
Remember me


Mean (± SE) values for kinematic and EMG during BEFORE, MOVING and AFTER trials are presented in Figs. 2 and 3, respectively. Grand averages for all outcomes for mean BEFORE and the first AFTER trial are presented in Fig. 4A (Control group) and 4B (CBL group).
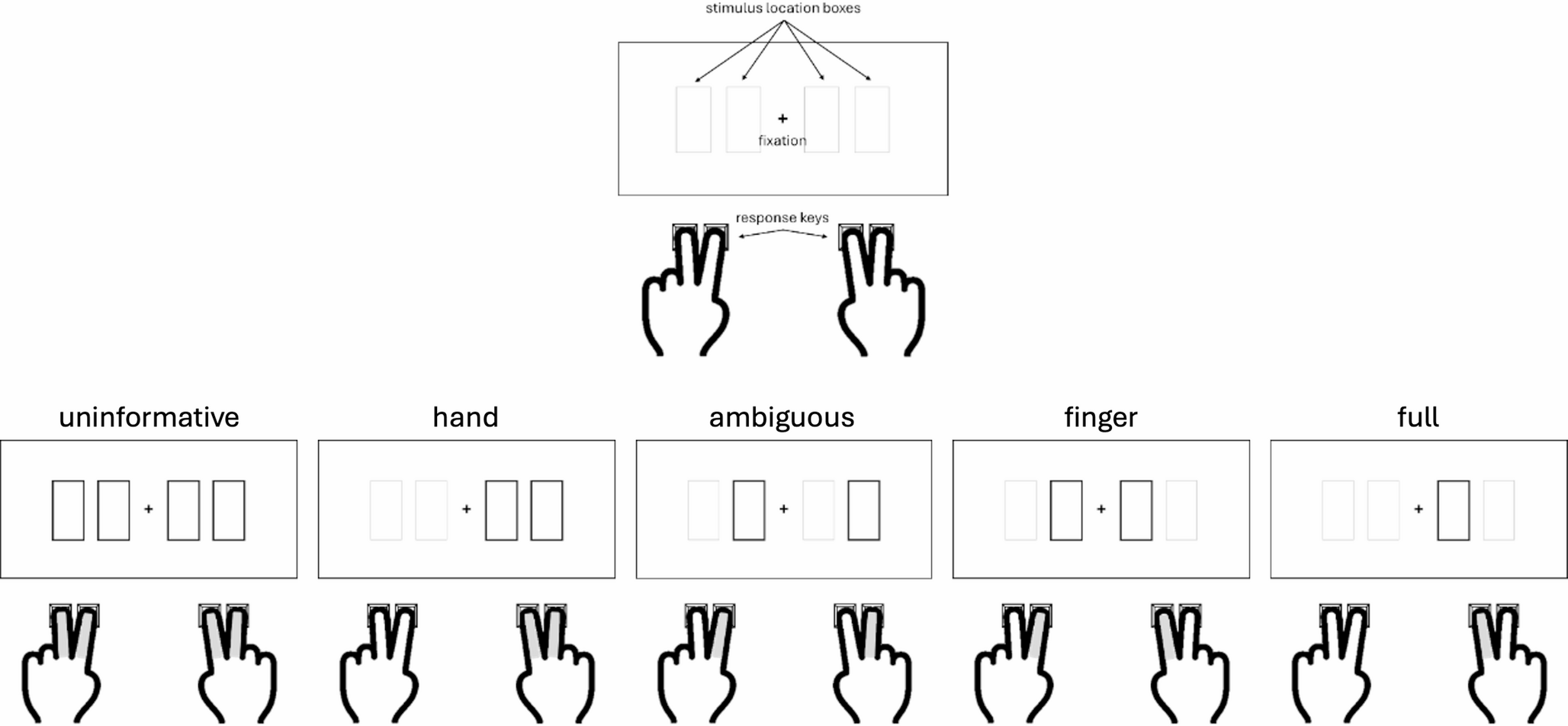
Fig. 2
Group kinematic data (mean ± SE) during mean BEFORE (left panel), MOVING (middle panel; gait velocity only) and AFTER (right panel) conditions for gait approach velocity (Fig. 2A) and trunk sway (Fig. 2B). Numbers along the x-axis represent trial numbers. Group data for the cerebellar patients (CBL; closed squares) and controls (white circles) are represented. Note, due to the very low SE values for trunk sway in BEFORE trials (for both groups), SE bars do not extend beyond the outer-limits of the squares/circles during BEFORE. Due to the criteria used to calculate trunk overshoot, it is not possible to calculate this outcome during MOVING trials and hence these data are omitted from analysis
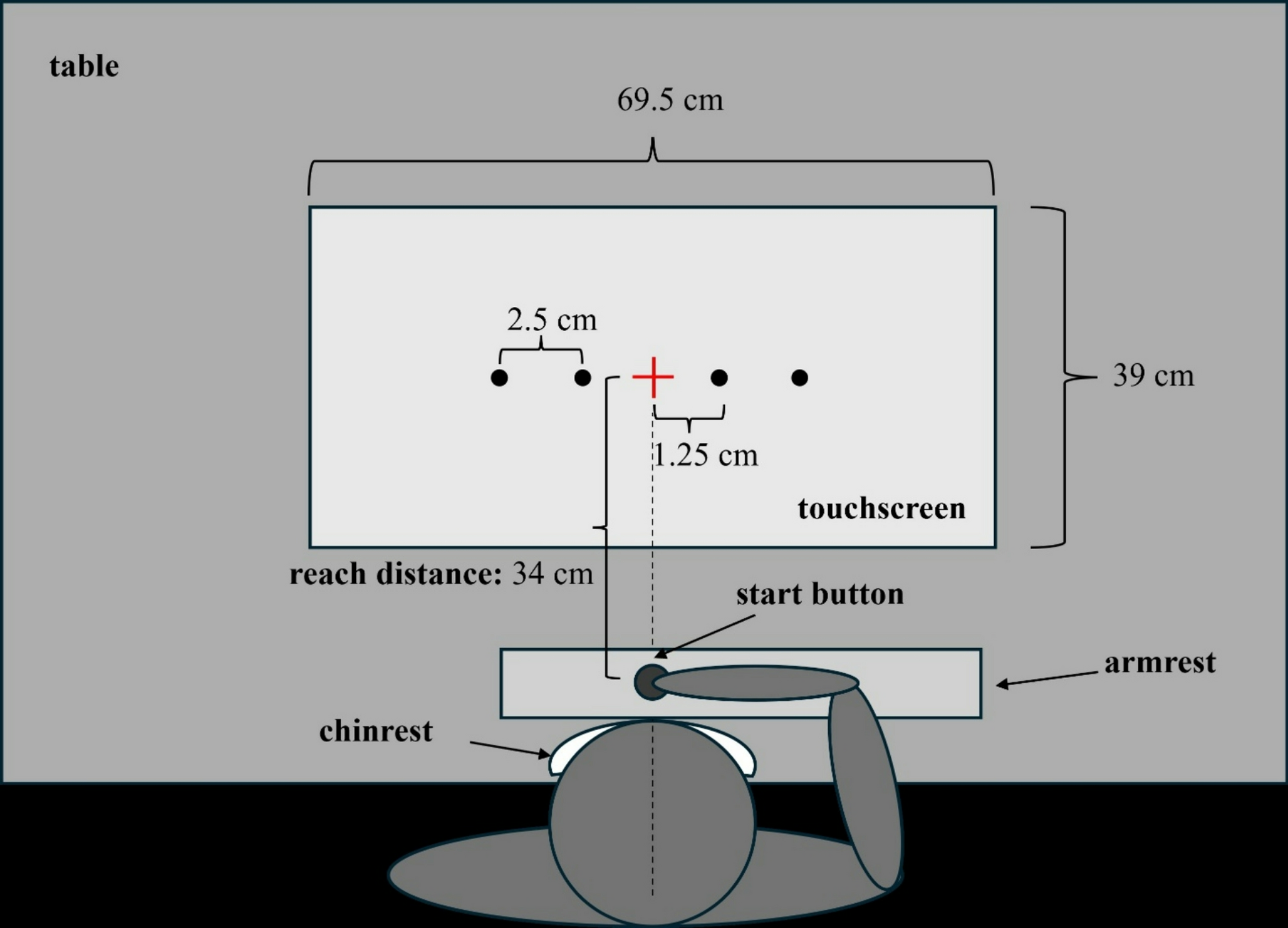
Fig. 3
Normalised (to mean BEFORE) group electromyographic (EMG) data (mean ± SE) during MOVING and AFTER conditions for the contact leg tibialis anterior (TA; Fig. 3A) and medial gastrocnemius (MG; 3B). Numbers along the x-axis represent trial numbers. Group data for the cerebellar patients (CBL; closed squares) and controls (white circles) are represented. The lack of an EMG aftereffect in the patients is best seen in the contact leg MG.
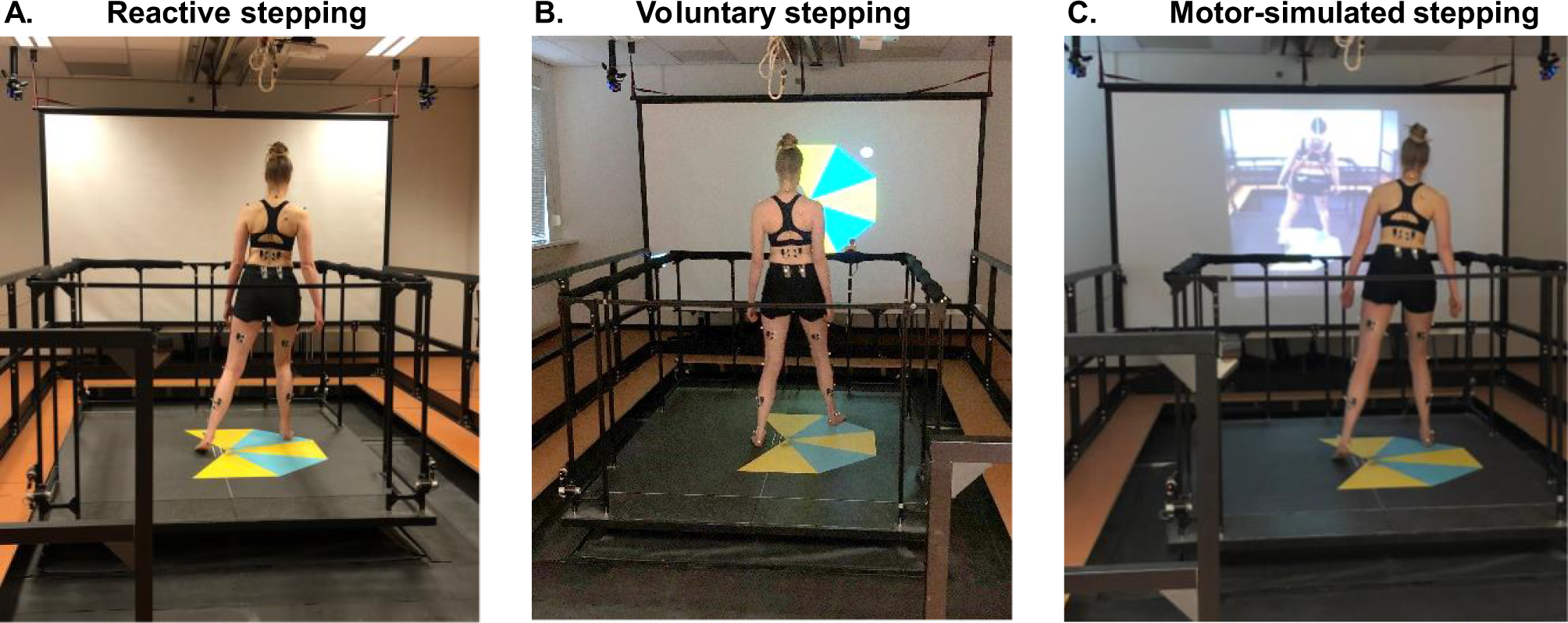
Fig. 4
Grand averaged of control (Fig. 4A) and cerebellar patients’ (CBL; Fig. 4B) data of movement and EMG responses during mean BEFORE (grey shaded area) and first AFTER trial (i.e., the aftereffect; solid line). The blank area delineated between the solid line and the grey area is a visual representation of the aftereffect magnitude – note the smaller ‘blank’ area (see arrows) for the CBL group as compared to the control subjects with respect to the contact leg medial gastrocnemius (MG) electromyographic (EMG) activity.
Before comparisonsWhilst gait approach velocity tended to be lower in the CBL patients during BEFORE trials, this difference was not statistically significant (Z=-1.54, p = .123). CBL patients did, however, have statistically greater trunk sway post foot contact during BEFORE trials (Z=-2.32, p = .021) – indicating greater postural instability following gait termination.
Regarding EMG, there were no statistically significant between-group differences for either contact leg MG (Z=-0.91, p = .364) or TA activity (Z=-1.31, p = .190).
Before-to-moving comparisons – gait approach velocityThere was a clear pattern of increased gait approach velocity during the first MOVING trial for Control participants (mean 33.4% increase), whilst the CBL group showed increases of around half this magnitude (mean 15.4% increase). Indeed, whilst there was a significant main effect of both group (χ2 = 5.87, p = .015) and trial (χ2 = 41.16, p < .001), the significant interaction effect (χ2 = 7.21, p = .007) and subsequent Bonferroni post-hocs revealed that the increase in gait velocity from BEFORE to MOVING-1 was significant for the Control group only (p < .001; CBL group, p = .104). These results remained when controlling for treadmill speed (see Supplementary Materials).
Before-to-moving comparisons – EMGWith respect to contact leg TA (the muscle activity required to arrest a backwards fall after stepping onto the moving treadmill), both groups showed a significant increase from BEFORE to MOVING-1, although this increase tended to be larger for the Control group: There was a significant main effect of trial (χ2 = 61.58, p < .001), a near significant effect of group (χ2 = 3.76, p = .052), and a significant interaction between the two (χ2 = 5.32, p = .021). Post-hoc tests revealed that EMG activity in contact leg TA significantly increased from BEFORE to MOVING-1 in both groups (Control: p < .001, CBL: p = .002). Whilst the increase in contact leg TA activity tended to be larger for the Control group, this was not statistically significant (p = .194). Due to the forwards-moving treadmill causing participants to fall backwards, the MG has a reduced role in maximising postural stability during MOVING trials. Indeed, there was limited significant change between BEFORE and MOVING-1 for either group with respect to contact leg MG activity: There was neither a significant main effect of group (χ2 = 0.84, p = .772) nor trial (χ2 = 1.91, p = .167), nor a significant interaction (χ2 = 1.51, p = .220).
When controlling for treadmill speed, the key patterns of results remained; however, the increase in contact leg TA activity during MOVING-1 was now significantly larger for the Control group (p = .047), suggesting an impairment in reactive neuromuscular control for patients with cerebellar damage. Please see Supplementary Materials for the full results from the covariate analysis.
Early-to-late Moving ‘adaptation’ trials – gait approach velocityThere was a main effect of both group (χ2 = 9.80, p = .002) and trial (χ2 = 5.37, p = .020) for gait velocity during the MOVING trials, but no significant interaction effect (χ2 = 0.46, p = .496). Gait speed was significantly greater for the Control group throughout (i.e. patients walk slower), and gait speed also significantly increased from MOVING-1 to MOVING-15, irrespective of the group. This indicates that both Control and CBL group were able to adapt and increase their gait speed during subsequent MOVING trials. These results remained when controlling for treadmill speed (see Supplementary Materials).
Early-to-late moving ‘adaptation’ trials – EMGEMG data revealed evidence of across-trial neuromuscular adaptation for both groups. For contact leg MG, there was a significant main effect of trial during MOVING trials (χ2 = 16.29, p < .001); with reduced EMG activity during MOVING-15 compared to MOVING-1. There was no significant effect of group (χ2 = 0.36, p = .551), nor a significant interaction (χ2 = 1.09, p = .297); indicating that EMG activity in the contact leg MG decreased across MOVING trials irrespective of group. For contact leg TA, whilst there was no significant main effect of group (χ2 = 2.30, p = .130), there was a significant main effect of trial (χ2 = 7.54, p = .006) and a significant interaction between the two (χ2 = 4.36, p = .037). Post-hoc tests revealed a non-significant decrease in contact TA (the more strongly activated muscle during MOVING trials) from MOVING-1 to MOVING-15 for Control group (p = .078), but no change for the CBL group (p = 1.00) – indicating reduced adaptation. These results remained when controlling for treadmill speed (see Supplementary Materials).
After ‘de-adaptation’ trials – kinematic outcomesAs illustrated in Fig. 2, there was a general pattern of consistent locomotor after-effects in both kinematic variables for the control participants during the first AFTER trial (mean increase of 0.1 m/s for gait approach velocity and 16.36 cm for trunk sway with respect to baseline, respectively). In comparison, CBL patients tended to only exhibit after-effects for trunk sway (mean increase of 7.38 cm) – a reactive response (learned during MOVING trials to maximise postural stability) that is subsequently triggered in a feedforward ‘pre-emptive’ manner (Tang et al. 2013). In contrast, they exhibited limited after-effects for gait approach velocity (mean increase of 0.03 m/s), which reflects a true feedforward behaviour.
With respect to gait approach velocity during the first AFTER trial, there was a main effect of both group (χ2 = 5.16, p = .023) and trial (χ2 = 15.02, p < .001), and a significant interaction (χ2 = 3.88, p = .049). Bonferonni corrected post-hocs revealed a significant after-effect (i.e., significant increase in velocity in AFTER-1 compared to BEFORE) for the Control group (p < .001), but not the CBL group (p = .943). Whilst there was no main effect of group with respect to trunk sway (χ2 = 1.46, p = .227), there was a significant main effect of trial (χ2 = 21.99, p < .001). The interaction effect was not significant (χ2 = 3.15, p = .076), indicating that trunk sway was significantly greater during AFTER-1 compared to BEFORE trials for both groups. These results remained when controlling for treadmill speed (see Supplementary Materials).
After ‘de-adaptation’ trial – EMGFigure 4 shows the grand averaged trunk displacement and EMG in both CBL and Control group. Mean BEFORE (grey shaded area/line) and first AFTER (solid line) are shown for both groups. The EMG shown up to heel contact with the treadmill (-3–0 s) corresponds to gait initiation and 1.5 gait cycles (i.e., 3 steps with the 3rd resulting in resting stance on the treadmill).
The general pattern for neuromuscular control outcomes revealed consistent after-effects for ‘braking’ MG activity for the Control group; and a general absence of any significant neuromuscular after-effects for the CBL group. At the point of foot-contact onto the treadmill, the Control group display a clear increase in contact MG activity in first AFTER compared to baseline EMG (Fig. 4A). This burst constitutes increased gait termination (‘braking’) activity as part of the locomotor after-effect that is triggered in an anticipatory manner prior to foot-contact (Reynolds and Bronstein 2003; Bunday and Bronstein 2008; Bronstein et al. 2009). This MG burst is significantly reduced (oblique arrow) and delayed (vertical arrow) in the patients (Fig. 4B; compare with control data in Fig. 4A). Indeed, with respect to contact leg ‘braking’ MG activity during the first AFTER trial; whilst there was no significant main effect of group (χ2 = 1.70, p = .192), there was both a significant effect of trial (χ2 = 32.06, p < .001) and also a significant interaction effect (χ2 = 9.16, p = .002). Bonferonni corrected post-hocs revealed a significant after-effect (i.e., significant increase in contact leg MG activity 500 ms after foot-contact during AFTER-1 compared to BEFORE) for the Control group (p < .001), but not the CBL group (p = .190). For contact leg TA, there was neither a significant main effect of group (χ2 = 0.98, p = .323) nor trial (χ2 = 3.22, p = .073), nor a significant interaction between the two (χ2 = 0.40, p = .529). Combined, these results reveal a general absence of after-effects for the CBL group, with respect to neuromuscular variables. These results remained when controlling for treadmill speed (see Supplementary Materials).
Comments (0)