ELF to AUC0–τ in plasma, assuming 20% protein binding in plasma and no protein binding in ELF; f, refers to the parameters determined for unbound ceftaroline concentrations; τ, dosing interval; Muscle fAUC0-τ ratio, ratio of the fAUC0-τ muscle to fAUC0-τ plasma; Subcutis fAUC0-τ ratio, ratio of the fAUC0-τ subcutis to fAUC0-τ plasma; cortical and cancellous bone; % penetration, based on the ratio of AUC in bone to plasma; Subcutis % penetration, based on the ratio of AUCtissue/AUCplasma.
The PK/PD index associated with efficacy for ceftaroline, and other β-lactam antibiotics, is the percentage of time that free drug concentrations, usually measured in serum/plasma, are above the bacteria MIC during a dosing interval (fT > MIC).32 When this index was assessed for ceftaroline in murine thigh and lung infection models, median fT > MIC values of 36% and 44% achieved 1-log kill for S. aureus and S. pneumonia, respectively.32 These PK/PD targets were used to determine the probability of target attainment (PTA) in the population PK analyses that supported the pediatric approvals for ceftaroline.33 Results from simulations using a regimen of 600 mg every 12 hours in adults for skin infection supported the use of 35% fT > MIC for 2-log kill to achieve 100% PTA for strains of S. aureus with MICs up to 1 mg/L.34 In vitro dynamic pharmacokinetic models provided additional data, based on a dosing regimen of 600 mg every 12 hours in adults, documenting PK/PD exposures required for 2-log kill ranging from 18.5% to 33% fT >MIC across different strains of MRSA.35 Using a global collection of S. aureus with higher MICs of 2 mg/L, “treated” in a hollow-fiber model, a dosing regimen of 600 mg every 8 hours provided exposures of 25.2 to 42.7% fT >MIC to achieve a 2-log kill at 24 hours.36 Additionally, results from popPK modeling and simulations based on serum concentrations indicate that the standard pediatric doses of ceftaroline (8 mg/kg/dose for 2 months to <2 years; 12 mg/kg/dose ≥2 years to <18 years) achieves high PTA (>90%) against the pathogens assessed at their susceptible MIC breakpoints (Table 3).3,4,34,37
TABLE 3 - Dosage by Indication in Pediatric Patients 2 Months of Age and Older3,4 Indication Age Range Dosage and Frequency Infusion Time Recommended Duration of Treatment ABSSSIs or CABP 2 mo to <2 y 8 mg/kg every 8 h 5 to 60 min 5–14 d >2 y to <18 y (<3 kg) 12 mg/kg every 8 h >2 y to <18 y (>33 kg) 400 mg every 8 h or 600 mg every 12 h There is insufficient information to recommend dosage adjustments in 3 distinct patient populations: adolescents from 12 to 3,4ABSSSI, acute bacterial skin and skin structure infections; CABP, community-acquired bacterial pneumonia.
A phase 2 study of the safety, efficacy, and PK of ceftaroline (6 mg/kg every 8 hours) in neonates and very young infants (7 to <60 days old) with late-onset sepsis (LOS) was recently conducted by Bradley et al.38 In this study, PK was assessed as a secondary objective. The popPK analysis was included to assess the adequacy of the previous ceftaroline fosamil popPK model developed by Riccobene et al33 based on combined pediatric (neonates to age <18 years) and adult data.38 The observed steady-state PK data obtained in the Bradley et al study38 were consistent with the steady-state concentrations of ceftaroline predicted by Riccobene et al.33 The concentrations detected were generally within 90% model prediction intervals,38 and the neonatal probability of target attainment was >95% based on established PK/PD targets for neonatal pathogens, as originally considered in the clinical trial design for late-onset sepsis in neonates.33
CEFTAROLINE IN CNS INFECTIONSTo determine the utility of ceftaroline in treating infections in the CNS, several nonclinical studies have examined the ability of ceftaroline to penetrate the meninges in rabbit models of meningitis. For example, Stucki et al15 compared the antibacterial activity of ceftaroline and cefepime against the Gram-negative strains Escherichia coli (QK-9) and Klebsiella pneumoniae (ATCC 1173687) using the rabbit model established by Dacey and Sande.39 Although the results indicated that both ceftaroline and cefepime had bactericidal activity, ceftaroline was found to be superior to cefepime in terms of bacterial killing rate against both strains (all P's < 0.001), although the clinical significance of this finding requires additional investigation. The study also assessed the level of penetration of ceftaroline into inflamed and uninflamed meninges, with findings of 15% and 3%, respectively.15 Using the same model, Cottagnoud et al14 conducted a study to assess the antibacterial activity of both ceftaroline and ceftriaxone against a penicillin-sensitive and a penicillin-resistant strain of Streptococcus pneumoniae in inflamed meninges. The study results showed that the CSF penetration rate of ceftaroline was ~14%, which provided bactericidal activity against both S. pneumoniae isolates. Although the MICs for ceftaroline and ceftriaxone differed, both exhibited similar killing rates against the penicillin-sensitive S. pneumoniae strain (P < 0.06). However, killing at 8 hours was significantly higher for ceftaroline (P < 0.03). Furthermore, the killing rate for ceftaroline was significantly superior to that of ceftriaxone against the penicillin-resistant S. pneumoniae strain (P < 0.009).14 Mermer et al40 employed an experimental rabbit meningitis model developed by Suntur et al41 using the ATCC 43300 MRSA strain. In this model, the antibacterial activity of ceftaroline and vancomycin were compared and showed similar effectiveness.40
More recently, a population pharmacokinetic model in rats was developed by Helfer et al42 to describe alterations in ceftaroline brain disposition caused by meningitis in healthy and MRSA-infected rats (ATCC 43300). Blood and brain microdialysate samples were obtained after a single bolus dose of ceftaroline fosamil (20 mg/kg) administered intravenously. Plasma data were modeled as 1 compartment, and brain data were added to the model as a second compartment, with bidirectional drug transport between plasma and brain (Qin and Qout). The Qin was approximately 60% higher in infected animals, leading to greater brain exposure to ceftaroline. Ceftaroline brain penetration was influenced by MRSA infection, increasing from 17% (Qin/Qout) in healthy animals to 27% in infected animals. Simulations of a 2-hour intravenous (IV) infusion of 50 mg/kg every 8 hours achieved 90% probability of target attainment (PTA) in plasma and brain for the European Committee on Antimicrobial Susceptibility Testing and modal MRSA MIC (0.25 mg/L), suggesting that the drug should be considered an option for treating CNS infections.
Ceftaroline treatment of CNS infections in humans has also been published. A case study of a spinal epidural abscess patient with a MRSA was presented by Bucheit et al.8 The patient initially received acyclovir 550 mg every 8 hours, ceftriaxone 2 g every 12 hours, and vancomycin (loading dose of 1 g followed by 650 mg every 8 hours) for suspected meningitis. Cultures taken from incision and drainage of a spinal epidural abscess after 4 days of vancomycin therapy remained positive for MRSA. The patient was switched from vancomycin to daptomycin, with repeat incision and drainage occurring 24 hours into daptomycin therapy. MRSA blood cultures were persistently positive 7 days into therapy with daptomycin. Ceftaroline salvage therapy (600 mg IV every 12 hours) was started and continued for 4 weeks. The investigators noted that ceftaroline was used off-label at the dose of 600 mg q12h, as there are no formal guidelines for ceftaroline for the treatment of epidural abscesses.8 Roujansky et al43 presented a case in of meningioma resection requiring a postoperative VP shunt, subsequently infected by S. epidermidis. The use of vancomycin was not felt to be medically appropriate by the patient's physicians. Treatment with daptomycin for 10 days proved ineffective. Ceftaroline salvage therapy (600 mg q6h) was begun at the time of VP shunt removal, with sterile CSF cultures after 6 days. A case report of a patient with successful treatment of an MRSA ventriculopleural shunt infection was published by Cies et al.44 CSF concentrations of ceftaroline were determined in this patient, and considered to be low, with a concentration approximately half of what has been demonstrated in rabbit meningitis models; however, the child had a successful clinical outcome. The case report did not specify the degree of meningeal inflammation.44
Stein et al17 conducted a study to evaluate the PK and PD of ceftaroline in serum and CSF samples from 5 neurosurgical patients with an EVD treated prophylactically with ceftaroline. None of the patients were infected at the time of study. Results showed that the mean exposure ratio (AUCCSF/AUCserum) was quite low with uninflamed meninges at 1.1%. It was not noted whether free, unbound drug, or total drug AUCCSF/AUCserum were assessed. The investigators also performed time-kill curves on serum and CSF from these neurosurgical patients against single isolates: methicillin-sensitive S. aureus (MIC to ceftaroline = 0.19 mg/L), a strain of MRSA (MIC to ceftaroline = 0.5 mg/L), and a coagulase-negative staphylococcal isolate (MIC to ceftaroline = 0.19 mg/L). Although bactericidal activity was noted in serum against these isolates, no CSF sample demonstrated antibacterial activity against the staphylococcal isolates.17 An additional study assessing the PK of free ceftaroline concentrations in the CSF of 9 neurosurgical patients with an EVD in the intensive care unit (none with bacterial infection) was conducted by Chauzy et al.16 The results of this PK analysis and population modeling (popPK) study of ceftaroline CNS penetration in these patients estimated a ratio of the mean free-drug AUC0-∞ in CSF to the mean free-drug AUC0-∞, in plasma of 0.064, with mean maximum unbound concentration reached in CSF of 0.22 mg/L. Based on the PK data collected, the investigators determined that the ceftaroline CSF concentrations were below those believed to be effective against pathogens with MICs between 1 and 2 mg/L in patients with minimal CSF inflammation.16 Although lower CSF glucose concentrations were associated with higher ceftaroline penetration, this was not an unexpected finding given the association of lower CSF glucose concentrations with increased inflammation.45 Helfer et al22 recently used the free CSF concentrations measured in the study by Chauzy et al16 and the free concentrations determined by microdialysis in soft tissues and muscle29 to build a popPK model and perform simulations to evaluate the PTA of different ceftaroline dosing regimens. Results from the simulations indicated that sufficient coverage of the approved doses is obtained in soft tissues, and that the penetration of ceftaroline into the CSF was dependent on the degree of meningeal inflammation, varying from 4% (absence of inflammation, mean glucose levels of 5 mmol/L) to 19% in mildly inflamed meninges (mean glucose levels of 2.8 mmol/L), up to approximately 62% in with inflamed meninges (mean glucose levels of 1.2 mmol/L). Based on these results, the investigators suggested that ceftaroline could be a candidate to treat CNS infection associated with substantial inflammation, such as those caused by MRSA.22
CONCLUSIONSBased on the CNS concentration data presented thus far, as well as the systemic PK/PD profile, ceftaroline has a potential role in the treatment of CNS infections. For bacterial infections in which CSF associated with meningeal inflammation, concentrations are likely to be therapeutic, particularly with the use of doses higher than routinely used for systemic infections, creating an optimal PK/PD exposure. For any PK/PD assessment of antibiotic exposure, the MIC of the infecting pathogen also needs to be considered. Although currently published data for pneumococcus suggest that significant resistance to ceftaroline has not emerged at this time, ongoing global surveillance for susceptibility is critical to assure future success in treatment of CNS infections. Additional prospective, controlled CSF PK studies are required, followed by PK/PD modeling to ensure that the proposed dose to treat a CNS infection will achieve an exposure predicted to successfully treat >95% of children, a higher target than usually sought for soft tissue infections and community-acquired pneumonia. Randomized prospective studies in CNS infection with vancomycin as standard of care will be able to compare safety and efficacy of ceftaroline.
ACKNOWLEDGMENTSMedical writing support was provided by ELM Medical and funded by Pfizer.
REFERENCES 1. Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: executive summary. Clin Infect Dis. 2011;52(3):285–292. 2. Randolph AG, Xu R, Novak T, et al. Vancomycin monotherapy may be insufficient to treat methicillin-resistant Staphylococcus aureus coinfection in children with influenza-related critical illness. Clin Infect Dis. 2019;68(3):365–372. 3. TEFLARO® Prescribing Information [TEFLARO® website]. December 2021. Available at: https://www.rxabbvie.com/pdf/teflaro_pi.pdf. Accessed July 21, 2023. 4. Zinforo® Prescribing Information [Zinforo® website]. March 2022. Available at: https://labeling.pfizer.com/ShowLabeling.aspx?id=12137. Accessed July 21, 2023. 5. Pfaller MA, Mendes RE, Castanheira M, et al. Ceftaroline activity tested against bacterial isolates causing community-acquired respiratory tract infections and skin and skin structure infections in pediatric patients from United States hospitals: 2012–2014. Pediatr Infect Dis J. 2017;36(5):486–491. 6. Sader HS, Flamm RK, Farrell DJ, et al. Activity analyses of staphylococcal isolates from pediatric, adult, and elderly patients: AWARE Ceftaroline surveillance program. Clin Infect Dis. 2012;55(Suppl 3):S181–S186. 7. Sader HS, Farrell DJ, Flamm RK, et al. Antimicrobial activity of ceftaroline and comparator agents when tested against numerous species of coagulase-negative Staphylococcus causing infection in US hospitals. Diagn Microbiol Infect Dis. 2016;85(1):80–84. 8. Bucheit J, Collins R, Joshi P. Methicillin-resistant Staphylococcus aureus epidural abscess treated with ceftaroline fosamil salvage therapy. Am J Health-Syst Pharm. 2014;71(2):110–113. 9. Cies JJ, Moore WS 2nd, Enache A, et al. Ceftaroline for suspected or confirmed invasive methicillin-resistant Staphylococcus aureus: a pharmacokinetic case series. Pediatr Crit Care Med. 2018;19(6):e292–e299. 10. Ho TT, Cadena J, Childs LM, et al. Methicillin-resistant Staphylococcus aureus bacteraemia and endocarditis treated with ceftaroline salvage therapy. J Antimicrob Chemother. 2012;67(5):1267–1270. 11. Kuriakose SS, Rabbat M, Gallagher JC. Ceftaroline CSF concentrations in a patient with ventriculoperitoneal shunt-related meningitis. J Antimicrob Chemother. 2015;70(3):953–954. 12. Polenakovik HM, Pleiman CM. Ceftaroline for methicillin-resistant Staphylococcus aureus bacteraemia: case series and review of the literature. Int J Antimicrob Agents. 2013;42(5):450–455. 13. Sakoulas G, Nonejuie P, Kullar R, et al. Examining the use of ceftaroline in the treatment of Streptococcus pneumoniae meningitis with reference to human cathelicidin LL-37. Antimicrob Agents Chemother. 2015;59(4):2428–2431. 14. Cottagnoud P, Cottagnoud M, Acosta F, et al. Efficacy of ceftaroline fosamil against penicillin-sensitive and -resistant streptococcus pneumoniae in an experimental rabbit meningitis model. Antimicrob Agents Chemother. 2013;57(10):4653–4655. 15. Stucki A, Acosta F, Cottagnoud M, et al. Efficacy of ceftaroline fosamil against Escherichia coli and Klebsiella pneumoniae strains in a rabbit meningitis model. Antimicrob Agents Chemother. 2013;57(12):5808–5810. 16. Chauzy A, Nadji A, Combes JC, et al. Cerebrospinal fluid pharmacokinetics of ceftaroline in neurosurgical patients with an external ventricular drain. J Antimicrob Chemother. 2019;74(3):675–681. 17. Stein GE, Yasin F, Smith C, et al. A pharmacokinetic/pharmacodynamic analysis of ceftaroline prophylaxis in patients with external ventricular drains. Surg Infect (Larchmt). 2015;16(2):169–173. 18. Robertson FC, Lepard JR, Mekary RA, et al. Epidemiology of central nervous system infectious diseases: a meta-analysis and systematic review with implications for neurosurgeons worldwide. J Neurosurg. 2019;130(4):1107–1126. 19. Gutierrez-Murgas Y, Snowden JN. Ventricular shunt infections: immunopathogenesis and clinical management. J Neuroimmunol. 2014;276(1–2):1–8. 20. Chihi M, Gembruch O, Ahmadipour Y, et al. Predictors of catheter-associated meningitis in pediatric patients after brain tumor surgery: a 10-year single center experience. J Neurol Sci. 2020;418:117100. 21. Koljonen PA, Chan SHS, Liu T, et al. Intrathecal baclofen pump infection with meningitis: effective treatment by radical debridement and intrareservoir baclofen-vancomycin co-infusion. Neuromodulation. 2021;24(7):1223–1228. 22. Helfer VE, Zavascki A, Zeitlinger M, et al. Population pharmacokinetic modeling and probability of target attainment of ceftaroline in brain and soft tissues. Antimicrob Agents Chemother. 2022;66(9):e0074122. 23. Lim L, Sutton E, Brown J. Ceftaroline: a new broad-spectrum cephalosporin. Am J Health-Syst Pharm. 2011;68(6):491–498. 24. Merker A, Danziger LH, Rodvold KA, et al. Pharmacokinetic and pharmacodynamic evaluation of ceftaroline fosamil. Expert Opin Drug Metab Toxicol. 2014;10(12):1741–1750. 25. Kiang TK, Wilby KJ, Ensom MH. A critical review on the clinical pharmacokinetics, pharmacodynamics, and clinical trials of ceftaroline. Clin Pharmacokinet. 2015;54:915–931. 26. Corey A, So TY. Current clinical trials on the use of ceftaroline in the pediatric population. Clin Drug Investig. 2017;37(7):625–634. 27. Riccobene T, Jakate A, Rank D. A series of pharmacokinetic studies of ceftaroline fosamil in select populations: normal subjects, healthy elderly subjects, and subjects with renal impairment or end-stage renal disease requiring hemodialysis. J Clin Pharmacol. 2014;54(7):742–752. 28. Riccobene TA, Pushkin R, Jandourek A, et al. Penetration of ceftaroline into the epithelial lining fluid of healthy adult subjects. Antimicrob Agents Chemother. 2016;60(10):5849–5857. 29. Matzneller P, Lackner E, Lagler H, et al. Single- and repeated-dose pharmacokinetics of ceftaroline in plasma and soft tissues of healthy volunteers for two different dosing regimens of ceftaroline fosamil. Antimicrob Agents Chemother. 2016;60(6):3617–3625. 30. MacVane S, Su S, Housman S, et al. A-1341 – Penetration of Ceftaroline (CPT) and Avibactam (AVI) into Subcutaneous Tissue After Multiple IV Doses of Ceftaroline Fosamil (CPT-F)/Avibactam (CXL) in Patients with Diabetic Foot Infections (DFI). 2014. Available at: https://www.abstractsonline.com/Plan/ViewAbstract.aspx?sKey=cc018810-0b59-4039-9af7-cdb3a90821a9&cKey=79b71140-f2e5-4dcb-8b1f-5693c6711811&mKey=5d6b1802-e453-486b-bcbb-b11d1182d8bb. Accessed July 21, 2023. 31. Riccobene TA, Cole P, Wolferstetter E, et al. A-1333 – Penetration of Ceftaroline (CPT) into Bone Following Administration of Ceftaroline Fosamil (CPT-F) to Subjects Undergoing Total Hip Replacement Surgery. 2014. Available at: https://www.abstractsonline.com/Plan/ViewAbstract.aspx?sKey=cc018810-0b59-4039-9af7-cdb3a90821a9&cKey=c0b92dbb-8b6d-4174-901a-567a35e6820d&mKey=5d6b1802-e453-486b-bcbb-b11d1182d8bb. Accessed July 21, 2023. 32. Andes D, Craig WA. Pharmacodynamics of a new cephalosporin, PPI-0903 (TAK-599), active against methicillin-resistant Staphylococcus aureus in murine thigh and lung infection models: identification of an in vivo pharmacokinetic-pharmacodynamic target. Antimicrob Agents Chemother. 2006;50(4):1376–1383. 33. Riccobene TA, Khariton T, Knebel W, et al. Popu
Comments (0)