
Remember me
The current study compared the rate of RAV localization on pre-AVS CT imaging to the rate of RAV localization during AVS. As demonstrated on prior studies, localization of the RAV on pre-AVS CT aids the proceduralist by providing a range of potential locations for the RAV during AVS [13,14,15,16]. Interventional radiologists will typically begin searching for the RAV at T11 and then probe the IVC for 2 vertebral bodies in the cranial and caudal directions. Our study demonstrates that the range of potential RAV locations during AVS can be be further refined when its position is identified on pre-AVS CT. Specifically, we found that the RAV localized within 3 levels (for purposes of our study a level was defined as a third of a vertebral body or disk space) cranial to the location identified on pre-AVS CT imaging in 98.1% of cases. While the location of the RAV on pre-AVS CT imaging and fluoroscopy is not exact, the more limited search area to probe the IVC for the RAV orifice may facilitate decreased procedure time, radiation exposure, and contrast dose. Furthermore, we postulate that our finding that the localization of the RAV within 3 levels cranial to the location found on pre-AVS CT imaging may be secondary to the differences in respiration during pre-AVS CT imaging and AVS. Specifically, CT imaging is performed during mid-expiration compared to imaging during AVS when the patient is most often in the expiratory phase of respiration. The different pattern of respiration and the degree of sedation may account for the observed differences in localization. Another potential benefit of accurate identification of the RAV using pre-AVS CT images is to aid the proceduralist with the axis of orientation of the RAV, which may be directed in the posterior, posterolateral, or lateral positions relative to the IVC.
This study underscores the importance of pre-AVS CT imaging. While no significant difference in successful RAV cannulation during AVS were observed when the RAV orifice was identified on pre-AVS CT imaging, it is possible that these results are confounded by the utilization of intraprocedural CT in only 64 (51.6%) of 124 AVS procedures during the study period. As evidence of the importance of pre-AVS identification of the RAV on CT imaging, the rate of successful RAV catheterization in our patient cohort was low (51.5%; n = 17 of 33 procedures) when both of the following conditions were met: (1) pre-AVS CT imaging failed to demonstrate the RAV and (2) intraprocedural CT was not performed. The main benefit of pre-AVS identification of the RAV orifice is to pinpoint the potential area of the IVC from which the RAV originates. While not specifically assessed in this retrospective review, we surmise that limiting the range in which the RAV may originate may help to decrease fluoroscopy and procedure times during AVS.
At our institution, we utilize a specific CT imaging protocol to aid in visualization of the RAV. Prior studies have shown that the RAV is best visualized on CT using thin-slice reconstructions (0.5–0.75 mm slice thickness) and imaging during multiple phases of contrast enhancement (i.e., arterial, “late” arterial [10–15 s after the initial scan], venous [70 s after the initial scan], and delayed [3 min after the initial scan] phases) [14, 23]. The importance of a specific protocol for imaging of the adrenal glands and veins is important for two reasons: to facilitate identification of the RAV for AVS and to aid the surgeon with a priori identification of RAV aberrations (e.g., duplicated RAV or < 1 cm RAV length) that may facilitate posterior retroperitoneoscopic adrenalectomy.
This study supports previous findings of the utility of intra-procedural CT during AVS [17,18,19,20,21]. The rate of successful RAV sampling increased from 63.9 to 93.8% when catheter position was confirmed by intraprocedural CT acquired after contrast administration through the catheter placed into the RAV (P < 0.01). CBCT was used for 27 (42.2%) of 64 intraprocedural CT scans and MDCT was used in 37 (57.8%) of 64 AVS procedures. While no correlation between the type of intra-procedural CT scan used and the subsequent success of RAV catheterization was observed, there are practical differences between CBCT and MDCT. First, CBCT is limited by a relatively long acquisition time, typically 6 s, as opposed to MDCT, which had an image acquisition time of approximately 1–2 s for a comparable image volume. The long acquisition time may lead to artifacts from respiratory motion, especially if the patient is sedated as minimal or moderate sedation can impact the depth of the respiratory cycle. Second, higher available radiation output in MDCT offers flexibility in positioning of the patient’s arms. The patient’s arms were raised above their head during CBCT while the patient’s arms remained by their side during MDCT. Considering the RAV’s short length and small diameter, these arm movements during CBCT can lead to dislodgement of the catheter used to cannulate the RAV during image acquisition. Finally, the tip of the catheter used to cannulate the RAV is radiopaque to improve visualization during fluoroscopy. The radiopacity of the tip, however, causes streak artifacts in CBCT images. Streak artifacts are less severe in MDCT compared to CBCT owing to increased angular sampling and reduced beam hardening, facilitating accurate identification of the RAV during AVS (Fig. 2).
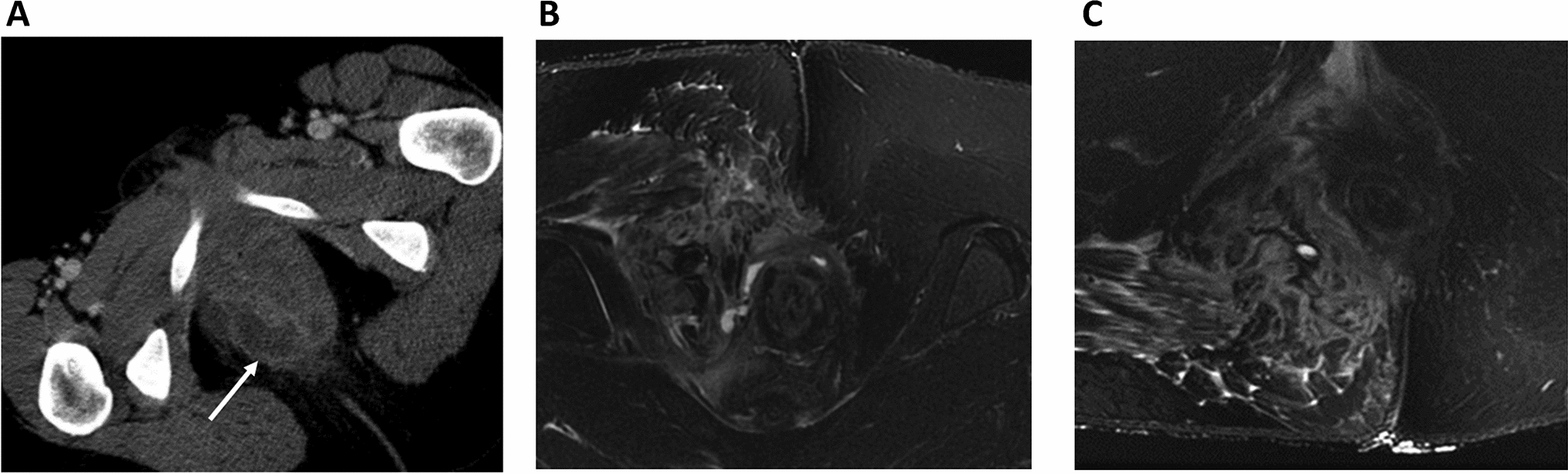
Fig. 2
Intraprocedural CT images of the RAV during AVS. a 65-year-old male was referred for AVS. Axial image from an intraprocedural CBCT scan showing the RAV (thin arrow). Steak artifact is caused by the radiopaque marker at the tip of the C2 catheter (thick arrow) which is used to cannulate the RAV. b Coronal reconstruction demonstrates the C2 catheter (thick arrow) and faint contrast within the medial limb of the right adrenal gland (thin arrow). c 59-year-old male was referred for AVS. Axial image from MDCT demonstrates the RAV (thin arrow). While the tip of the C2 catheter (thick arrow) is radiopaque, the degree of streak artifact is less pronounced than on CBCT. d Coronal reconstruction demonstrates contrast clearly opacifying the entirety of the adrenal gland (thin arrow). RAV right adrenal vein, AVS adrenal venous sampling, CBCT cone-beam CT, C2 Cobra-2, MDCT multidetector CT
This study has the following limitations. First, this study was retrospective with its attendant biases. Operators at our institution place an emphasis on high-quality pre-AVS CT imaging as well as performing intraprocedural CT whenever the technology is available in the procedural suite. The predisposition of our practice to emphasize pre-AVS and intraprocedural CT imaging may introduce a bias towards detecting a difference. Second, the success rates of AVS procedures increased over time. The importance of physician experience for the success rate of RAV catheterization cannot be overstated. The protracted time frame of this study (22 years) introduces a confounding effect of increasing operator experience. It should be noted, however, that one of the most difficult aspects of successful RAV catheterization during AVS is the wide variation in radiographic appearance [8]. Our experience was that intra-procedural CT served to expedite the learning curve for interventional radiologists during their early experience, introducing them to the different radiographic appearances of the RAV. Third, the pre-AVS CT imaging evaluated in this study was conducted at various institutions. Prior studies have evaluated the accuracy of CT imaging in depicting the RAV. Fourth, most intraprocedural CT images were acquired using MDCT, which provides superior contrast and temporal resolution compared to CBCT. While other studies have described similar improvements with successful RAV catheterization when using CBCT, our results should be interpreted with the caveat that a MDCT imaging was used in most of the procedures in which the RAV was successfully cannulated during AVS.
Our findings corroborate the utility of pre-AVS CT imaging and intra-procedural CT imaging to facilitate successful RAV sampling during AVS. Given the high prevalence of hypertension and the suspected underdiagnosis of PA, utilization of AVS will likely increase. Success of the procedure is primarily contingent upon cannulation of the RAV. This work also provides a CT-guided roadmap for improving the success of AVS.
Comments (0)