
Remember me





Stroke is the third leading cause of death worldwide, with approximately 80% of deaths due to ischemic stroke [1]. Gastrodin (GAS) is a compound found abundantly in Gastrodia elata that has been studied for its significant neurological protective properties, as evidenced in clinical studies [2]. Electroacupuncture (EA), employed in treating cerebral ischemia, has been shown to be safe without adverse effects. Rats subjected to acupuncture at the Baihui (GV20) and Zusanli (ST36) points display a capacity to regulate microglial polarization, increase brain-derived neurotrophic factor (BDNF) levels and mitigate inflammatory reaction, and then exhibit the potential to improve postcerebral ischemic neurological function and reduce infarct areas in rats [3]. The comprehensive mechanism underlying the synergy between traditional Chinese medicine (TCM) and EA in the treatment of cerebral ischemia, however, remains incompletely elucidated and requires further investigation.
Alterations in BDNF expression within brain tissues have been linked to various central nervous system disorders, such as stroke, parkinsonism and Alzheimer’s [4]. BDNF plays a pivotal role in sustaining normal neuronal physiological functions, modulating axonal plasticity and facilitating neuronal repair, crucial for neuronal network system homeostasis [5]. Conversely, interleukin-6 (IL-6), a multifaceted proinflammatory cytokine, is implicated in the pathophysiological processes of numerous diseases. Suppression of IL-6 expression postcerebral ischemia has been associated with dampening the inflammatory response, conferring a certain protective effect against cerebral ischemia [6]. This study aims to investigate the mechanisms underlying rat cerebral protection after cerebral ischemia using a combination of GAS and EA (GAS + EA). The study focuses on the roles of BDNF and IL-6 and intends to provide an experimental basis for the treatment of cerebral ischemia with TCM.
Materials and methods Experimental animalsA total of 50 rats were obtained from the Qinglongshan Animal Experiment Center, certified under Conformity No. SCXK (Shanghai) 2018-0004. Adaptive feeding was conducted in separate cages for 7 days in the animal room, following the Animal Ethics and Ethics Code of Wannan Medical College (No. LLSC-2022-012). The rats were randomly assigned to five groups using a random number table method, with 10 rats per group. The groups were as follows: sham, model, GAS, EA and GAS + EA.
Model preparation methodsRat cerebral ischemia model was established using the modified Zea longa bolus method [7]. An intraperitoneal injection of 1.5% pentobarbital sodium (2 ml/kg) was administered to anesthetize the rat. The right common carotid artery, internal carotid artery and external carotid artery were exposed by separating the subcutaneous tissue in the midline of the rat’s neck layer by layer with a glass parting needle. The common carotid and external carotid arteries were then ligated, and an arterial clip was used to clamp the distal end of the internal carotid artery. A small incision was made at the proximal bifurcation of the internal carotid and external carotid arteries. Then, the bolus wire was inserted, and the arterial clip was released. The bolus wire was continued to be inserted until slight resistance was felt, allowing the tip of the bolus to reach the bifurcation of the anterior and middle cerebral arteries. Finally, the internal carotid artery was ligated to secure the wire and prevent bleeding. Post incision closure, suturing and sterilization, successful modeling was assessed after 2 h, during the rats’ awakened state. Successful modeling criteria included neurological impairment signs such as partial extension of the contralateral forepaw during walking, tilting or circling toward the contralateral side [8]. Treatments were initiated 24 h postsurgery.
The sham group underwent anesthesia via intraperitoneal injection of 1.5% pentobarbital sodium (2 ml/kg). The subcutaneous tissues were then separated layer by layer using a glass parting needle at the midline of the neck of the rats to expose the right common carotid artery, the internal carotid artery and the external carotid artery. The incision was sutured and sterilized. The rats were reared under normal conditions and subsequently subjected to pathological, biochemical and other experiments, along with the remaining four groups of rats.
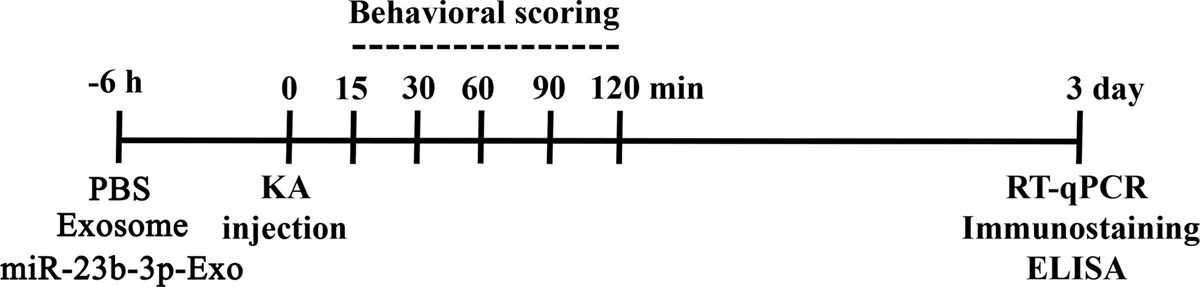
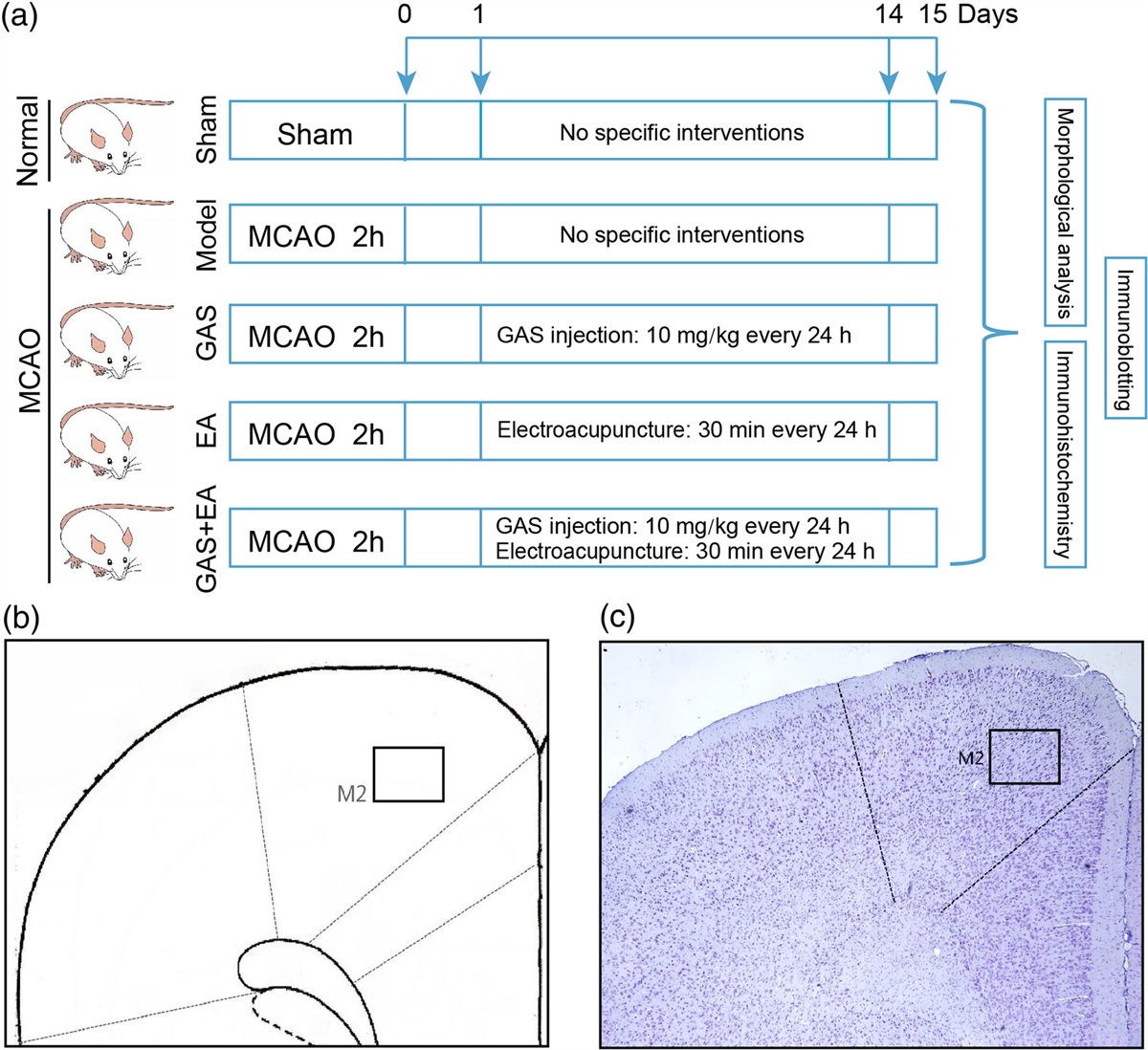
Experimental programThe experimental groups were designated as follows (Fig. 1a): the sham-operated and model groups received no treatment. In the GAS group, rats were administered GAS (10 mg/kg, H20064392, Sinopharm, Shanghai, China) via intraperitoneal injection once daily for 14 consecutive days. In the EA group, rats were first anesthetized by intraperitoneal injection of 1.5% sodium pentobarbital (2 ml/kg), and then EA was administered after the rats were anesthetized. The ST36 (5 mm lateral to the anterior tibial tuberosity, 7 mm straight) and GV20 (the center of the parietal bone, 2 mm diagonally) points were stimulated using sparse dense wave EA at a current of 1 mA and frequency of 2/10 Hz, 30 min per day, continuously for 14 days, referencing previous literature [9]. The GAS + EA group received both intraperitoneal GAS injections and EA stimulation using the same dosages and methods as the individual GAS and EA groups.
 Fig. 1:
Fig. 1: The experimental schema of this study. (a)The rats in the experiment were divided into five distinct groups: the sham group, the model group, and three treatment groups (GAS, EA, GAS + EA), which were established using the MACO method. The model group received no specific intervention, while the GAS group was administered GAS at a dose of 10 mg/kg every 24 h for 14 consecutive days. The EA group received EA treatment for 30 min every 24 h for 14 consecutive days. The GAS + EA group, which received both EA and GAS injection, underwent treatment for 14 consecutive days. On the 15th day, after sacrificing the rats, the samples were collected and preserved for further analysis via Nissl staining, immunohistochemistry and immunoblotting techniques. (b, c) Schematic representation of the frontal cortical M2 region of the brain selected for this study. EA, electroacupuncture; GAS, gastrodin; MACO, middle cerebral artery occlusion.
After the 14-day intervention period, five rats were randomly selected from each group and anesthetized with 1.5% pentobarbital Na (2 ml/kg) via intraperitoneal injection. The rats were rapidly perfused with 0.9% saline through the left ventricular ascending aorta followed by 4% paraformaldehyde solution at 4 °C. Afterward, the brain tissue was taken and fixed in 4% paraformaldehyde for one day. The brain tissue was then sectioned anterior to the optic cross, and the frontal cortex was dehydrated in gradient alcohol, cleared, embedded in wax and embedded for subsequent Nissl staining and immunohistochemical analyses. Concurrently, the remaining five rats in each group were anesthetized with 1.5% pentobarbital Na (2 ml/kg) and their brain tissues were swiftly removed on ice. The right frontal cortex tissues were isolated and stored at −80 °C for subsequent immunoblot analysis.
Nissl stainingSerial coronal sections of the ipsilateral frontal cortex were made from posterior to anterior in five rats per group. Each section was 5 μm thick. After conventional dewaxing (in the order of xylene, gradient concentration ethanol, double distilled water), paraffin sections were immersed in cresyl violet staining solution at 56 °C for 60 min. After rinsing double steaming water, Nissl differentiation treatment was performed for approximately 10 s. This differentiation process was repeated until clear cellular differentiation was observed under microscopic examination. Subsequently, the sections were dehydrated, rendered transparent and sealed. Five coronal sections of the M2 area of the ipsilateral frontal cortex were taken from each rat (Fig.1b and c). The images were collected under a microscope with a field of view of ×400 and used to count the Nissl-positive cells with Image J software (NIH, Bethesda, USA). The average count of the five sections from each rat was used for statistical analysis.
Immunohistochemical stainingThe ipsilateral frontal cortex of rats was sectioned coronally from back to front, with a continuous slice thickness of 5 μm per slice. Paraffin sections were dewaxed conventionally, and then treated with 3% H2O2 at 37 °C for 12 min. Microwave repair was conducted for 2 min at high power followed by 12–14 min at low power, followed by natural cooling. Subsequently, a 5% BSA blocking solution at 37 °C for 60 min was applied. Primary antibodies against BDNF (1 : 100, DF6387, Affinity Biosciences, Melbourne, Australia) and IL-6 (1 : 100, DF6087, Affinity Biosciences, Melbourne, Australia) were incubated overnight at 4 °C. Upon rewarming, goat antirabbit IgG at 37 °C for 60 min was applied, followed by strept avidin-biotin complex (37 °C, 60 min) and horseradish peroxidase-diaminobenzidine (HRP-DAB) incubation while avoiding light exposure. After observing cellular characteristics under the microscope and distinguishing clear backgrounds, the sections were washed with running water to remove HRP-DAB and mounted. Five coronal sections of the M2 area of the ipsilateral frontal cortex were taken from the same part of each rat (Fig.1b and c). The images were collected under a microscope with a field of view of ×400. The immunopositive cells were counted using Image J software. The average optical density of the immunopositive products was determined using Image-Pro Plus software (Media Cybernetics, Rockville, USA). The mean value of the five section counts of each rat was used for statistical analysis.
Immunoblot analysisThe tissue specimens from the right frontal cortex were weighed accurately and homogenized following the addition of lysate to extract the total protein content. Molecular weight determination was conducted prior to preparing the gel. Electrophoresis and membrane transfer were performed using 110 V for 100 min after sampling. The membrane was blocked for 120 min, and then incubated with primary antibodies. BDNF (1 : 1000, DF6387, Affinity Biosciences), IL-6 (1 : 1000, DF6087, Affinity Biosciences) and the internal reference, β-actin (1 : 10000, AF7018, Affinity Biosciences) were incubated on a shaker overnight at 4°C. After that, the membrane was incubated with a secondary antibody, specifically goat antirabbit IgG, for 60 min at room temperature. Image acquisition was performed using the ECL developer and Amersham Imager 600 system (GE Healthcare, Chicago, USA). The grayscale values of protein bands were quantified for each experimental group using Image J software.
Statistical analysisSPSS 26.0 statistical software (IBM SPSS Inc.,Chicago, USA) was used for data processing. GraphPad Prism 9 software(GraphPad, Boston, USA) was used to generate statistical graphs. The experimental data were presented as mean ± SD. One-way analysis of variance) was used to analyze comparisons between multiple groups, and Tukey’s honestly significant difference method was used for two-by-two comparisons between groups. Significance was established at P < 0.05.
Results Gastrodin and electroacupuncture mitigate frontal cortex neuron injury in rats with brain ischemiaThe Nissl staining analysis revealed distinct observations within the frontal cortical neurons. Initially, Nissl bodies were characterized by a blue coloration, prominently dispersed within the cytoplasm, exhibiting deeply stained nuclei alongside clear and intact cell structures with a densely arranged configuration (Fig. 2a). In the model group, after inducing postcerebral ischemia, there was a noticeable decrease in Nissl bodies. This reduction correlated with a marked decrease in cell count (204.6 ± 7.83 vs. 65 ± 3.54, P < 0.0001), notable cytoplasmic atrophy and a loosely arranged cellular architecture (Fig. 2b). Following interventions with GAS, EA and their combined application, however, a noteworthy increase in Nissl bodies and the count of Nissl-positive cells compared with the model group was observed (98 ± 5.24 vs. 65 ± 3.54, P < 0.0001; 87 ± 4.85 vs. 65 ± 3.54, P = 0.0002; 126.6 ± 8.38 vs. 65 ± 3.54, P < 0.0001, respectively) (Fig. 2c–f). Concurrently, the treated groups showed a significant improvement in cell morphology. In ischemic brain injury, neurons undergo morphological changes such as unclear nucleus and cytoplasm structure, fragmented nucleus, condensed cytoplasm, disintegrated axon and myelin sheath and ultimately necrosis or apoptosis (Fig. 2b). When EA and GAS are used in combination, they may replace necrotic or apoptotic cells with newborn neuronal cells, gradually restoring clarity to the structure of the nucleus and cytoplasm (Fig. 2e). Furthermore, this treatment can promote synaptic growth and connection of neurons, improving nerve conduction function. Notably, the combination therapy (GAS + EA group) further amplified the cell count compared with the individual GAS and EA treatment groups (Fig. 2f) (126.6 ± 8.38 vs. 98 ± 5.24, P < 0.0001; 126.6 ± 8.38 vs. 87 ± 4.85, P < 0.0001). These findings collectively underscore the potential of GAS and EA interventions in mitigating neuronal damage within the frontal cortex of rats afflicted with cerebral ischemia.
 Fig. 2:
Fig. 2: The histopathological changes in the FC resulting from the combination of gastrodin and electroacupuncture. (a–e) The Nissl staining results for the right FC of rats in each group (red arrows show Nissl-positive neurons, green arrows show damaged neurons, scale bar = 100 μm, n = 5). (f) Comparison of the number of Nissl-positive cells in the right FC of rats in each group. One-way ANOVA was used to analyze the data [F(4,20) = 375.706, P < 0.0001]. The denotation of significance levels is as follows: . ***P < 0.001, ****P < 0.0001. ANOVA, analysis of variance; FC, frontal cortex.
Combined treatment with gastrodin and electroacupuncture upregulates the expression level of the anti-inflammatory factor BDNFThe immunohistochemical product of BDNF, which appeared brownish-yellow, was expressed on the cytoplasm, cytomembrane and protrusions of neurons (Fig. 3a). In the model group, the number of BDNF protein immunopositive cells in the right frontal cortex was reduced compared with the sham group (42.6 ± 2.70 vs. 91.2 ± 3.49, P < 0.0001) (Fig. 3b and f), as was the mean optical density (MOD) of immunopositive products (0.152 ± 0.006 vs. 0.236 ± 0.016, P < 0.0001) (Fig. 3g). Compared to the model group, both the GAS and EA groups showed a significant increase in the positive expression of BDNF protein (42.6 ± 2.70 vs. 72.4 ± 2.70, P < 0.0001 and 42.6 ± 2.70 vs. 71.2 ± 2.39, P < 0.0001) (Fig. 3c, d, f) and an increase in the MOD value of the immunopositive product (0.152 ± 0.006 vs. 0.176 ± 0.011, P = 0.0074 and 0.152 ± 0.006 vs. 0.176 ± 0.004, P = 0.0069) (Fig. 3g). Compared to the GAS or EA groups, the GAS + EA group exhibited a significantly higher number of BDNF immunopositive cells (72.4 ± 2.70 vs. 83.2 ± 2.86, P < 0.0001 and 71.2 ± 2.39 vs. 83.2 ± 2.86, P < 0.0001) (Fig. 3e and f) and a higher MOD value of immunopositive products within the unit area (0.176 ± 0.011 vs. 0.198 ± 0.008, P = 0.0186 and 0.176 ± 0.004 vs. 0.198 ± 0.008, P = 0.0200) (Fig. 3g).
 Fig. 3:
Fig. 3: Effects of gastrodin and electroacupuncture on BDNF expression in the rat FC. (a–e) Immunohistochemistry detected BDNF expression in the right frontal cortical region of rats in each group. BDNF-positive neurons are indicated by red arrowheads (scale bar = 100 μm, n = 5). (f) Statistics on the number of immunopositive cells of BDNF in (a–e) [F(4,20) = 208.717, P < 0.0001]. (g) Statistics on the MOD of BDNF immunopositive products in [F(4,20) = 51.397, P < 0.0001] (a–e). (h) Immunoblot of BDNF protein expression levels in the right FC of rats in each group (n = 5). (i) Comparison of BDNF protein expression levels in (h) [F(4,20) = 344.721, P < 0.0001]. (h) Significant difference in (f, g, i) were denoted as follows: *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001. BDNF, brain-derived neurotrophic factor; FC, frontal cortex; MOD, mean optical density.
In addition, immunoblotting results showed that the protein level of BDNF significantly decreased in the model group compared with the sham group (0.544 ± 0.013 vs. 0.979 ± 0.011, P < 0.0001) (Fig. 3h and i). While in the GAS and EA groups, BDNF protein levels significantly increased compared to the model group (0.754 ± 0.015 vs. 0.544 ± 0.013, P < 0.0001 and 0.852 ± 0.019 vs. 0.544 ± 0.013, P < 0.0001) (Fig. 3h and i). Furthermore, the GAS + EA group exhibited a greater elevation in BDNF protein expression in comparison to the GAS and EA groups (0.894 ± 0.034 vs. 0.754 ± 0.015, P < 0.0001 and 0.894 ± 0.034 vs. 0.852 ± 0.019, P = 0.0286) (Fig. 3h and i).
The expression level of IL-6 decreased in ischemic rats treated with gastrodin and electroacupunctureThis study discovered that the IL-6 protein was expressed in the cytoplasm, cytomembrane and protrusions of neuronal cells, appearing yellowish-brown in color (Fig. 4a). Additionally, the number of IL-6 protein immunopositive cells in the right frontal cortex increased in the model group compared with the sham group (84.8 ± 3.11 vs. 41.4 ± 2.30, P < 0.0001) (Fig. 4b and f). The groups treated with GAS, EA and the combination of GAS and EA showed a decrease in the expression of IL-6 protein (71.6 ± 2.70 vs. 84.8 ± 3.11, P < 0.0001; 75.6 ± 2.30 vs. 84.8 ± 3.11, P = 0.0001 and 65.6 ± 2.07 vs. 84.8 ± 3.11, P < 0.0001) (Fig. 4c–f) and the MOD of immunopositive products within the unit area compared with the model group (0.365 ± 0.015 vs. 0.393 ± 0.008, P = 0.0083; 0.366 ± 0.011 vs. 0.393 ± 0.008, P = 0.0113; 0.342 ± 0.015 vs. 0.393 ± 0.008, P < 0.0001) (Fig. 4g). Moreover, the count of IL-6 immunopositive cells in the GAS + EA group was lower than that in the GAS and EA groups (65.6 ± 2.07 vs. 71.6 ± 2.70, P = 0.0097 and 65.6 ± 2.07 vs. 75.6 ± 2.30, P < 0.0001) (Fig. 4e and f). Furthermore, the MOD of immunopositive products within the unit area was lower in the GAS + EA group (0.365 ± 0.015 vs. 0.342 ± 0.015, P = 0.0344 and 0.366 ± 0.011 vs. 0.342 ± 0.015, P = 0.0258) (Fig. 4g).
 Fig. 4:
Fig. 4: Effects of gastrodin and electroacupuncture on IL-6 expression in the rat FC. (a–e) Immunohistochemistry detected IL-6 expression in the right frontal cortical region of rats in each group (IL-6 positive neurons are indicated by red arrowheads, scale bar = 100 μm, n = 5). (f) Statistics on the number of immunopositive cells of IL-6 in (a–e) [F(4,20) = 208.871, P < 0.0001]. (g) Statistics on the MOD of IL-6 immunopositive products in (a–e) [F(4,20) = 185.946, P < 0.0001]. (h) Immunoblot of IL-6 protein expression levels in the right FC of rats in each group (n = 5). (i) Comparison of IL-6 protein expression levels in (h) [F(4,20) = 57.273, P < 0.0001]. Significant differences in (f, g, i) were denoted as follows: *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001. BDNF, brain-derived neurotrophic factor; FC, frontal cortex; IL-6, interleukin-6; MOD, mean optical density.
The immunoblot analysis revealed an increase in IL-6 protein expression in the model group compared to the sham group, as seen in Figure 4h and i (1.048 ± 0.043 vs. 0.798 ± 0.028, P < 0.0001). The expression level, however, decreased in the GAS, EA and GAS + EA groups compared with the model group (0.857 ± 0.027 vs. 1.048 ± 0.043, P < 0.0001; 0.859 ± 0.029 vs. 1.048 ± 0.043, P < 0.0001; 0.798 ± 0.02 vs. 1.048 ± 0.043, P < 0.0001) (Fig. 4h and i). Additionally, the GAS + EA group showed a greater decrease than either the GAS or EA group (0.798 ± 0.02 vs. 0.857 ± 0.027, P = 0.0442 and 0.798 ± 0.02 vs. 0.859 ± 0.029, P = 0.0348) (Fig. 4h and i). The immunohistochemical results of BDNF and IL-6 indicate that the combined treatment of GAS and EA can effectively rebalance the levels of these two proteins in the right frontal cortex cells of rats with a cerebral ischemia model. This rebalancing effect is superior to that of GAS and EA alone.
DiscussionIn approximately 90% of ischemic stroke patients, middle cerebral artery occlusion is often linked to damage in cortical branches, which affects the sensory and motor regions of the cerebral cortex [10]. Sensory and motor deficits are common clinical manifestations following ischemic stroke, potentially attributable to cortical neuron impairment. Studies have evidenced significant damage in the frontal cortex due to cerebral ischemia [11]. In this study, Nissl staining revealed a substantial reduction in neuron count in the ischemic ipsilateral frontal cortex of model group rats compared with sham-operated ones (Fig. 2b and f).
Research has highlighted the ability of GAS to suppress IL-6 to reduce oxidative stress and inflammatory responses. These mechanisms provide neuronal protection and constitute its pharmacological role in ischemic stroke therapy [12]. Additionally, studies have demonstrated that GAS can effectively decrease hypoxic-ischemic brain damage by regulating the Notch signaling pathway and enhancing Sirt3 in activated microglia [13]. GAS exhibits protective effects against cerebral ischemic injury by facilitating neuronal repair through modulation of neurotransmitters, response to antioxidant stress, inhibition of inflammation and upregulation of neurotrophic proteins [14]. The Nissl staining results from this experiment indicated increased neuronal count in the frontal cortex damaged area after treatment with GAS (Fig. 2c and f), suggesting its potential role in neuronal repair and protection against cerebral ischemia.
Recent research indicates that EA applied to the ST36 and GV20 acupoints can augment the expression of growth arrest-specific 7 and nerve growth factor. This augmentation fosters the differentiation of endogenous neural stem cells into neurons within the injured area, subsequently facilitating cortical neuron regeneration after cerebral ischemia [15]. Additionally, EA targeting the Quchi (LI11) and ST36 points demonstrates the ability to stimulate the synthesis and secretion of BDNF in the ischemic side’s cortex in cerebral ischemia-afflicted rats [16]. Notably, Nissl staining revealed an augmented count of Nissl-positive neurons in the ischemic-side frontal cortex of rats subjected to EA, accompanied by improved neuronal cell morphology compared with the model group (Fig. 2d and f). These findings suggest that EA applied at GV20 and ST36 acupoints contributes to the recovery from cerebral ischemic injury. Furthermore, immunohistochemistry and immunoblotting outcomes underscored that EA treatment in cerebral ischemia rats resulted in heightened BDNF expression (Fig. 3d, f, h and i), which promoted regeneration, and significantly influenced recovery from nerve injury after cerebral ischemia [17].
Combining Chinese medicines has been extensively applied in stroke management, employing a multifaceted approach to ameliorate neurological dysfunction via intricate mechanisms involved in cerebral ischemia [18–20]. Studies have evidenced salvia miltiorrhiza, a Chinese medicine, attenuating neurological impairments in cerebral ischemic rats by curbing microglial polarization toward the M1 type and diminishing the expression of proinflammatory factors such as IL-6 and IL-1β [21]. Microglia represent the initial responders postcerebral ischemia onset, exhibiting dual potential for damage and repair [22]. These activated microglia manifest two phenotypes: the classically activated M1 (proinflammatory) and alternatively activated M2 (anti-inflammatory) states [23]. While M1 microglia release proinflammatory cytokines (e.g. IL-6, IL-1β) aggravating brain injuries, M2 microglia release anti-inflammatory factors such as BDNF and TGF-β, fostering inflammation modulation and neural repair [24,25]. Within this study, Nissl staining showcased that the amalgamation of GAS and EA in cerebral ischemia treatment further diminished the count of impaired neurons on the ischemic side (Fig. 2e and f). This implies that their combination exhibited a synergistic and augmented effect in treating cerebral ischemia by promoting the polarization of activated microglia toward the M2 type, inhibiting their polarization toward the M1 type and then repairing neuronal damage and modulating neuroinflammatory responses by upregulating BDNF (Fig. 3h and i) and downregulating IL-6 (Fig. 4h and i) to play neuroprotective effects. This amalgamated approach might offer a potential clinical target for cerebral ischemia treatment. Additionally, further exploration is necessary to understand the complex molecular mechanism by which GAS combined with EA induces microglial polarization from M1 to M2 type.
ConclusionThe combined therapy of GAS with EA demonstrates a substantial protective effect on frontal cortex injury in rats experiencing cerebral ischemia. This effect likely stems from a synergistic upregulation of anti-inflammatory factors alongside the downregulation of proinflammatory factors, which facilitates the polarization of microglia from the M1 type to the M2 type. The results of this investigation strongly suggest that regulating the neuroinflammatory response may promote neuronal repair and regeneration, offering a potential therapeutic approach for addressing cerebral ischemia.
AcknowledgementsThis research was supported in part by the Key Research Foundation of Wannan Medical College (WK2021Z14 and WK2021Z10), the National Natural Science Foundation of China (82072890 and 31701288), the Mid-Young-Aged Project of Wannan Medical College (WK202219), the Guangzhou City Science and Technology Project (202102010118), the Launch Foundation for High-Level Talent Research at Wannan Medical College (12060201161) and the Natural Science Foundation of Guangdong Province (2020A1515010113).
Z.X.: conceived and supervised the study; M.L., R.G., L.D.: generated reagents and conducted experiment design and execution, data collection and data analysis; Y.Z., X.Y., L.S.: preparation of rats with cerebral ischemia; M.L., Y.Z. and Z.X. wrote and edited the manuscript. All authors read and approved the final manuscript.
The care and procedures for rats in this study were conducted in accordance with the regulations for the use of animals in research, as outlined in the Statutes of the Laboratory Animal Welfare and Ethics Committee of Wannan Medical College, and with local ethical approval.
Conflicts of interestThere are no conflicts of interest.
References 1. Alpua M, Say B, Yardimci I, Ergün U, Kisa U, Ceylan OD. First admission neutrophil-lymphocyte ratio may indicate acute prognosis of ischemic stroke. Rambam Maimonides Med J 2021; 12:e0021. 2. Xiao GR, Tang R, Yang N, Chen YH. Review on pharmacological effects of gastrodin. Arch Pharm Res 2023; 46:744–770. 3. Zhang HY, Zhao YJ, Zhang PJ, Guo MF, Yu JW, Chai Z, et al. Acupuncture ameliorates neurological function by suppressing microglia polarization and inflammatory response after cerebral ischemia in rats. Acupunct Res 2022; 47:941–948. 4. Brigadski T, Leßmann V. The physiology of regulated BDNF release. Cell Tissue Res 2020; 382:15–45. 5. Li Y, Xiang L, Wang C, Song Y, Miao J, Miao M. Protection against acute cerebral ischemia/reperfusion injury by Leonuri Herba Total Alkali via modulation of BDNF-TrKB-PI3K/Akt signaling pathway in rats. Biomed Pharmacother 2021; 133:111021. 6. Kaur S, Bansal Y, Kumar R, Bansal G. A panoramic review of IL-6: structure, pathophysiological roles and inhibitors. Bioorg Med Chem 2020; 28:115327. 7. Longa EZ, Weinstein PR, Carlson S, Cummins R. Reversible middle cerebral artery occlusion without craniectomy in rats. Stroke 1989; 20:84–91. 8. Chan C, Ma T, Wang J, Zhang Y, Gong X. Gastrodin injection alleviates lung injury caused by focal cerebral ischemia in rats through NGF/TrkA pathway- mediated activation of the antiinflammatory pathway. J South Med Univ 2022; 42:116–122. 9. Zhang YM, Xu H, Chen SH, Sun H. Electroacupuncture regulates endoplasmic reticulum stress and ameliorates neuronal injury in rats with acute ischemic stroke. Evid Based Complement Altern Med 2021; 2021:9912325. 10. Yao SQ, Yi W, Liu R, Xu NG. Development of research on mechanisms of electroacupuncture intervention underlying improvement of cerebral ischemia rats in recent five years. Acupunct Res 2019; 44:383–387. 11. Wahul AB, Joshi PC, Kumar A, Chakravarty S. Transient global cerebral ischemia differentially affects cortex, striatum and hippocampus in Bilateral Common Carotid Arterial occlusion (BCCAo) mouse model. J Chem Neuroanat 2018; 92:1–15. 12. Zhang ZL, Gao YG, Zang P, Gu PP, Zhao Y, He ZM, et al. Research progress on mechanism of gastrodin and p-hydroxybenzyl alcohol on central nervous system. China Journal of Chinese materia medica 2020; 45:312–320. 13. Guo J, Zhang XL, Bao ZR, Yang XK, Li LS, Zi Y, et al. Gastrodin regulates the Notch signaling pathway and sirt3 in activated microglia in cerebral hypoxic-ischemia neonatal rats and in activated BV-2 microglia. Neuromolecular Med 2021; 23:348–362. 14. Liu Y, Gao J, Peng M, Meng H, Ma H, Cai P, et al. A review on central nervous system effects of gastrodin. Front Pharmacol 2018; 9:24. 15. Ma TJ, Dong WQ, Zhang YG, Ding J, Wu F. Electroacupuncture increases the expression of Gas7 and NGF in the prefrontal cortex of male rats with focal cerebral ischemia. J Integr Neurosci 2023; 22:63–68. 16. Li SS, Hua XY, Zheng MX, Wu JJ, Ma ZZ, Xing XX, et al. Electroacupuncture treatment improves motor function and neurological outcomes after cerebral ischemia/ reperfusion injury. Neural Regen Res 2022; 17:1545–1555. 17. Guo W, Nagappan G, Lu B. Differential effects of transient and sustained activation of BDNF-TrkB signaling. Dev Neurobiol 2018; 78:647–659. 18. Chang QY, Lin YW, Hsieh CL. Acupuncture and neuroregeneration in ischemic stroke. Neural Regen Res 2018; 13:573–583. 19. Wang ZH, Chen BH, Lin YY, Xing J, Wei ZL, Ren L. Herbal decoction of Gastrodia, Uncaria, and Curcuma confers neuroprotection against cerebral ischemia in vitro and in vivo. J Integr Neurosci 2020; 19:513–519. 20. Liu M, Wang W, Zhang Y, Xu Z. Effects of combined electroacupuncture and medication therapy on the RhoA/ROCK-2 signaling pathway in the striatal region of rats afflicted by cerebral ischemia. Brain Res Bull 2023; 205:110828. 21. Shen HP, Pei HY, Zhai LP, Guan QB, Wang GH. Salvianolic acid C improves cerebral ischemia reperfusion injury through suppressing microglial cell M1 polarization and promoting cerebral angiogenesis. Int Immunopharmacol 2022; 110:109021. 22. Li T, Zhao J, Xie W, Yuan W, Guo J, Pang S, et al. Specific depletion of resident microglia in the early stage of stroke reduces cerebral ischemic damage. J Neuroinflammation 2021; 18:81. 23. Zhao SC, Ma LS, Chu ZH, Xu H, Wu WQ, Liu F. Regulation of microglial activation in stroke. Acta Pharmacol Sin 2017; 38:445–458. 24. Jha MK, Lee WH, Suk K. Functional polarization of neuroglia: implications in neuroinflammation and neurological disorders. Biochem Pharmacol 2016; 103:1–16. 25. Wang J, Xing H, Wan L, Jiang X, Wang C, Wu Y. Treatment targets for M2 microglia polarization in ischemic stroke. Biomed Pharmacother 2018; 105:518–525.
Comments (0)