
Remember me








Children supported by extracorporeal membrane oxygenation (ECMO) are at significant risk of bleeding and thrombotic complications, which are associated with increased morbidity and mortality (1–5). Clinicians use hemostatic agents to treat bleeding or to prevent bleeding in patients anticipated to be at high risk for bleeding. Despite potential therapeutic benefits of hemostatic agents in this vulnerable patient population, there is variation in administration between clinicians and institutions (6).
The objective of this subgroup of the Pediatric ECMO Anticoagulation CollaborativE (PEACE) was to derive systematic review-informed, modified Delphi consensus regarding antifibrinolytic and adjunct hemostatic agents in pediatric ECMO support including antifibrinolytics (epsilon-aminocaproic acid [EACA] or tranexamic acid), recombinant factor VIIa (rFVIIa), or topical hemostatic agents (THAs).
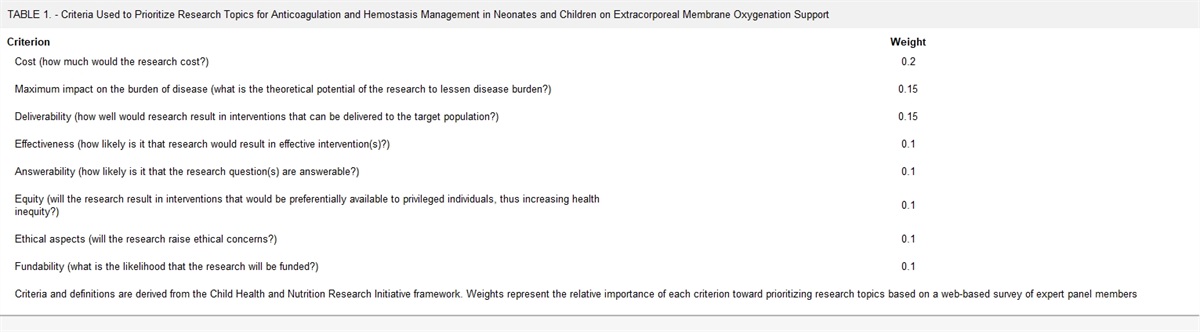
METHODSDetailed methods and definitions of clinically relevant bleeding are described in the PEACE executive summary (7). Briefly, a structured literature search was performed using PubMed, EMBASE, and Cochrane Library (CENTRAL) databases from January 1988 to May 2020, with an update in May 2021, using a combination of medical subject heading terms and text words to investigate pediatric patients supported on ECMO (population), if antifibrinolytics (EACA or tranexamic acid), rFVIIa, THAs, or a hemostatic treatment algorithm or combination of hemostatic agents (interventions) compared with standard/conservative measures or alternate hemostatic agents (comparison) impacted outcomes (outcomes) (Supplemental Methods, https://links.lww.com/PCC/C491). Two authors independently reviewed citations with a third independent reviewer resolving any conflicts (7). Evidence tables were constructed using a standardized data extraction form. Risk of bias was assessed using the Quality in Prognosis Studies (QUIPS) tool or the revised Cochrane risk of bias for randomized trials, as appropriate (8–10), and the evidence was evaluated using the Grading of Recommendations Assessment, Development, and Evaluation system (11,12). A panel of 48 experts met over 2 years to develop evidence-based recommendations and, when evidence was lacking, expert-based consensus statements. Supporting literature was reviewed and statements were developed using the Evidence to Decision framework, emphasizing the panel’s assessment of risks versus benefits of each proposed statement and a prioritized list of patient outcomes that had been created by a web-based survey of expert panel members (13–15). A web-based modified Delphi process was used to build consensus via the Research And Development/University of California Appropriateness Method. Consensus was defined as greater than 80% agreement (16,17). Additional references, not included in the structured literature search, were included in rationale statements to provide context but were not used to derive recommendations or consensus statements.
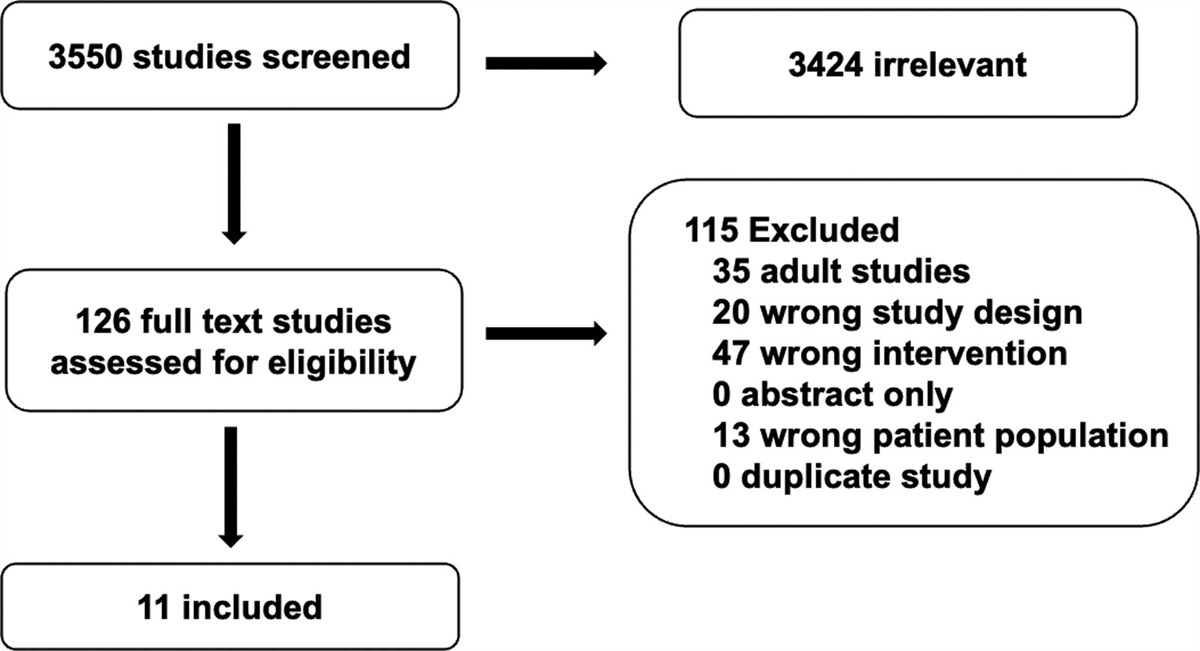
RESULTSThe structured literature search identified 3550 citations with 3424 excluded based on the abstract. An additional 115 references were excluded based on full article review, leaving 11 references for recommendation and consensus statement creation (Fig. 1). The included references are detailed in Supplemental Table 1 (https://links.lww.com/PCC/C491). A summary of the risk of bias assessments is in Supplemental Figure 1 (https://links.lww.com/PCC/C491). One weak recommendation and three consensus statements were developed and reached agreement (> 80%).
 Figure 1.:
Figure 1.: Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram of studies screened and included in the pediatric extracorporeal membrane oxygenation antifibrinolytic and adjunct hemostatic agents group.
Systemic Antifibrinolytic and Hemostatic Agents Consensus Statement6.1 In ECMO patients with bleeding or anticipated to be at high-risk of bleeding, use of lysine analog antifibrinolytic agents (epsilon aminocaproic acid, tranexamic acid) may be considered to decrease bleeding as part of a multimodality blood management strategy.Consensus panel expertise with weak agreement, 93% agreement (n = 46), median 8 (IQR 7–9).
Summary of the evidence.Four studies investigated EACA. A retrospective cohort of neonates who received prophylactic EACA for “high-bleeding risk” was compared with a historical cohort and “low-risk” neonates not receiving EACA (18). “High-bleeding risk” factors included surgical procedures, hypoxia, acidosis, coagulopathy, prematurity, or intracranial hemorrhage (ICH). EACA dosing consisted of 100 mg/kg IV bolus pericannulation, followed by 30 mg/kg/hr infusion until decannulation. Neonates receiving this regimen had less bleeding and required fewer blood products, with the greatest difference seen in the congenital diaphragmatic hernia (CDH) and congenital heart disease patients. No EACA patients developed ICH (12% of controls), whereas thrombotic complications were nonsignificantly more frequent with EACA. A subsequent randomized control trial of prophylactic EACA in neonates on ECMO used the aforementioned protocol (19). Transfusion requirements, bleeding, and thrombotic complications were similar; however, a trend toward higher ICH frequency was observed with EACA. A retrospective study of ECMO patients who received prophylactic EACA for “high-bleeding risk” compared results with “low-risk” institutional controls and Extracorporeal Life Support Organization (ELSO) data. Compared with ELSO, EACA patients required more frequent circuit changes, and less surgical site bleeding with similar rates of ICH, thrombotic complications, and mortality. Compared with institutional controls, transfusion requirements, and patient-related thromboses were similar; however, a greater frequency of circuit changes was observed. A retrospective pediatric ECMO study compared standard therapy with bleeding and high-risk protocols with and without EACA; the frequency of circuit changes was similar between groups (20).
One historical control study examined prophylactic tranexamic acid in neonates with CDH on ECMO (21). Dosing and timing were inconsistent; however, those receiving tranexamic acid experienced less bleeding and blood transfusions, with similar thrombotic complication rates.
Smaller series report antifibrinolytics in pediatric periprocedural ECMO, including postcardiotomy, lung biopsies, and CDH (21–25). See PEACE consensus recommendations for the management of pediatric ECMO during the periprocedural period for details (26). In a historical control study in CDH and ECMO, EACA administration was associated with reduced perioperative blood loss, transfusion requirements, and surgical reexploration with improved survival and no statistical increase in thrombotic complications or ICH (25). Supporting data are also available for antifibrinolytics in bleeding or as prophylaxis in adult ECMO (27,28). Consistent with our statement and based on similar data, the Societies of Thoracic Surgery and Cardiovascular Anesthesiologists Blood Conservation Task Force advocate to consider antifibrinolytic therapy to reduce hemorrhagic complications in ECMO patients (class IIa) (29).
Balance of benefits versus harms.The paucity of high-quality data, study heterogeneity, inconsistent findings, limited safety data for optimal dosing, and potential for complications resulted in an informed consensus statement on lysine-analog antifibrinolytic agents (18–21,30). This consensus view covers both EACA and tranexamic acid, with evidence reasonably consistent between these agents, and a precedent for combining both agents in guidelines statements (29).
Other considerations: Heterogeneity.Included and supporting data vary in terms of populations, antifibrinolytic indications such as bleeding or prophylaxis, and definitions of high risk. Optimal regimen remains unclear, with variable doses, intervals, and durations described (27,28,31–34). Although an in vitro study on EACA in ECMO found no significant sequestration of the drug within the circuit (33), dosing questions remain even in the highly studied cardiac surgical population (34,35). Across all studies, reported efficacy is inconsistent, and descriptions of thrombotic events, safety, and pharmacokinetics are limited (29,36–39). In cardiac surgery, prophylactic intraoperative antifibrinolytics have been recommended; however, a seven-fold increase in seizure risk with tranexamic acid has been reported (29,36,37). Further studies on antifibrinolytic agents in pediatric ECMO are needed to inform evidence-based recommendations.
Age.Included data informing this recommendation was predominantly in neonates, although findings are anticipated to apply across pediatric age.
Agents.Lysine-analog antifibrinolytic agents (EACA, tranexamic acid) reversibly bind to plasminogen, preventing conversion into plasmin, a serine protease that degrades fibrin (31–33). Aprotinin, a nonspecific serine protease inhibitor, while traditionally included in the antifibrinolytic class, is excluded from the recommendations. Following the publication of the Blood Conservation Using Antifibrinolytics Trial aprotinin is not routinely indicated for bleeding (40,41).
Route.No data met the inclusion criteria for alternate administration routes. Evidence suggests topical antifibrinolytics (e.g., soaked gauze), independent of IV doses, may limit cardiac surgical site or oral cavity bleeding (29,32). Inhaled or bronchoscopic tranexamic acid has been described for life-threatening pulmonary hemorrhage with varying doses and efficacy reported (32,42–47).
Consensus Statement6.2 In the ECMO patient – because of the risk of thrombotic complications, we advise against the use of Factor VIIa (rFVIIa) except in the case of life-threatening bleeding refractory to multimodality blood management and resuscitation that addresses factors contributing to bleeding.Consensus panel expertise with strong agreement, 96% agreement (n = 46), median 8 (IQR 7–9).
Summary of the evidence.A retrospective case series evaluated rFVIIa in pediatric ECMO patients with bleeding, comparing those administered rFVIIa to historical controls (48). Bleeding and transfusion requirements significantly decreased following rFVIIa administration with similar rates of thromboembolic complications, circuit failures, and mortality between groups. Other data were derived from three observational studies of cardiac surgical patients including subsets on ECMO. Neonates who received rFVIIa experienced more clinically significant thrombotic complications compared with control patients (49). In children with bleeding on ECMO who received rFVIIa compared with blood products alone, rFVIIa reduced bleeding volume and blood product use; however, thrombotic events occurred in 25%, including two ECMO patients with major patient- and circuit-related complications (50). Another registry review of children on ECMO treated with rFVIIa reported treatment response rate of 82% and significant reduction in blood transfusions despite dose variability with thromboembolic event rate of 19% (51).
Smaller pediatric ECMO case series and data in pediatric cardiac surgical bleeding where rFVIIa is reported as rescue therapy to control refractory hemorrhage informed our statement; however, varying doses, frequency, inconsistent efficacy, and variable adverse event rates are reported (52–57). Supporting data exists for adult ECMO and aligns with our recommendation. The Societies of Thoracic Surgery and Cardiovascular Anesthesiologists Blood Conservation Task Force states that for cardiac surgical patients on ECMO, rFVIIa therapy may be helpful for life-threatening bleeding, and recommends that potential benefits be weighed against reports of catastrophic acute thrombotic complications (class IIb) (29). In life-threatening bleeding, despite surgery and correction of coagulopathy, rFVIIa controlled bleeding in adults on ECMO; however, patient- and circuit-related thrombotic complications are reported (27,58,59).
Balance of benefits versus harms.No substantive evidence supports routine use of recombinant-activated factor VII (rFVIIa, NovoSeven, Novo Nordisk, Copenhagen, Denmark) in pediatric ECMO. Although rFVIIa may reduce bleeding, the overall safety profile and clinical utility remain uncertain because of small sample sizes and concern for thrombosis including fatal and acute catastrophic events (49,53,56).
Other considerations: Pediatric use and dose.Use of rFVIIa for life-threatening or refractory pediatric bleeding in ECMO is off-label. Recombinant-activated factor VIIa is a vitamin-K-dependent, genetically engineered glycoprotein that activates factors IX and X and enhances thrombin production, encouraging platelets to form a fibrin plug (31). Optimal dose remains unclear (range, 24–174 μg/kg, most commonly 60–90 μg/kg reported) at 1–4 hourly frequency, for 1–23 doses (51,52,56,60).
Other contributing factors.Adult studies support correcting the following before rFVIIa: prothrombin time to greater than 50%, activated partial thromboplastin time ratio to less than greater than 2x normal, platelets to greater than 50,000/mL, fibrinogen to greater than 1 g/L, temperature to greater than 36°C, calcium to greater than 2.2 mM, and hematocrit to greater than 24% (58,59).
Route.Inhaled rFVIIa for hemoptysis refractory to inhaled tranexamic acid has been evaluated in a limited case series and should be reserved as an adjunct therapy for life-threatening, refractory bleeding until safety data are available (32,46).
Topical Hemostatic Agents Recommendation6.3 In ECMO, consider prophylactic application of non-bovine derived topical hemostatic agents at the time of cannulation to decrease cannulation site bleeding as part of a multimodality blood management strategy.Weak recommendation, low-quality pediatric evidence, 83% agreement (n = 46), median 8 (IQR 7–9).
Consensus Statement6.4 During ECMO, it is reasonable to consider the application of non-bovine derived topical hemostatic agents in response to active cannulation site bleeding as part of a multimodality blood management strategy including surgical hemostasis.Consensus panel expertise with weak agreement, 83% agreement (n = 46), median 8 (IQR 7–9).
Summary of the evidence.A single, multicenter prospective randomized controlled trial compared standard cauterization alone with the addition of fibrin sealant (comprised of human topical fibrin complex and human thrombin) prophylactically to control hemostasis at the peripheral ECMO cannulation site in neonates with respiratory failure (61). THAs resulted in greater cannulation-site hemostasis (42% vs. 18%), and less bleeding volume and duration, although no reduction in transfusion requirements and two product-related adverse events were observed (site infections). In a case series of neonates on ECMO who had surgical reexploration for excessive bleeding without a surgical source identified, the application of fibrin glue (comprised of human donor fibrinogen concentrate and bovine thrombin) achieved hemostasis (62).
Despite limited evidence in pediatric ECMO, extensive data review THAs in bleeding or as prophylaxis in adult ECMO and cardiac surgery. A retrospective analysis of bleeding adults supported on ECMO found limited success with THAs (27); however, case reports describe success with Chitosan-based products, with further robust informing data unlikely to emerge (63,64). Aligned with our statements, STS and the International Hemostatic Expert Panel surmise that uncontrolled bleeding has significant clinical and economic impacts, with potentially important benefits to the use of THAs despite potential risks so these agents may be considered for local hemostasis as part of a multimodality blood management program (class IIb) (29,65).
Balance of benefits versus harms.A paucity of high-quality data with extrapolation from other populations informed these statements on THAs. Given the potential benefit of reducing bleeding with minimal risks associated with nonbovine-derived agents, their use is suggested. Potential risks of THAs include immunologic reactions, antibody development, and transmission of viral infections, although these risks are minimized by the use of nonbovine-derived agents. In children, there are 12 reported cases of immune-mediated coagulopathy with life-threatening bleeding due to antibody cross-reactivity from topical bovine thrombin (66,67). In adults, repeated perioperative exposure to topical bovine thrombin increased antibody titers; however, no association with adverse events was identified (64,68). Human-derived thrombin is likely as effective as bovine thrombin in reducing bleeding with reduced risk of antibody production informing our recommendation to use nonbovine-derived THAs if available. Any plasma-derived product carries a potential risk of viral transmission although rigorous elimination steps have resulted in enhanced safety. Synthetic sealants and mechanical agents have a lower risk of adverse events.
Other EtD considerations: Age.Included data informing this consensus statement was in neonates; however, findings are anticipated to apply across pediatric ages.
Type.Included literature describes fibrin-based sealants (nonbovine RCT and bovine case series), biocompatible, biodegradable, effective tissue adhesives comprised of purified, virus-inactivated human fibrinogen, human thrombin, with virus-inactivated human factor XIII occasionally added (65,69). THAs are broadly classified as active or nonactive according to blood clotting agent composition, and categorized by mechanism of action (providing a scaffold for clot formation with compression from swelling versus creating an air-tight seal to form fibrin clot). Multiple agents are commercially available with varying benefits and despite widespread use in cardiac procedures, no data supports the use of a specific agent (29,65).
Route.No data inform recommendations regarding THAs on mucosal surfaces or topical antifibrinolytics in our population.
CONCLUSIONSDespite a systematic review of the literature describing outcomes of pediatric patients supported on ECMO who received antifibrinolytics (EACA or tranexamic acid), rFVIIa, and THAs, evidence to support recommendations was sparse and inconclusive. Although the expert panel reached a consensus on all questions, the strength of the evidence could only substantiate expert opinion-based consensus statements or weak recommendations. Antifibrinolytics or hemostatic concentrates are often provided in life-threatening hemorrhage despite pervasive knowledge gaps regarding indication, dose, route of administration, and duration in addition to lack of clarity regarding risk-benefit balance. Much work remains to determine effective and safe usage strategies.
ACKNOWLEDGMENTSWe thank all members of the Pediatric Extracorporeal Membrane Oxygenation Anticoagulation CollaborativE (PEACE) for their support, especially during the COVID-19 pandemic. The authors would like to acknowledge the important contributions of Dr. M. Patricia Massicotte to the design and execution of the PEACE project. In addition, we thank AABB, the American Society of Extracorporeal Therapists, the American Pediatric Surgical Association, the Children’s Hospital Neonatal Consortium, the Collaborative Pediatric Critical Care Research Network, the European Society for Pediatric and Neonatal Intensive Care, the International Society of Blood Transfusion, Pediatric Cardiac Critical Care Consortium, Pediatric Cardiac Intensive Care Society, the Society for Critical Care Medicine (Pediatric Section and Clinical Pharmacy and Pharmacology Section), and the Society of Thoracic Surgeons.
REFERENCES 1. Dalton HJ, Reeder R, Garcia-Filion P, et al.; Eunice Kennedy Shriver National Institute of Child Health and Human Development Collaborative Pediatric Critical Care Research Network: Factors associated with bleeding and thrombosis in children receiving extracorporeal membrane oxygenation. Am J Respir Crit Care Med. 2017; 196:762–771 2. O’Halloran CP, Andren KG, Mecklosky J, et al.: Mortality and factors associated with hemorrhage during pediatric extracorporeal membrane oxygenation. Pediatr Crit Care Med. 2020; 21:75–81 3. Penk JS, Reddy S, Polito A, et al.: Bleeding and thrombosis with pediatric extracorporeal life support: A roadmap for management, research, and the future from the pediatric cardiac intensive care society: Part 1. Pediatr Crit Care Med. 2019; 20:1027–1033 4. Penk JS, Reddy S, Polito A, et al.: Bleeding and thrombosis with pediatric extracorporeal life support: A roadmap for management, research, and the future from the pediatric cardiac intensive care society: Part 2. Pediatr Crit Care Med. 2019; 20:1034–1039 5. Extracorporeal Life Support Organization (ELSO): International Summary—ECLS Registry Report 2023 30 July 2023. Available at: https://www.elso.org/registry/internationalsummaryandreports/internationalsummary.aspx. Accessed January 10, 2024 6. Ozment CP, Scott BL, Bembea MM, et al.; Pediatric ECMO (PediECMO) subgroup of the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network and the Extracorporeal Life Support Organization (ELSO): Anticoagulation and transfusion management during neonatal and pediatric extracorporeal membrane oxygenation: A survey of medical directors in the United States. Pediatr Crit Care Med. 2021; 22:530–541 7. Alexander PMA, Bembea M, Cashen K, et al.; Pediatric Extracorporeal Membrane Oxygenation (ECMO) Anticoagulation CollaborativE (PEACE), in collaboration with the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network, the Pediatric Critical Care Blood Research Network (BloodNet), and the Pediatric ECMO subgroup of PALISI and the Extracorporeal Life Support Organization (PediECMO): Executive summary: The Pediatric Extracorporeal Membrane Oxygenation Anticoagulation CollaborativE Consensus Conference. Pediatr Crit Care Med. 2024; 25:643–675 8. Sterne JAC, Savovic J, Page MJ, et al.: RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ. 2019; 366:l4898 9. Higgins JP, Sterne JA, Savovic J, et al.: A revised tool for assessing risk of bias in randomized trials. Cochrane Methods. Chandler J, McKenzie J, Boutron I, et al (Eds). Cochrane Database of Systematic Reviews 2016; 10 (Suppl 1) 10. Hayden JA, van der Windt DA, Cartwright JL, et al.: Assessing bias in studies of prognostic factors. Ann Intern Med. 2013; 158:280–286 11. Balshem H, Helfand M, Schunemann HJ, et al.: GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011; 64:401–406 12. Neumann I, Santesso N, Akl EA, et al.: A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016; 72:45–55 13. Alonso-Coello P, Oxman AD, Moberg J, et al.; GRADE Working Group: GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016; 353:i2089 14. Alonso-Coello P, Schunemann HJ, Moberg J, et al.; GRADE Working Group: GRADE Evidence to Decision (EtD) frameworks: A systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016; 353:i2016 15. Neumann I, Brignardello-Petersen R, Wiercioch W, et al.: The GRADE evidence-to-decision framework: A report of its testing and application in 15 international guideline panels. Implement Sci. 2016; 11:93 16. Diamond IR, Grant RC, Feldman BM, et al.: Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol. 2014; 67:401–409 17. Fitch K, Bernstein SJ, Aguilar MD, et al. The RAND/UCLA Appropriateness Method User’s Manual. Santa Monica, CA, RAND, 2001 18. Wilson JM, Bower LK, Fackler JC, et al.: Aminocaproic acid decreases the incidence of intracranial hemorrhage and other hemorrhagic complications of ECMO. J Pediatr Surg. 1993; 28:536–40; discussion 540 19. Horwitz JR, Cofer BR, Warner BW, et al.: A multicenter trial of 6-aminocaproic acid (Amicar) in the prevention of bleeding in infants on ECMO. J Pediatr Surg. 1998; 33:1610–1613 20. Muensterer OJ, Laney D, Georgeson KE: Survival time of ECMO circuits on and off bleeding protocol: Is there a higher risk of circuit clotting? Eur J Pediatr Surg. 2011; 21:30–32 21. van der Staak FH, de Haan AF, Geven WB, et al.: Surgical repair of congenital diaphragmatic hernia during extracorporeal membrane oxygenation: Hemorrhagic complications and the effect of tranexamic acid. J Pediatr Surg. 1997; 32:594–599 22. ElMahrouk AF, Ismail MF, Hamouda T, et al.: Extracorporeal membrane oxygenation in postcardiotomy pediatric patients—15 years of experience outside Europe and North America. Thorac Cardiovasc Surg. 2019; 67:28–36 23. Agati S, Ciccarello G, Salvo D, et al.: Use of a novel anticoagulation strategy during ECMO in a pediatric population: Single-center experience. ASAIO J. 2006; 52:513–516 24. Houmes RJ, Ten Kate CA, Wildschut ED, et al.: Risk and relevance of open lung biopsy in pediatric ECMO patients: The Dutch experience. J Pediatr Surg. 2017; 52:405–409 25. Wilson JM, Bower LK, Lund DP: Evolution of the technique of congenital diaphragmatic hernia repair on ECMO. J Pediatr Surg. 1994; 29:1109–1112 26. Willems A, Anders MM, Garcia A, et al.; Pediatric Extracorporeal Membrane Oxygenation (ECMO) Anticoagulation CollaborativE (PEACE), in collaboration with the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network, the Pediatric Critical Care Blood Research Network (BloodNet), and the Pediatric ECMO subgroup of PALISI and the Extracorporeal Life Support Organization (PediECMO): Management of extracorporeal membrane oxygenation anticoagulation in the perioperative period: The Pediatric Extracorporeal Membrane Oxygenation Anticoagulation CollaborativE Consensus Conference. Pediatr Crit Care Med. 2024; 25:e53–e65 27. Lotz C, Streiber N, Roewer N, et al.: Therapeutic interventions and risk factors of bleeding during extracorporeal membrane oxygenation. ASAIO J. 2017; 63:624–630 28. Buckley LF, Reardon DP, Camp PC, et al.: Aminocaproic acid for the management of bleeding in patients on extracorporeal membrane oxygenation: Four adult case reports and a review of the literature. Heart Lung. 2016; 45:232–236 29. Ferraris VA, Brown JR, Despotis GJ, et al.; Society of Thoracic Surgeons Blood Conservation Guideline Task Force: 2011 update to the Society of Thoracic Surgeons and the Society of Cardiovascular Anesthesiologists blood conservation clinical practice guidelines. Ann Thorac Surg. 2011; 91:944–982 30. Downard CD, Betit P, Chang RW, et al.: Impact of AMICAR on hemorrhagic complications of ECMO: A ten-year review. J Pediatr Surg. 2003; 38:1212–1216 31. Buck ML: Control of coagulation during extracorporeal membrane oxygenation. J Pediatr Pharmacol Ther. 2005; 10:26–35 32. Hensch LA, Hui SR, Teruya J: Coagulation and bleeding management in pediatric extracorporeal membrane oxygenation: Clinical scenarios and review. Front Med (Lausanne). 2018; 5:361 33. Wagner D, Caraballo M, Waldvogel J, et al.: In vitro effects of an extracorporeal membrane oxygenation circuit on the sequestration of aminocaproic acid. Perfusion. 2017; 32:226–229 34. Faraoni D, Rahe C, Cybulski KA: Use of antifibrinolytics in pediatric cardiac surgery: Where are we now? Paediatr Anaesth. 2019; 29:435–440 35. Shi J, Zhou C, Liu S, et al.: Outcome impact of different tranexamic acid regimens in cardiac surgery with cardiopulmonary bypass (OPTIMAL): Rationale, design, and study protocol of a multicenter randomized controlled trial. Am Heart J. 2020; 222:147–156 36. Boer C, Meesters MI, Milojevic M, et al.; Task Force on Patient Blood Management for Adult Cardiac Surgery of the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Cardiothoracic Anaesthesiology (EACTA): 2017 EACTS/EACTA guidelines on patient blood management for adult cardiac surgery. J Cardiothorac Vasc Anesth. 2018; 32:88–120 37. Myles PS, Smith JA, Forbes A, et al.; ATACAS Investigators of the ANZCA Clinical Trials Network: Tranexamic acid in patients undergoing coronary-artery surgery. N Engl J Med. 2017; 376:136–148 38. Fanashawe MP, Shore-Lesserson L, Reich DL: Two cases of fatal thrombosis after aminocaproic acid therapy and deep hypothermic circulatory arrest. Anesthesiology. 2001; 95:1525–1527 39. Hocker JR, Saving KL: Fatal aortic thrombosis in a neonate during infusion of epsilon-aminocaproic acid. J Pediatr Surg. 1995; 30:1490–1492 40. Henry D, Carless P, Fergusson D, et al.: The safety of aprotinin and lysine-derived antifibrinolytic drugs in cardiac surgery: A meta-analysis. CMAJ. 2009; 180:183–193 41. Fergusson DA, Hebert PC, Mazer CD, et al.; BART Investigators: A comparison of aprotinin and lysine analogues in high-risk cardiac surgery. N Engl J Med. 2008; 358:2319–2331 42. O’Neil ER, Schmees LR, Resendiz K, et al.: Inhaled tranexamic acid as a novel treatment for pulmonary hemorrhage in critically ill pediatric patients: An observational study. Crit Care Explor. 2020; 2:e0075 43. Moynihan KM, Ge S, Sleeper LA, et al.: Life-threatening hemoptysis in a pediatric referral center. Crit Care Med. 2021; 49:e291–e303 44. Segrelles Calvo G, De Granda-Orive I, Lopez Padilla D: Inhaled tranexamic acid as an alternative for hemoptysis treatment. Chest. 2016; 149:604 45. Solomonov A, Fruchter O, Zuckerman T, et al.: Pulmonary hemorrhage: A novel mode of therapy. Respir Med. 2009; 103:1196–1200 46. Bafaqih H, Chehab M, Almohaimeed S, et al.: Pilot trial of a novel two-step therapy protocol using nebulized tranexamic acid and recombinant factor VIIa in children with intractable diffuse alveolar hemorrhage. Ann Saudi Med. 2015; 35:231–239 47. Heslet L, Nielsen JD, Nepper-Christensen S: Local pulmonary administration of factor VIIa (rFVIIa) in diffuse alveolar hemorrhage (DAH)—a review of a new treatment paradigm. Biologics. 2012; 6:37–46 48. Niebler RA, Christensen M, Berens R, et al.: Antithrombin replacement during extracorporeal membrane oxygenation. Artif Organs. 2011; 35:1024–1028 49. Christoff AS, Winlaw DS, Curtin J, et al.: Recombinant activated factor VII in neonatal cardiac surgery. Eur J Cardiothorac Surg. 2019; 55:817–822 50. Agarwal HS, Bennett JE, Churchwell KB, et al.: Recombinant factor seven therapy for postoperative bleeding in neonatal and pediatric cardiac surgery. Ann Thorac Surg. 2007; 84:161–168 51. McQuilten ZK, Barnes C, Zatta A, et al.: Off-label use of recombinant factor VIIa in pediatric patients. Pediatrics. 2012; 129:e1533–e1540 52. Veldman A, Neuhaeuser C, Akintuerk H, et al.: rFVIIa in the treatment of persistent hemorrhage in pediatric patients on ECMO following surgery for congenital heart disease. Paediatr Anaesth. 2007; 17:1176–1181 53. Kurkluoglu M, Engle AM, Costello JP, et al.: Single center experience on dosing and adverse events of recombinant factor seven use for bleeding after congenital heart surgery. J Saudi Heart Assoc. 2015; 27:18–22 54. Wittenstein B, Ng C, Ravn H, et al.: Recombinant factor VII for severe bleeding during extracorporeal membrane oxygenation following open heart surgery. Pediatr Crit Care Med. 2005; 6:473–476 55. Chalwin RP, Tiruvoipati R, Peek GJ: Fatal thrombosis with activated factor VII in a paediatric patient on extracorporeal membrane oxygenation. Eur J Cardiothorac Surg. 2008; 34:685–686 56. Long MT, Wagner D, Maslach-Hubbard A, et al.: Safety and efficacy of recombinant activated factor VII for refractory hemorrhage in pediatric patients on extracorporeal membrane oxygenation: A single center review. Perfusion. 2014; 29:163–170 57. Preston TJ, Olshove VF Jr, Ayad O, et al.: Novoseven use in a non-cardiac pediatric ECMO patient with uncontrolled bleeding. J Extra Corpor Technol. 2008; 40:123–126 58. Anselmi A, Guinet P, Ruggieri VG, et al.: Safety of recombinant factor VIIa in patients under extracorporeal membrane oxygenation. Eur J Cardiothorac Surg. 2016; 49:78–84 59. Repesse X, Au SM, Brechot N, et al.: Recombinant factor VIIa for uncontrollable bleeding in patients with extracorporeal membrane oxygenation: Report on 15 cases and literature review. Crit Care. 2013; 17:R55 60. Davis MC, Andersen NE, Johansson P, et al.: Use of thromboelastograph and factor VII for the treatment of postoperative bleeding in a pediatric patient on ECMO after cardiac surgery. J Extra Corpor Technol. 2006; 38:165–167 61. Atkinson JB, Gomperts ED, Kang R, et al.: Prospective, randomized evaluation of the efficacy of fibrin sealant as a topical hemostatic agent at the cannulation site in neonates undergoing extracorporeal membrane oxygenation. Am J Surg. 1997; 173:479–484 62. Moront MG, Katz NM, O’Connell J, et al.: The use of topical fibrin glue at cannulation sites in neonates. Surg Gynecol Obstet. 1988; 166:358–359 63. Muzzi L, Tommasino G, Tucci E, et al.: Successful use of a military haemostatic agent in patients undergoing extracorporeal circulatory assistance and delayed sternal closure. Interact Cardiovasc Thorac Surg. 2012; 14:695–698 64. Clark J, Crean S, Reynolds MW: Topical bovine thrombin and adverse events: A review of the literature. Curr Med Res Opin. 2008; 24:2071–2087 65. Bracey A, Shander A, Aronson S, et al.: The use of topical hemostatic agents in cardiothoracic surgery. Ann Thorac Surg. 2017; 104:353–360 66. Rodgers GM: Immune-mediated coagulopathy associated with topical bovine thrombin: Review of the pediatric literature. J Pediatr Hematol Oncol. 2011; 33:86–88 67. Israels SJ, Israels ED: Development of antibodies to bovine and human factor V in two children after exposure to topical bovine thrombin. Am J Pediatr Hematol Oncol. 1994; 16:249–254 68. Ofosu FA, Crean S, Reynolds MW: A safety review of topical bovine thrombin-induced generation of antibodies to bovine proteins. Clin Ther. 2009; 31:679–691 69. Jackson MR: Fibrin sealants in surgical practice: An overview. Am J Surg. 2001; 182(2 Suppl):1S–7S
Comments (0)