
Remember me
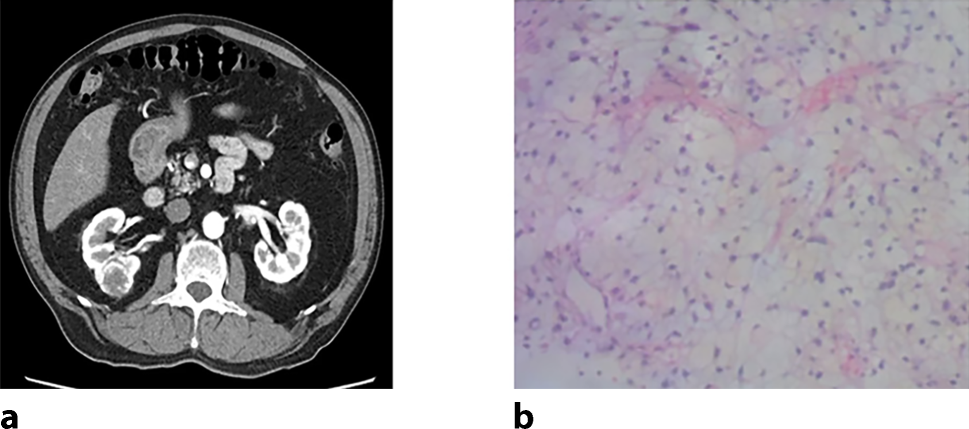
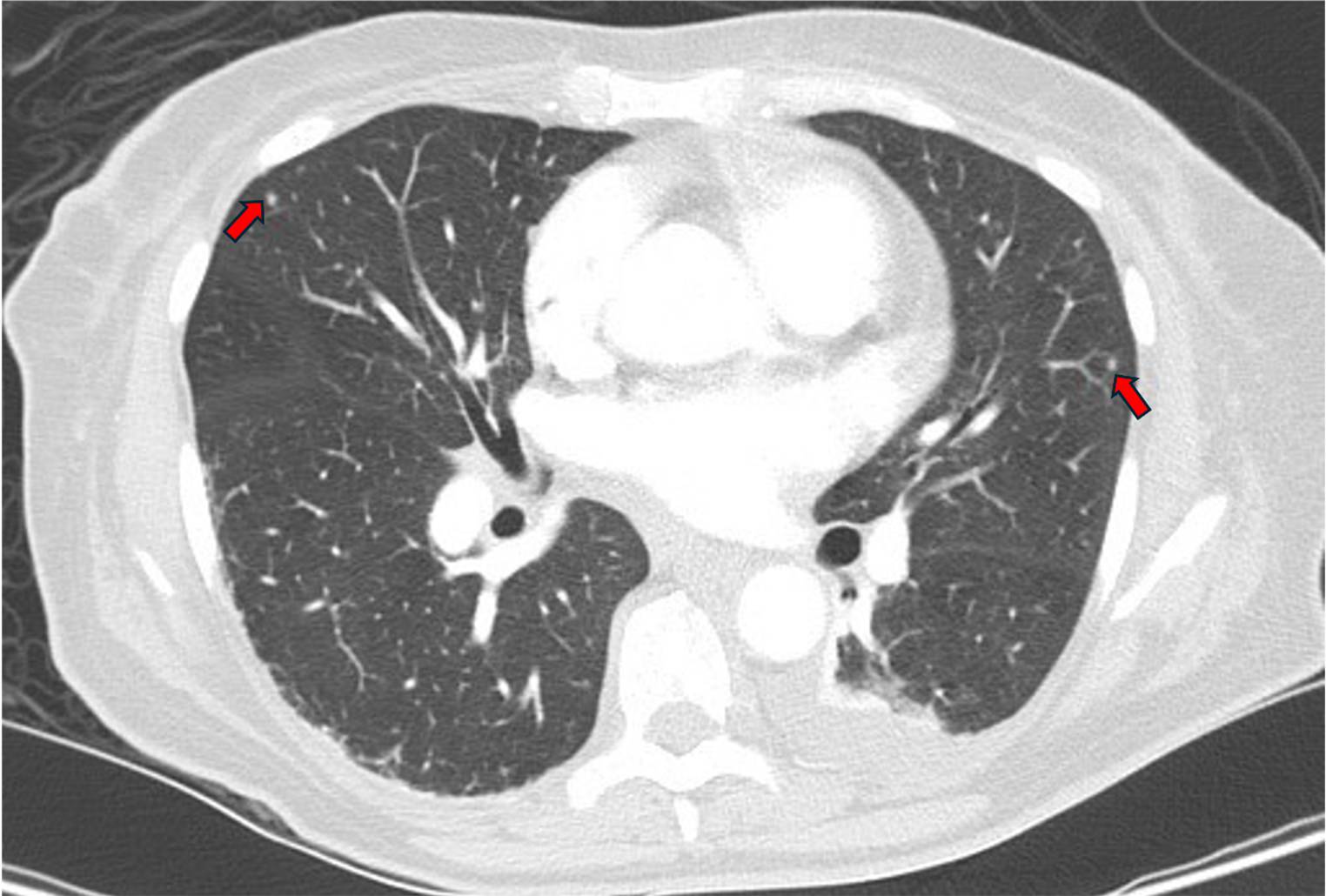
We present the case of a 59-year-old female patient, who presented to the emergency room with fatigue, dyspnea, and fever. Laboratory blood chemistry tests revealed: hemoglobin, 8.5 g/dL; leukocytes, 2.9 G/L; platelets, 84 G/L; C‑reactive protein (CRP), 23 mg/dL; interleukin, 6272 pg/mL; procalcitonin, 2.5 ng/mL; lactate dehydrogenase (LDH), 350 U/L; and an absolute neutrophil count of 0.3 G/L. A computed tomography (CT) scan showed multiple subpleural ventrally arranged, cavernous, cystic, partly disintegrating infiltrates in the upper and middle right lung lobe; morphologically similar lesions on the liver, as well as peripancreatic lesions and in the mesentery. The differential diagnosis corresponded to tuberculosis (Fig. 1).
Fig. 1
Thoracic/abdominal computed tomography scan showing multiple pulmonary and hepatic cavernous, cystic, partly disintegrating lesions
A bone marrow biopsy revealed the diagnosis of acute monocytic leukemia. Bone marrow aspirate showed a pronounced proliferation of partly myeloid and partly monocytic blast cells (85%). Trephine biopsy showed a hypercellular bone marrow with a dense infiltration by medium-sized to large, slightly pleomorphic blastic cells. The blastic infiltrate percentage was 60%. Immunomorphologically, these blasts were CD117+, CD13+, CD33+ and predominantly MPO+. No reactivity was observed with antibodies against CD34, TCD, cd19, PAX‑5, CD79a, CD10, CD3, CD71, CD61, and tryptase. Nucleophosmin showed an exclusively nuclear staining pattern without mutation (NPMC−). The bone marrow aspirate was cell-rich with predominantly medium-sized to large blastic cells with round-oval nuclei with one to two nucleoli. The cytoplasms were narrow to moderately broad, basophilic, partially granulated. There was no proliferation of ring sideroblasts, and there were no cytogenetic abnormalities. Molecular genetics revealed an IDH1 mutation, a DNMT3 mutation, and a KMT2A mutation.
The patient was transferred to undergo bronchoscopy with bronchoalveolar washing. Bacterial culture and Ziehl–Neelsen staining revealed the presence of Mycobacterium tuberculosis (MTB). The susceptibility test with genotypic resistance testing showed no abnormalities, so that therapy with ethambutol, pyrazinamide, isoniazid, and rifampicin was decided. The patient, however, suddenly presented with severe abdominal pain and de novo hematochezia. An urgent colonoscopy revealed a covered perforation, which was treated by clipping. Although the patient was originally classified as a candidate for intensive treatment, due to her young age and few comorbidities, it was decided against intensive high-dose therapy in view of the recent perforation and the infectious situation. Therefore, a therapy with VenAza was chosen. During application of venetoclax, CYP3A4 interactions must be considered, which in her case applied to the simultaneous application of rifampicin [3].
Recent data from patients with MDS have shown that a 14-day treatment regimen with VenAza achieved good results with complete remissions and less therapy-associated neutropenia and toxicities [5]. This 14-day regimen has also repeatedly appeared in smaller AML studies with good results [6]. A 14-day regimen was therefore chosen for our patient: The first 14 days consisted of 7 days subcutaneous administration (s.c.) of azacitidine with 14 days of per os (p.o.) venetoclax (with ramping up to 400 mg) followed by the start of the antituberculosis therapy and a break in hematological therapy for a further 14 days. Treatment was then restarted with 5 days of s.c. azacitidine (dose reduced) and 14 days of venetoclax (dose reduced to 200 mg) followed by a 14-day break (see below). Sulfametrole/trimethoprim was prescribed as prophylaxis against Pneumocystis jirovecii (Fig. 2).
Fig. 2
The 14-day therapy regimen to reduce hepato-toxicity and myelosuppression
In the first 14 days of hematological therapy, all cell lines started to decrease, as expected, and the increased continuously until day 28. Overall, four red blood cell transfusions and no platelet transfusions were necessary in the first 28 days of treatment. The absolute neutrophil count gradually increased from 0.3 G/L on day 1 to 1.26 G/L on day 28, hence overcoming the initial disease-associated neutropenia. The patient was released from inpatient care after 30 days or when neutropenia receded. All further treatment cycles were administered on an outpatient basis. There were no periods of severe neutropenia in later treatment cycles, nor were further blood transfusions necessary, which emphasizes the low hematotoxicity of the regimen applied in this case (Fig. 3).
Fig. 3
Treatment-induced hematotoxicity in the first 28 days of therapy. Separate units are given for each blood component
In later bone marrow biopsies (1 and 6 months after therapy) the AML was no longer detectable in terms of a complete remission. In a CT thorax/abdomen examination after 3 and 6 months of antitubercular therapy, the tuberculosis also showed adequate signs of regression. Currently, our patient is being evaluated for stem cell transplantation.
Comments (0)