
Remember me




This study had several limitations. In this study, the camera and PA images were aligned; however, because the postures at the time of shooting were different, errors in the alignment remained. Thus, it is challenging to assert that the varicose veins identified by the physicians are perfectly congruent with the varicosities depicted in the PA images. These errors may result in lower BPD values even within regions identified by physicians as varicose veins. Therefore, enhancing the precision of the alignment is imperative, which is anticipated to improve the diagnostic capability of BPD.
Additionally, variations in posture during image acquisition may potentially affect the thickness of blood vessels. Since patients were in the supine or prone position when the PAI system was used in this study, the blood vessels may have been thinner than in the sitting or standing position during the actual diagnosis. It is necessary to investigate whether such differences in posture affect how varicose veins appear on PA images.
Optimization of the diameter of the circular area also may hold potential for augmenting the diagnostic accuracy of BPD. A circular area that is too small may merely blur the vascular image, thus only depicting local vascular density. Conversely, an excessively large circular area could impair the ability to discern local variations. The diameter of the circular area was set at 10 mm to facilitate the detection of vascular conditions, including not only dilated vessels but also reticular veins (vessel diameter 2–3 mm) and spider veins (vessel diameter less than 1 mm), as variations in the proportion of the vascular region within the circular area. This size was found to be effective as it allowed for the detection of spider-web patterns, which were also observable upon clinical examination, with a high BPD. Future studies should aim to increase the sample size and continue the search for an optimal circular area size to determine the most effective value.
In addition, varicose veins were assumed to be areas with high BPD; however, if it becomes necessary to distinguish these veins from clusters of web vessels or fine tortuous vessels, they may be identified by adding a curvature judgment.
Within the scope of this research, the difference between areas identified as varicose veins and other regions was calculated as the BPD ratio. The reason for using BPD ratio is the significant variability and individual differences in the BPD of areas not identified as varicose veins, which was observed to be a minimum value of 0.08 and a maximum value of 0.31 across the nine subjects and 12 limbs analyzed (Table 2).
In this study, the varicose vein area was determined based on the area specified by the physician, but further detection methods are needed to extract varicose vein areas from images in the future. Consideration of deviations from the mean or the use of AI for automatic segmentation into two groups may be necessary. In developing this, it is posited that including images of the healthy side in the analysis will be crucial for examining the balance between sensitivity and specificity in the extraction of varicose vein regions.
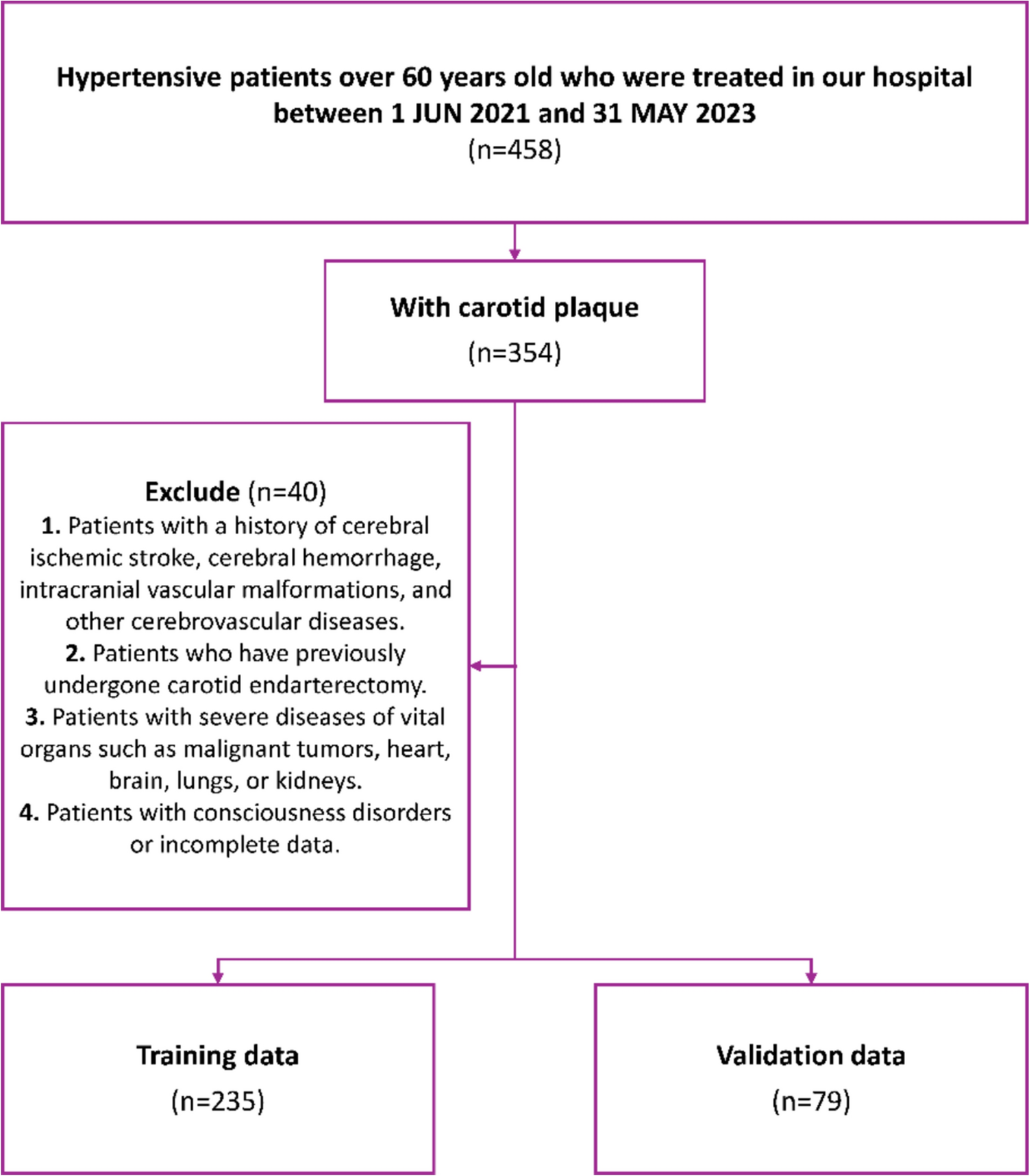
Moreover, this study was limited to a small cohort of only nine patients, which may have been insufficient for analyzing the correlation between the CEAP classification and the BPD ratio. Further investigation is essential to stratify the CEAP severity within individual lower limbs and to explore the association with the “P” (pathophysiologic) category of the CEAP classification, which is only verifiable through ultrasound. This necessitates the inclusion of a larger patient population, encompassing those with healthy control groups as well.
Future workThe lower limb images acquired via PAI allowed visualization of many vessels that could not be confirmed by visual inspection, and the course of the vessels could be observed in more detail (Fig. 7a). The BPD heat map created in this study revealed the existence of high BPD regions not only in the marked varicose vein sites but also in other locations. By detecting changes in vessels that are not visible to the eye, such as thin or deep-running vessels, this study may contribute to the early detection of lower limb varicose veins. Various display methods using BPD (Figs. 5b, 7b) indicated the potential to contribute to diagnostic support, such as reducing the interobserver variability of visual inspection and enabling the early detection of varicose veins. Moreover, quantification of BPD is expected to be useful in various situations such as evaluating treatment effects and performing screening tests.
Fig. 7
Example of a PA image and varicose vein display. b Example of another colored BPD map for varicose vein generated from PA image (a)
Comments (0)