
Remember me





Healthcare simulation is “a technique that creates a situation or environment to allow persons to experience a representation of a real event for the purpose of practice, learning, evaluation, testing, or to gain understanding of systems or human actions”.1 Beyond education and training, it plays a pivotal role in optimizing healthcare systems, thereby enhancing healthcare delivery, promoting staff well-being and improving patient safety and outcomes.2,3
The dynamics of knowledge sharing and interaction within healthcare communities have evolved significantly in recent years, driven by exponential access to virtual platforms.4 This transformation has heightened awareness of the diverse landscape of simulation practices in healthcare worldwide. This underscores the need for a unified global position on needs, solutions and priorities. A consensus-driven process enabled thoughtful consideration of key variations in conditions and practices, ultimately fostering global alignment on future directions.5
This collaboration, facilitated by the Society for Simulation in Europe (SESAM) and the Society for Simulation in Healthcare (SSH), aims to articulate a global perspective on the current scope of simulation-based practice and gain consensus on future guidance. It emphasizes the crucial role of simulation in enhancing healthcare practices and education, as well as its far-reaching impact. The resulting recommendations aim to promote widespread adoption of simulation practices, benefiting patients and healthcare workforces globally. Policymakers, healthcare organization leaders, health education institutions, and simulation practitioners are the intended recipients of this valuable insight.
A global perspective has been rigorously crafted through extensive and iterative consultation. Representatives from 50 national and international simulation societies and networks distributed across 67 countries were actively engaged in this collaborative effort.
The chosen themes for discussion encompassed key healthcare challenges, the current landscape of simulation use, and ethical considerations within simulation practice. Prior to virtual encounters, relevant questions were emailed, and initial input was thoughtfully provided during structured online meetings during November 2023. All individual contributions were inclusively aggregated through an implicit approach, and emerging themes were summarized into narrative statements and tables.
Consensus on the identified themes was attained during face-to-face meetings held in January 2024. Subsequently, key areas were prioritized through an online survey. The initial draft of this document was produced in February 2024, and then shared with all contributors for peer review. Out of 24 responses, every comment received was thoroughly considered and significantly contributed to the final production of this document.
Current state of simulation practice in healthcareHealthcare simulation finds application across the spectrum of health and care, involving all clinical disciplines and allied professions including dental, mental health and social care. Within this context, simulation practice serves educational and non-pedagogical uses. It encompasses activities such as device, process, system testing, system integration, quality improvement, research and innovative approaches.2,3 Contributions obtained during consultation have highlighted that simulation serves as an adjunct to therapeutic interventions. It is employed in diverse situations, including complex case-by-case surgical planning, aiding pain management during labor, supporting cognitive behavioral therapy in mental health settings and facilitating the training of social skills for autistic patients.
Furthermore, there has been an exponential integration of simulation approaches into quality improvement and patient safety efforts within healthcare teams, departments, and organizations.
Notably, simulation transcends the confines of healthcare systems. It emerges as an excellent public engagement tool and plays a crucial role in multi-agency team preparedness for disaster management.
The value of healthcare simulation is vast and encompasses a wide array of tools and practices. These include, but are not limited to part task trainers, patient simulators (i.e. manikins), cadaveric simulation, and standardized patients or simulated participants portraying patients, relatives, by-standers, and healthcare colleagues. It also includes telesimulation, computer-based simulation, tabletop exercises, data modeling and extended realities including augmented reality, virtual reality, mixed reality, and haptic feedback models. As a community of practice, we provide unique opportunities to learn, rehearse and enhance the wide array of capabilities required to care for all patients, from carrying out simple procedures to managing rare and life threatening situations. We nurture the development of patient-centered communication skills, situational awareness, decision making, team working, leadership and other essential professional behaviors. We continue to innovate and adapt, developing new initiatives according to emerging needs, such as the delivery of packaged simulation materials to students in order to facilitate remote learning during the COVID-19 pandemic. Likewise, this creativity is crucial when supporting healthcare learning in low resource and rural settings, with an increasing use of telesimulation and “pack-and-go” equipment.
Contributions received during the consultation process highlighted the universal challenge of disparities in access to simulation education and resources across geographical areas and socio-economic contexts as well as between different institutions and specialties. Different professions continue to learn within isolated ficient opportunities for interprofessional education, particularly in clinical environments. These inequities result in uneven development of competencies, and are encountered at both undergraduate and postgraduate levels, revealing a clear imperative to integrate simulation into healthcare curricula and into everyday learning opportunities within healthcare organizations.
Additional challenges reported include insufficient standardization of simulation training programmes and inadequate quality assurance of practices, particularly related to assessment and faculty development. A novel challenge arises from the impact of the COVID-19 pandemic on student development. Not only have students experienced reduced exposure to clinical environments, but also to in-person simulation. Consequently, they might initially perceive immersive settings as intimidating.
However, simulation offers global opportunities to support healthcare capabilities. For instance, it aids in preparing health professionals as they enter the workforce. Additionally, simulation helps mitigate skill degradation, especially in the context of high-risk low-frequency situations such as cardiopulmonary resuscitation performance by healthcare personnel or bystanders.
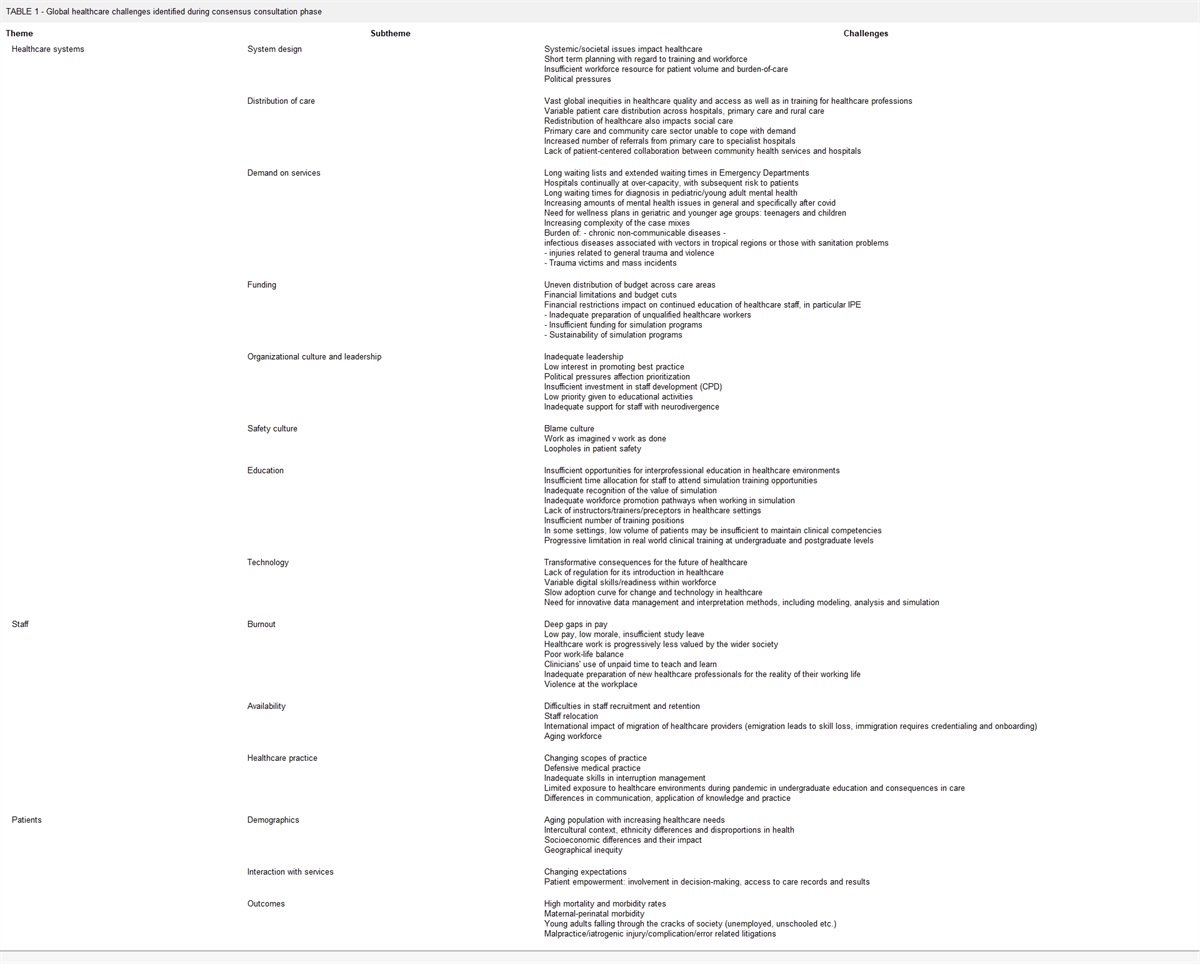
Overcoming healthcare challengesThe consultation process has identified healthcare challenges with a global reach (Table 1). These challenges encompass significant inequalities in access to healthcare and safety culture, extending to education and training for healthcare professions at undergraduate and postgraduate levels. Financial constraints contribute to disparities in healthcare and education, with lower income countries experiencing the most pronounced effects. The consequences of inadequate funding and resource allocation reverberate throughout healthcare systems and culture, limiting the onboarding, upskilling, and continuing education of healthcare staff and teams. Ultimately, these challenges have a negative impact on the workforce, patients, and societies at large.
TABLE 1 - Global healthcare challenges identified during consensus consultation phase Theme Subtheme Challenges Healthcare systems System design Systemic/societal issues impact healthcareThe role of simulated practice in overcoming these challenges is paramount. For example, simulation has demonstrated a positive impact in reducing education inequities, leading to reductions in mortality and morbidity in low-resource areas.6,7 In addition, it supports improvements in patient experiences.8 Simulation interventions contribute to the optimization of healthcare processes and systems, and to organizational safety culture.9–11 They have proven to be cost-effective and successful in enhancing team performance,12 while also fostering workforce well-being and resilience.13,14 It is indisputable that simulation improves healthcare practices, such as central venous catheter placements, leading to a decrease in related infections, and improving patient outcomes.15,16
Simulation can help adapt to the changing demands on healthcare systems, for instance preparing clinicians to manage complexity,17 and supports the development of skills for health and social care professionals in caring for an aging population.18 Additionally, it improves team performance in managing trauma victims and mass casualty disasters.19,20
Other evolving challenges include the ongoing transformation of healthcare practice and education from technological developments. While there is little regulation regarding their introduction, staff digital skills often lag behind, impacting the adoption curve for technological changes in healthcare settings. Regardless, the increasing volume of health data necessitates innovative methods for management and interpretation, including the use of modeling, analysis and simulation.20
Ethical considerationsEthical considerations focus on issues that may be interpreted as “morally right or wrong, just or unjust”.21 These considerations help to ensure that all individuals involved in healthcare simulation are treated and treat others with integrity, respect, empathy, and compassion.
The consultation process revealed a wide array of ethical considerations of importance to the global healthcare community (Table 2). A foundational requirement is to promote equitable access to high-quality healthcare, including dental, mental health, and social care. Simulation complements the development and refinement of caregiving skills, which are essential for all practitioners to deliver the excellent healthcare that every patient deserves. Therefore, global availability of healthcare simulation is an ethical imperative. Concurrently, opportunities for simulation faculty development must be identified globally, with consideration of their affordability in low-resource settings.
TABLE 2 - Ethical considerations in simulation in healthcare provided during the consultation process Theme Considerations Equity of access High quality healthcare including dental, mental health and social care, should be universally accessibleAs with all relevant tools, medicines, and interventions, healthcare simulation must be employed ethically. This includes a commitment to and adherence with common guidelines, such as the standards produced by the International Nursing Association of Clinical Simulation and Learning (INACSL), the Association for Simulated Practice in Healthcare (ASPiH) and the Association of Standardized Patient Educators (ASPE), as well as the Healthcare Simulationist Code of Ethics.22–25
Encouraging and fostering a shared safety culture mindset is critical. This ensures the psychological and physical safety of all participants, protects personal and patient information, and removes “blame and shame” feedback from learning and operational culture.23 Furthermore, learners should be supported in the process of experiential learning with integrity and transparency, and in accordance with best practices.25
Diversity, equity, inclusion, and accessibility principles are essential in simulation and healthcare practice.26 By intentionally integrating these principles, we create a more culturally competent and responsive environment. Teams, institutions, and broader healthcare contexts must actively manage complex cultural relationships. Additionally, fostering equitable collaborative partnerships across all levels of care and education is crucial.
While incorporating advancing technologies into healthcare simulation is valuable, it is equally important to proceed judiciously. We should minimize potential unforeseen negative learning outcomes by carefully evaluating and implementing these innovations.
As fellow stewards of the planet, we bear a collective responsibility. Encouraging a shared mindset of sustainability and conservation is imperative.27
RecommendationsThe global consultation process has yielded several key themes for recommendations (Table 3). The subsequent recommendations aim to provide alignment and direction to simulation professionals, healthcare systems, healthcare education institutions, and global leaders.
First and foremost, it is necessary to advocate for the benefits that simulation brings to patients, staff and organizations. Promoting its adoption and integration into daily learning and practice across the entire spectrum of healthcare is essential. Beyond enhancing care providers' and teams' performances, simulation can also empower patients by providing new perspectives and fostering necessary responsibilities and beneficial behaviors, ultimately leading to improved patient outcomes.
Political, strategic and financial support at an institutional and governmental level is vital. Ensuring the sustainability of simulation facilities, programmes, and workforce requires concerted efforts and commitment.
Exploring low-cost high-impact simulation methods can expand its use throughout the training continuum. Particularly in interprofessional learning contexts, such approaches can be transformative. Simultaneously, integrating simulation into system improvement processes as well as undergraduate and postgraduate curricula, should follow a collaborative, prudent approach based on best practices.
There is a global agreement that simulation must be used appropriately. To enhance its effectiveness, we propose several key strategies:
Development and use of evidence-based tools to ensure the quality of healthcare practice. These tools should be aligned with recognized standards of best practice and evolve alongside simulation methodologies. Invest in faculty development to enhance their expertise in simulation practice. Rigorously evaluate all simulation activities to maintain quality standards. Establish quality-assured approaches for accrediting, credentialing, and certifying (and recertifying) simulation programs and practitioners Provide equitable access to high-quality, contextually relevant simulation-based learning opportunities. To achieve this, it is critical to cultivate the support necessary to ensure consistent resourcing for healthcare simulation. Leverage telesimulation and virtual approaches to facilitate accessibility across the spectrum of professions and practice, including rural, remote and low-income areas. Uphold the principles of equity, diversity and inclusion both within and via simulation. Be mindful of the environmental impact of simulation activities. Encourage a renewed emphasis on research and scholarship in order to progress as a community of practice. Focus on simulation-specific initiatives and explore novel ways to integrate simulation into broader healthcare research and innovation. Call for actionHealthcare simulation serves a greater purpose beyond its own existence. Its mission is to elevate the performance of healthcare providers, teams and systems, ultimately leading to improved health outcomes for patients, communities, and societies. To achieve this transformative impact, it will require a concerted effort by leaders and policymakers, healthcare systems, healthcare education institutions, and simulation practitioners to promote and enhance this critical capability as a means of improving patient outcomes across the globe.
To this end, we propose several key actions:
We propose that policymakers and leaders formally acknowledge and embrace the benefits of simulation in healthcare practice and education, which ultimately enhance patient outcomes by:
Committing sustained resources to simulation. Mandating the use of simulation within education, training, and clinical environments. Being explicit in how simulated experiences may augment or replace clinical experiences for learners in residency and pre-licensure status.We recommend that healthcare systems and healthcare education institutions commit to the goal of high-quality healthcare and improved patient outcomes by:
Promoting healthcare simulation as a critical and necessary learning tool throughout all phases and levels of a caregiver's career. Providing the necessary resourcing for healthcare simulation, including staff, equipment, space, and curricular context. Using healthcare simulation to create interprofessional education and training opportunities. Fostering and adhering to healthcare simulation best practice standards. Cultivating simulation-capable faculty and mentors.We call on simulation practitioners to:
Promote healthcare simulation as a critical learning tool. Adhere to best practice standards. Perform to the highest levels of personal integrity and ethical behavior. Commit to lifelong learning. Persist in their fervent advocacy for patient safety.We hope that this global statement contributes to increasing the visibility of simulation in healthcare, and guides the coordination of simulation and healthcare strategies and policies worldwide.
Authors' contributionsWe wish to acknowledge all societies and networks that have contributed to this document and the individuals who have represented their perspectives: African Simulation Network, Jo Park-Ross; Asociación de Simulo-Educadores de Puerto Rico (ASEPUR), Widalys González-Ortiz; Association for Simulated Practice in Healthcare (ASPiH), Colette Laws-Chapman; Association of Standardized Patient Educators (ASPE), Lou Clark and Shawn Galin; Australian Society for Simulation in Healthcare (ASSH), Kellie Britt and Belinda Judd; Brazilian Society of Simulation in Healthcare, Carolina Felipe Soares Brandão, Jose Roberto Generoso Junior and Itamar Magalhaes; Canadian Alliance of Nurse Educators using Simulation, Jane Tyerman; Canadian Simulation Network, Timothy Willett; China Medical Education Association, Li Li; Comité Internacional de Colaboración Científica entre asociaciones de Simulación (CICCAS), Andres Diaz-Guio; Deutsche Gesellschaft zur Förderung der Simulation in der Medizin, Marcus Rall and Stephan Prückner; Dutch Society for Simulation in Healthcare (DSSH), Ulrich Strauch; European Society for Artificial Organs (ESAO), Frank R. Halfwerk; European Society of Anaesthesiology and Intensive Care (ESAIC), Crina Burlacu; Extracorporeal Life Support Organization (EuroELSO), Frank R. Halfwerk; Federación Latinoamericana de Simulación Clínica y Seguridad del Paciente, Andres Diaz-Guio; Finnish Simulation Network (FinnSim), KirsiMarja Metsavainio; Global Network for Simulation in Healthcare, Lennox Huang and Pam Jeffries; Healthcare Simulation Users Network in Turkey, G. Ulufer Sivrikaya; Hong Kong Society for Simulation in Healthcare, Albert Chan; International Network for Simulation-based Pediatric Innovation, Research and Education (INSPIRE), Tensing Maa and Kimberly Stone; International Nursing Association for Clinical Simulation and Learning (INACSL), Desiree Diaz, Laura Gonzalez, and Ashley Franklin; International Pediatric Simulation Society (IPSS), Justin Jeffers and Kimberly Stone; Irish Association for Simulation, Crina Burlacu and Paul O'Connor; Japan Association for Simulation-based Education in Healthcare Professionals, Ichiro Kaneko; Malaysian Society for Simulation in Healthcare (MaSSH), Zaleha Mahdy, Ismail Mohd Saiboon and Thiruselvi Subramaniam; New Zealand Association for Simulation in Healthcare (NZASH), Brad Peckler: Pakistan Simulation Network, Faisal Ismail; Pan Asia Society for Simulation in Healthcare (PASSH), Ashokka Balakrishnan and Sayaka Oikawa; Pediatric Simulation Training and Research Society (PediSTARS), Geethanjali Ramachandra: Polish Society of Medical Simulation, Marek Dabrowski, Gregorz and Aleksandra Steliga; Portuguese Society for Simulation Applied to Health Sciences (SPSim), Gustavo Norte; RegSim Vest, Sigrun Qvindesland; Saudi Society of Simulation in Healthcare (SSSH), Abdulaziz M. A. Boker; Sociedad Argentina de Simulación (SASIM), Carla Prudencio; Sociedad Chilena de Simulación Clínica (SOCHISIM), Soledad Armijo-Rivera and Mario Zuniga; Sociedad Dominicana Simulación Clínica (SODOSICLI), Pablo C. Smester; Sociedad Ecuatoriana de Simulación en Ciencias de la Salud para Seguridad del Paciente, Betty Bravo; Sociedad Española de Simulación Clínica y Seguridad del Paciente (SESSEP), Aida Camps-Gómez; Sociedad Mexicana de Simulación en Ciencias de la Salud, Edgar Israel Herrera Bastida; Società Italiana di SIMulazione in MEDicina (SIMMED), Pier Luigi Ingrassia; Société Francophone de Simulation en Santé (SoFraSimS), Dan Benhamou and Fouad Marhar; Society for Simulation Applied to Medicine of Moldova, Andrei Romancenco; Society for Simulation in Europe (SESAM), Francisco Maio Matos, Pier Luigi Ingrassia and Doris Ostergaard; Society for Simulation in Healthcare (SSH), Barry Issenberg and Jayne Smitten; Swedish Association for Clinical Training and Medical Simulation (KlinSim), Magnus Berndtzon; The Gathering of Healthcare Simulation Technology Specialists (SimGHOSTS), Yixing Chen and Erica Hinojosa; Ukrainian Simulation Network, Halyna Tsymbaliuk; Victorian Simulation Alliance, Debra Nestel; Vital Anaesthesia Simulation Training (VAST), Adam Mossenson.
Declarations Competing interestsCDN is the Chair of the Board of Trustees at the TALK Foundation, Chair of the Scientific Committee for SESAM - the Society for Simulation in Europe, and a member of the executive committee at the Association for Simulated Practice in Healthcare (ASPiH).
RA is a Past President of the Society for Simulation in Healthcare, and Chair of the Global Advocacy Task Force, Society for Simulation in Healthcare. RA has an equity stake serves in an unsalaried role as the Director of Simulation and Technology in eTrainetc, LLC, a healthcare simulation company.
MC is Secretary of the Board of Directors of the Society for Simulation in Healthcare. He is Past Secretary and Member of the Board of Directors for SimGHOSTS. MC provides consulting services as a contractor to CAE Healthcare for simulator and center design.
KJF is Secretary of SESAM - the Society for Simulation in Europe, and is an Associate Editor of the International Journal of Healthcare Simulation.
SBLK is Vice Treasurer, Pan Asia Simulation Society in Healthcare.
GR is Editor-in-Chief of Advances in Simulation.
JS is Immediate Past President of the Society for Simulation in Healthcare, and an Editorial Board Member of Quality Advancement in Nursing Education (QANE)—Avancées en formation infirmières.
PLI is President-Elect of SESAM—the Society for Simulation in Europe, Immediate Past-President of Società Italiana di SIMulazione in MEDicina (SIMMED), and co-founder and editorial director of SIMZINE.
FMM is President of SESAM - the Society for Simulation in Europe, and Chair of the European Society of Anaesthesiology and Intensive Care (ESAIC) Connectivity Taskforce.
BI is Professor of Medicine and Director of the University of Miami Michael S Gordon Center for Simulation and Innovation in Medical Education. The University of Miami has agreements with Laerdal Medical and the American Heart Association to develop and disseminate simulation-based training programs. Any associated revenue is directed back to the University of Miami. No personal income or royalty is realized by the individual. BI is the current President of the Society for Simulation in Healthcare.
References 1. Healthcare Simulation Dictionary -Second Edition Rockville, MD: Agency for Healthcare Research and Quality; September 2020. AHRQ Publication No. 20-0019. https://doi.org/10.23970/simulationv2. 2. Nickson CP, Petrosoniak A, Barwick S, Brazil V. Translational simulation: from description to action. Adv Simul. 2021;6:1–1. 3. Weldon SM, Buttery AG, Spearpoint K, Kneebone R. Transformative forms of simulation in health care-the seven simulation-based'I's: a concept taxonomy review of the literature. Int J Healthcare Simul. 2023:1–3. 4. Slater BJ, Kashyap MV, Calkins CM, Powell D, Rothstein DH, Clifton M, Pandya S. Global dissemination of knowledge through virtual platforms: Reflections and recommendations from APSA/IPEG. J Pediatr Surg. 2022;57(9):124–129. 5. Murphy MK, Black NA, Lamping DL, McKee CM, Sanderson CF, Askham J, Marteau T. Consensus development methods, and their use in clinical guideline development. Health Technol Assessment (Winchester, England). 1998;2(3):i–88. 6. Mduma E, Ersdal H, Svensen E, Kidanto H, Auestad B, Perlman J. Frequent brief on-site simulation training and reduction in 24-h neonatal mortality—an educational intervention study. Resuscitation. 2015;1(93):1–7. 7. Nelissen E, Ersdal H, Mduma E, Evjen-Olsen B, Twisk J, Broerse J, van Roosmalen J, Stekelenburg J. Clinical performance and patient outcome after simulation-based training in prevention and management of postpartum haemorrhage: an educational intervention study in a low-resource setting. BMC Pregnancy Childbirth. 2017;17(1):1–9. 8. van Tetering AA, Ntuyo P, Martens RP, Winter N, Byamugisha J, Oei SG, Fransen AF, van der Hout-van MB. Simulation-based training in emergency obstetric care in sub-Saharan and Central Africa: a scoping review. Ann Global Health. 2023;89(1). 9. Ajmi SC, Advani R, Fjetland L, Kurz KD, Lindner T, Qvindesland SA, Ersdal H, Goyal M, Kvaløy JT, Kurz M. Reducing door-to-needle times in stroke thrombolysis to 13 min through protocol revision and simulation training: a quality improvement project in a Norwegian stroke centre. BMJ Qual Saf. 2019;28(11):939–948. 10. Brazil V, Purdy E, Bajaj K. Simulation as an improvement technique. Cambridge University Press; 2023. 11. Schram A, Paltved C, Lindhard MS, Kjaergaard-Andersen G, Jensen HI, Kristensen S. Patient safety culture improvements depend on basic healthcare education: a longitudinal simulation-based intervention study at two Danish hospitals. BMJ Open Quality. 2022;11(1):e001658. 12. Ajmi SC, Kurz MW, Ersdal H, Lindner T, Goyal M, Issenberg SB, Vossius C. Cost-effectiveness of a quality improvement project, including simulation-based training, on reducing door-to-needle times in stroke thrombolysis. BMJ Qual Saf. 2022;31(8):569–578. 13. Sullivan J, Al-Marri A, Almomani E, Mathias J. The impact of simulation-based education on nurses' perceived predeployment anxiety during the COVID-19 pandemic within the cultural context of a middle eastern country. J Med Educ Curric Dev. 2021;8:23821205211061012. 14. Madrigano J, Chandra A, Costigan T, Acosta JD. Beyond disaster preparedness: Building a resilience-oriented workforce for the future. Int J Environ Res Public Health. 2017;14(12):1563. 15. Barsuk JH, Cohen ER, Potts S, Demo H, Gupta S, Feinglass J, McGaghie WC, Wayne DB. Dissemination of a simulation-based mastery learning intervention reduces central line-associated bloodstream infections. BMJ Qual Saf. 2014;23(9):749–756. 16. Barsuk JH, Cohen ER, Feinglass J, McGaghie WC, Wayne DB. Use of simulation-based education to reduce catheter-related bloodstream infections. Arch Intern Med. 2009;169(15):1420–1423. 17. Gormley GJ, Fenwick T. Learning to manage complexity through simulation: students' challenges and possible strategies. Perspect Med Educ. 2016;5:138–146. 18. Eost-Telling C, Kingston P, Taylor L, Emmerson L. Ageing simulation in health and social care education: A mixed methods systematic review. J Adv Nurs. 2021;77(1):23–46. 19. McLaughlin C, Barry W, Barin E, Kysh L, Auerbach MA, Upperman JS, Burd RS, Jensen AR. Multidisciplinary simulation-based team training for trauma resuscitation: a scoping review. J Surg Educ. 2019;76(6):1669–1680. 20. Murray RE, Ryan PB, Reisinger SJ. Design and validation of a data simulation model for longitudinal healthcare data. InAMIA Annual Symposium Proceedings 2011. Am Med Info Assoc. 2011:1176. 22. Watts PI, Rossler K, Bowler F, Miller C, Charnetski M, Decker S, Molloy MA, Persico L, McMahon E, McDermott D, Hallmark B. Onward and upward: introducing the healthcare simulation standards of best PracticeTM. Clin Simul Nurs. 2021;1(58):1–4. 23. Diaz-Navarro C, Laws-Chapman C, Moneypenny M, Purva M. The ASPiH Standards - 2023: guiding simulation-based practice in health and care [cited 2024 Feb 25]. Available from https://aspih.org.uk. 24. Lewis KL, Bohnert CA, Gammon WL, Hölzer H, Lyman L, Smith C, Thompson TM, Wallace A, Gliva-McConvey G. The association of standardized patient educators (ASPE) standards of best practice (SOBP). Adv Simul. 2017;2(1):1–8. 25. Healthcare Simulationist Code of Ethics, [cited 2024 Feb 25]. Available from https://www.ssih.org/SSH-Resources/Code-of-Ethics. 26. Purdy E, Symon B, Marks RE, Speirs C, Brazil V. Exploring equity, diversity, and inclusion in a simulation program using the SIM-EDI tool: the impact of a reflexive tool for simulation educators. Adv Simul. 2023;8(1):11. 27. NaynaSchwerdtle P, Horton G, Kent F, Walker L, McLean M. Education for sustainable healthcare: a transdisciplinary approach to transversal environmental threats. Med Teach. 2020;42(10):1102–1106.
Comments (0)