
Remember me

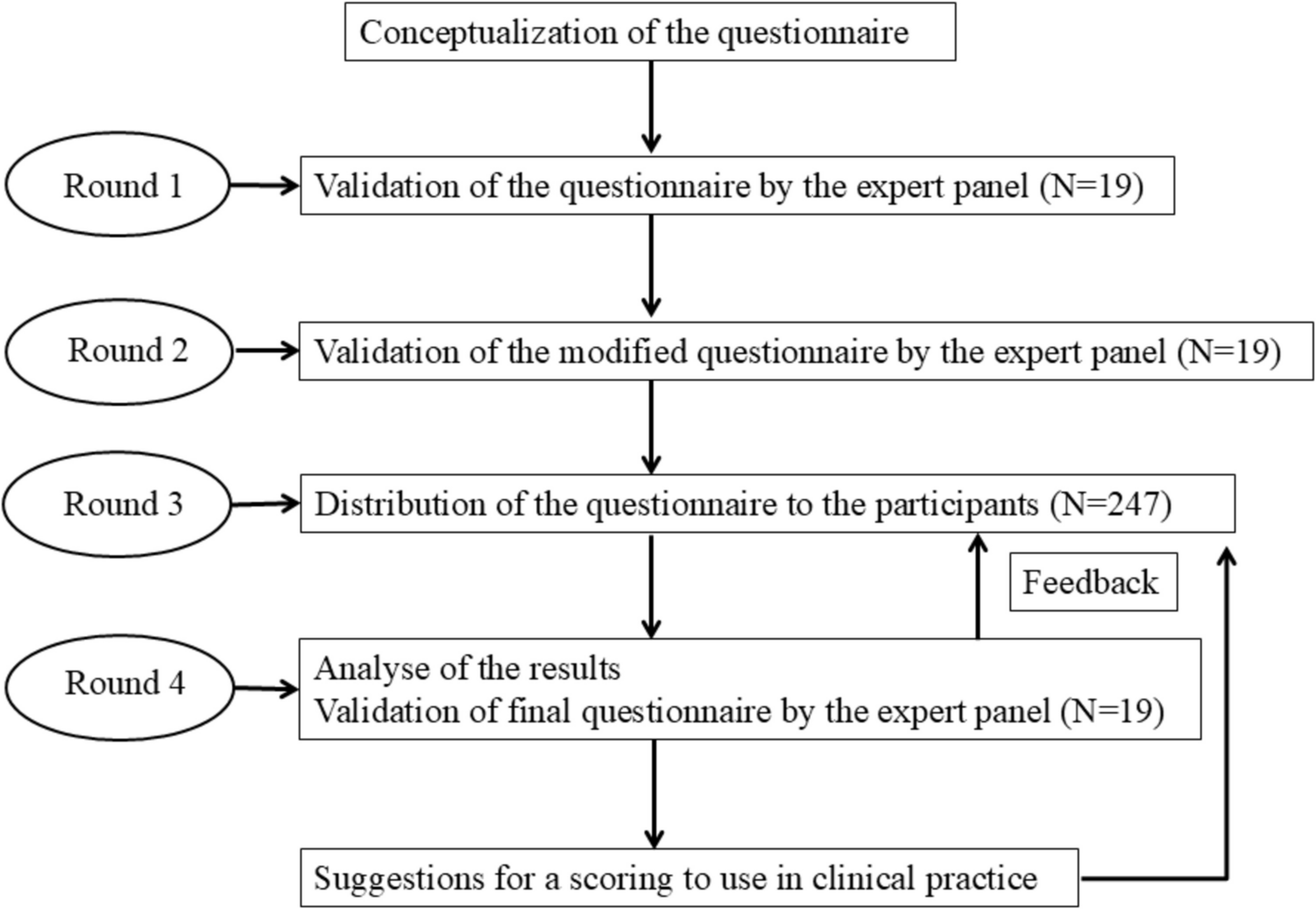
As in other autoinflammatory syndromes, establishing the diagnosis of AiKD can be challenging. In most cases of inflammatory keratinization diseases, there is no monogenic mutation resulting in the hyperactivation of innate immunity. At the same time, the clinical features may imitate conventional inflammatory keratinization diseases. Therefore, we propose a clinical approach to the diagnosis and management of AiKDs illustrated in Fig. 2.
Fig. 2
Suggested diagnostic approach to the autoinflammatory keratinization diseases. This figure shows the most significant disorders. ACH—acrodermatitis continua of Hallopeau; AGEP—acute generalized exanthematous pustulosis; DIRA—deficiency of the interleukin-1-receptor antagonist; GPP—generalized pustular psoriasis; NADED—NLRP1-associated autoinflammatory disease with epithelial dyskeratosis; PRP—pityriasis rubra pilaris
First, autoinflammation should be suspected in inflammatory keratinization diseases whenever there is a history of early onset and familial incidence [48]. This should also be considered in the setting of concomitant systemic syndromes such as recurrent fever, arthritis, and cholangitis. However, by definition of AiKDs and in contrast to other autoinflammatory diseases, the inflammation is primarily present in the epidermis and upper dermis [5]. Hence, extracutaneous features involving the nervous system, bones, and gastrointestinal tract are atypical findings. This also explains the difference in the morphology of skin lesions between AiKDs and other autoinflammatory syndromes. Most autoinflammatory diseases characterized by deep cutaneous inflammation can be classified into clinico-pathological patterns such as urticarial dermatosis, neutrophilic dermatosis, or granulomatosis [99]. In contrast, AiKDs present with hyperkeratotic and/or pustular lesions reflecting the superficial inflammation altering the keratinization process.
Once AiKD is considered in the differential diagnoses, the history and physical examination should be detailed to determine specific features of the analyzed case. The morphology, location, and triggers of cutaneous lesions should be carefully studied, along with the possible pattern of inheritance. In most cases, a skin biopsy is recommended to confirm the diagnosis of a suspected inflammatory disorder of keratinization. These established patterns of clinical and histological symptoms should be complemented by genetic studies.
Identification of causative mutations can tailor the treatment regimen to the particular case. In contrast to classic systemic treatments such as methotrexate and oral retinoids, most AiKDs will respond to pharmaceuticals targeting the IL-1, IL-12/IL-23, or IL-17 pathways [48, 50]. For example, favorable effects of treatment with IL-1 receptor antagonist anakinra were reported in a patient with generalized pustular psoriasis associated with IL36RN mutation [100]. The IL-1R blockade is not commonly used in classic forms of inflammatory keratinization diseases. Hence, effort should be made to establish the possibility of expanding the available therapeutic options and improve the management of patients with AiKDs.
Below we provide a brief, clinically oriented description of the most significant AiKDs (Tables 1 and 2).
Table 1 Autoinflammatory keratinization diseases described in the present articleTable 2 Summary of diseases associated with NLRP-1 hyperactivation. Common pathogenesis and clinical similarities justify considering these entities jointly within the spectrum of NLRP1-associated autoinflammatory disease with epithelial dyskeratosis (NADED)Generalized and Localized Variants of Pustular PsoriasisClinical FeaturesPsoriasis is a frequent inflammatory keratinization disease characterized by a chronic course and a significant negative effect on the quality of life [47]. It is estimated that the prevalence of psoriasis amounts to 3% of the general population [47, 101]. Psoriasis can be divided into two primary subtypes: the more frequent nonpustular type (approx. 90% of cases) presenting with papulosquamous lesions and the less prevalent pustular type. The spectrum of pustular psoriasis involves generalized forms (the acute von Zumbusch variant (Fig. 3), impetigo herpetiformis, annular pustular psoriasis, and juvenile pustular psoriasis) and localized forms (palmoplantar pustulosis (Fig. 4) and acrodermatitis continua of Hallopeau (Fig. 5). Most pustular psoriasis subtypes can present as AiKD [5].
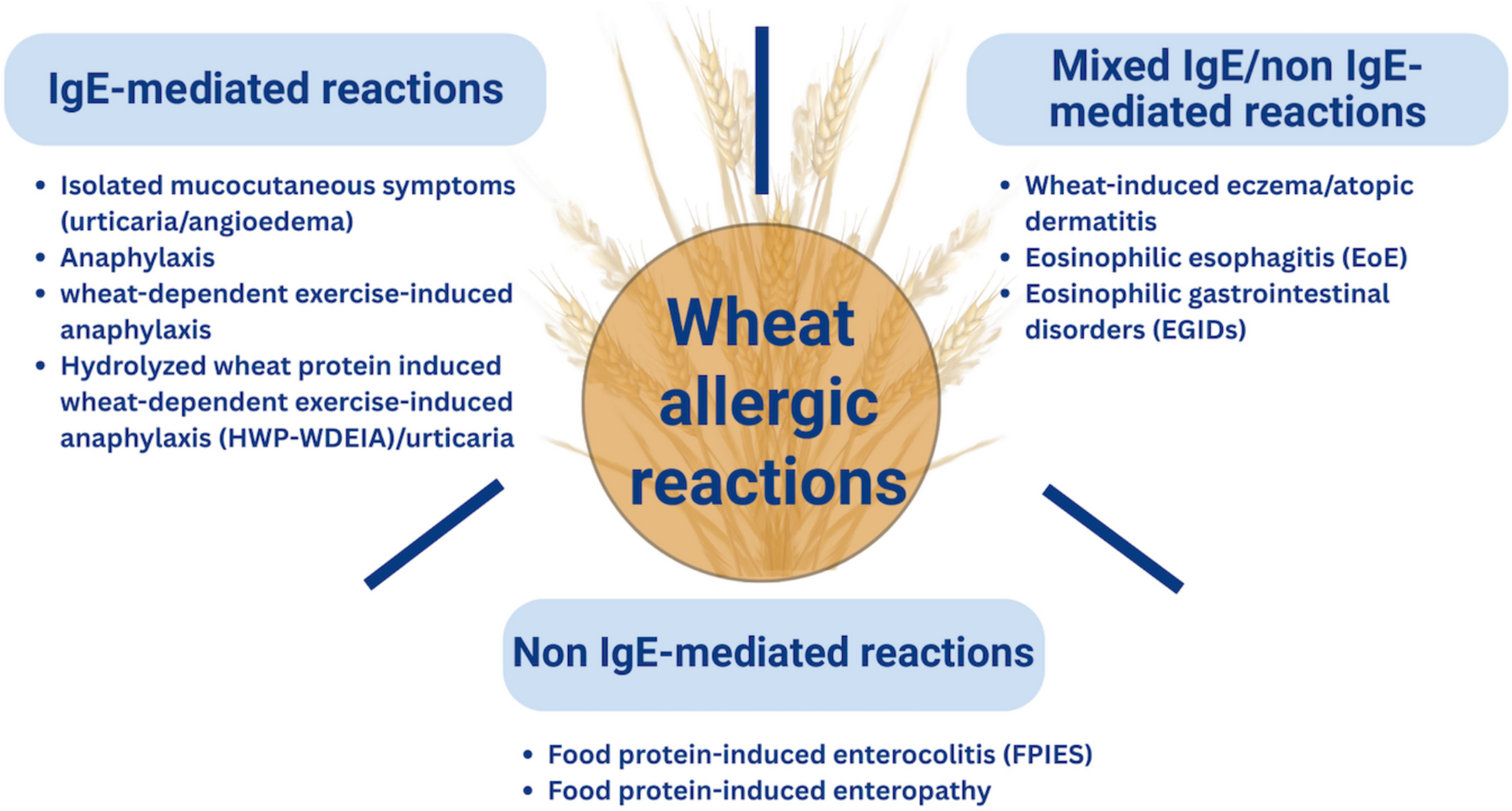
Fig. 3
Sterile pustules in generalized pustular psoriasis. a, b Histology shows Munro microabscesses and spongiform pustules of Kogoj c occasionally accompanied by typical features of psoriasis vulgaris (acanthosis, confluent parakeratosis, elongation of rete ridges, and dilation of papillary blood vessels)
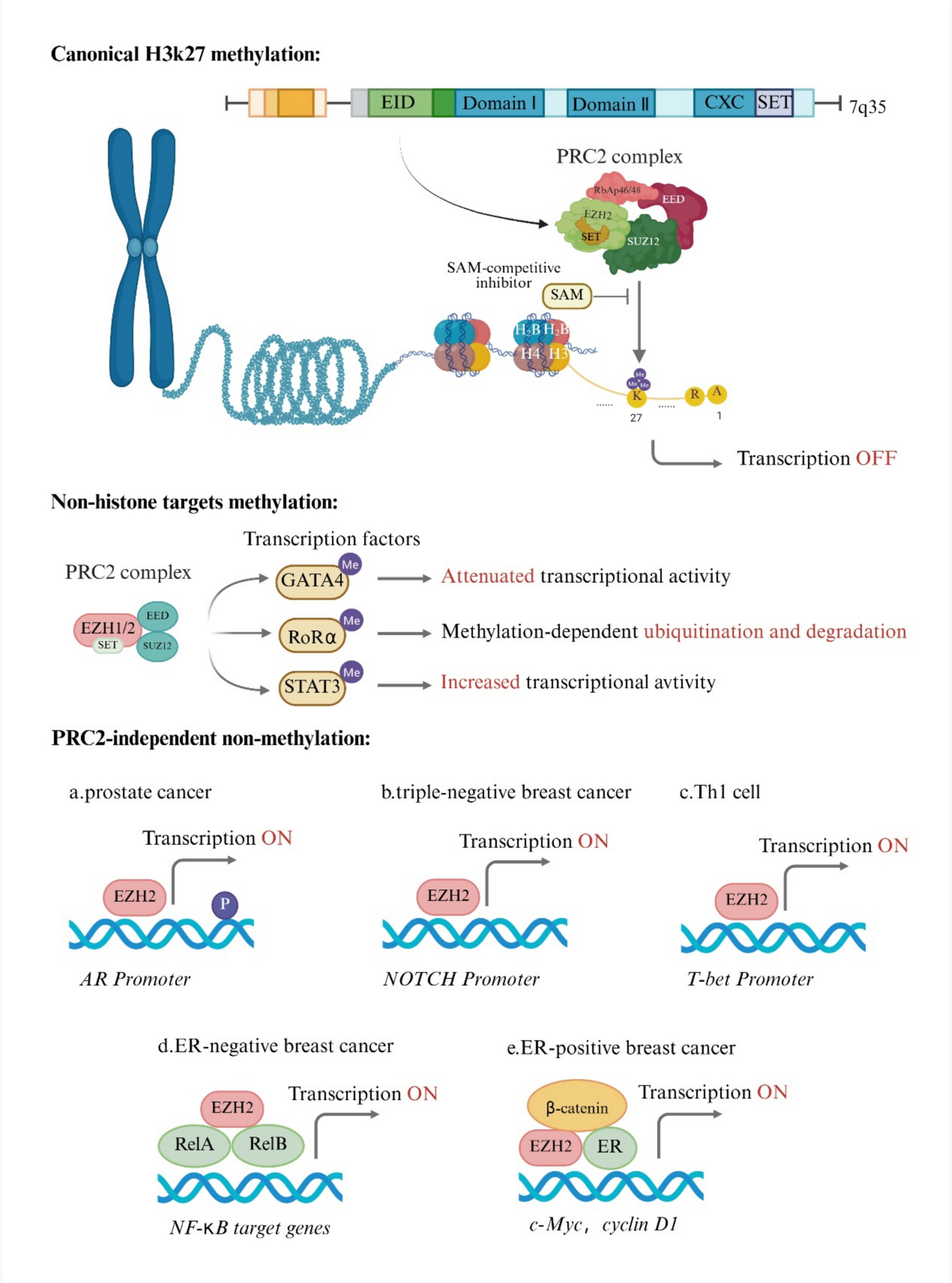
Fig. 4
Palmoplantar pustulosis. Sterile pustules limited to palms (a) and/or soles (b) which may rupture and produce fissures and erosions, thereby impairing fine motor skills and walking
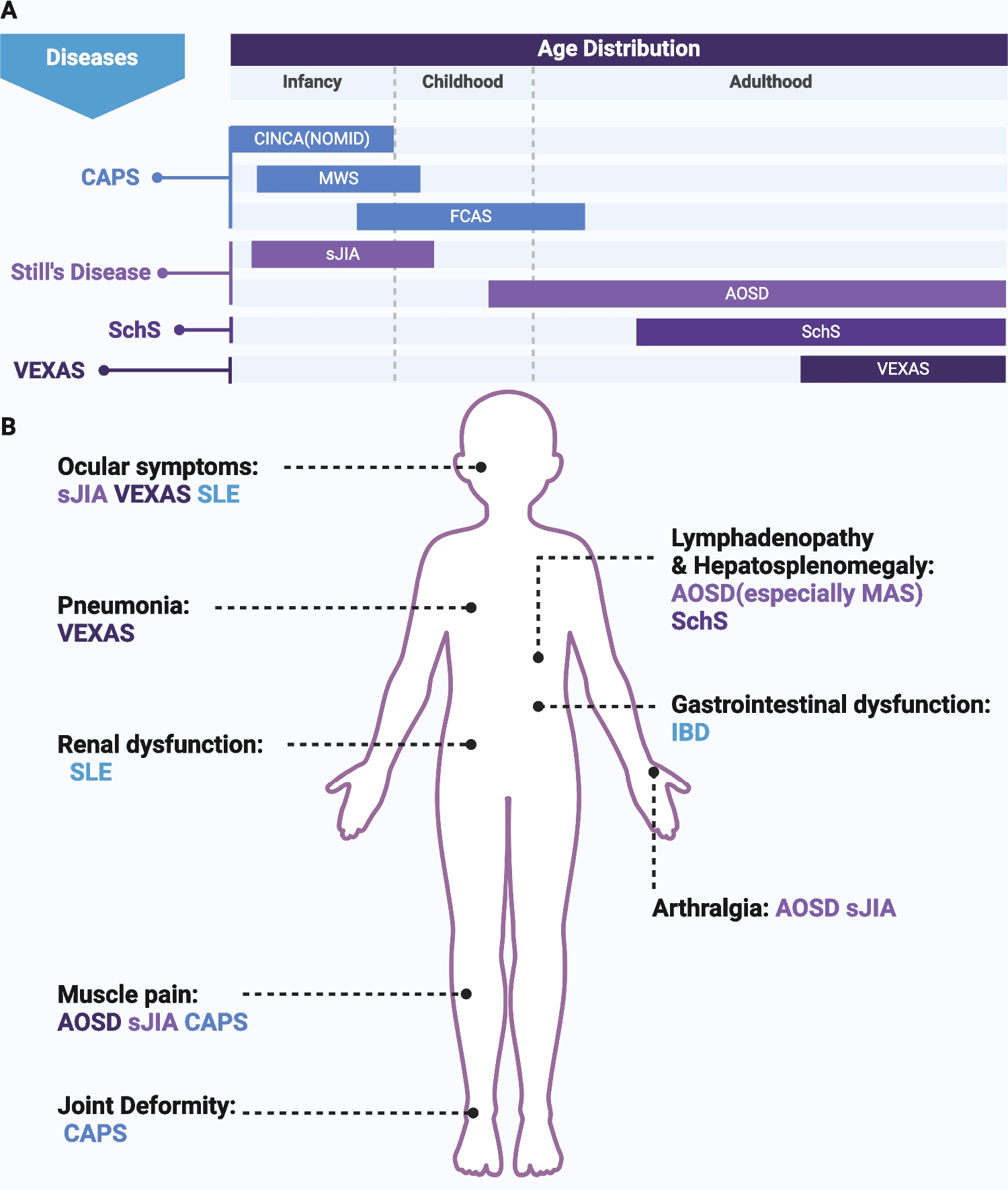
Fig. 5
Acrodermatitis continua of Hallopeau. Pustular lesions occupying the distal phalanges of the hands (a) and/or the feet (b). There is a prominent involvement of the nail apparatus resulting in onychodystrophy
The diagnosis of psoriasis is clinical [101]. In doubtful cases, histopathological examination can be performed to confirm the clinical suspicion. According to the name, the pustular forms of psoriasis are characterized by the formation of sterile pustules. The von Zumbusch variant is typically accompanied by systemic symptoms (fever, malaise, uveitis, osteoarthritis, cholangitis) and elevated biomarkers of systemic inflammation. It is also a potentially lethal condition, threatening with quick progression of cutaneous lesions into erythroderma. The confluence of pustular lesions may result in epidermal detachment causing electrolyte abnormalities, increased risk of infection, and other serious complications [102]. The localized variants are rarely associated with systemic manifestations but tend to present a protracted course [101].
Impetigo herpetiformis is considered to be a form of GPP developing during pregnancy [65, 102]. In most cases, the lesions begin during the third trimester. Similarly to GPP, impetigo herpetiformis is a potentially life-threatening condition. Apart from the risk to the mother, it is associated with possible fetal distress resulting from placental insufficiency [103]. Hence, the prompt diagnosis and treatment are essential to prevent severe maternal and fetal complications.
Palmoplantar pustulosis constitutes a localized variant of psoriasis affecting the palms and/or the soles [104]. The clinical picture involves persistent eruptions of sterile pustules superimposed on an erythematous and desquamative background. The prevalence of PPP is estimated at up to 0.05% of the general population and is slightly higher in women [105]. The lesions may coexist with typical lesions of psoriasis vulgaris in other locations and nail changes (onycholysis, pitting, nail destruction) [106].
Acrodermatitis continua of Hallopeau (ACH) is a very rare form of localized pustular psoriasis distinguished by the presence of lesions on the distal digits of the hands and/or the feet and involvement of the nail apparatus resulting in onychodystrophy (Fig. 5) [102, 107]. It may also be associated with osteitis of the distal phalanges. ACH has been reported in patients suffering from occasional GPP flare-ups, which supports the view that those two diseases belong to the common spectrum [102].
Acute generalized exanthematous pustulosis (AGEP) is the main differential diagnosis of GPP [108]. AGEP is a widespread pustular drug reaction driven by drug-specific CD4 and CD8 lymphocytes [109]. The skin lesions have an almost identical morphology and progression as in GPP. Small pustules superimposed on an erythematous base are initially seen in the skin folds and may quickly spread to other skin areas. AGEP can be associated with systemic symptoms (fever, malaise) and laboratory abnormalities including elevated C-reactive protein, hypocalcemia, hypoalbuminemia, and leukocytosis (with concomitant eosinophilia in approximately 30% of cases) [109]. The offending drugs are usually administered 48 h prior to the onset of symptoms. Identification of the common genetic background of GPP and AGEP raised controversies about whether AGEP is not indeed a form of drug-induced GPP [66].
Another differential diagnosis of GPP is the subcorneal pustular dermatosis (SPD), also known as the Sneddon-Wilkinson syndrome [110]. SPD is characterized by the presence of flaccid hypopyon pustules with annular distribution. Similarly to GPP and AGEP, the lesions tend to arise in the intertriginous areas and may progress to involve the trunk and extremities. SPD tends to run a relatively benign and self-limiting course. Systemic symptoms are infrequent. It usually begins in adulthood, but several cases of childhood-onset cases have also been reported [111, 112]. Clinically, SPD may imitate IgA pemphigus, but it is differentiated by negative direct and indirect immunofluorescence studies [113]. It was shown that SPD may coexist with a number of other disorders, involving connective tissue diseases (rheumatoid arthritis, systemic lupus erythematosus) and hematologic disorders (IgA monoclonal gammopathy, multiple myeloma) [110]. To date, the pathogenesis of SPD is unknown.
HistologyThe histological features of pustular psoriasis involve the presence of Munro microabscesses and spongiform pustules of Kogoj (Fig. 3c) [101]. The lesions can coexist with features of psoriasis vulgaris (acanthosis, confluent parakeratosis, elongation of rete ridges, and dilation of papillary blood vessels) or be present in the setting of otherwise unchanged epidermis.
Genetic BackgroundAs discussed previously, autoinflammatory variants of generalized and localized pustular psoriasis can result from several pathogenetic pathways, i.e., IL36RN loss-of-function (OMIM no. 605507), CARD14-activating (OMIM no. 602723), and AP1S3 loss-of-function (OMIM no. 616106) pathogenic variants. The IL-36Ra deficiency results from biallelic loss of function variants in IL36RN [61]. The patients with IL-36Ra deficiency present a more severe phenotype and have an earlier onset of GPP compared to those with CARD14 variants (Fig. 6) [108]. CARD14-activating variants stimulate the transcription of pro-inflammatory factors in the NF-κB-dependent pathway. This can lead to the onset of pustular psoriasis in patients with concurrent psoriasis vulgaris. Other clinical features involve early age of onset; prominent involvement of the cheeks, chin, and ears; family history of psoriasis or PRP; and minimal improvement using classic therapies of psoriasis [50]. Lastly, AP1S3 variants seem most closely associated with palmoplantar pustulosis [84].
Fig. 6
Generalized pustular lesions in a child with confirmed deficiency of the IL-36 receptor antagonist (DITRA)
Recently, the role of IL36RN variants was shown to underlie most cases of impetigo herpetiformis particularly in the East Asian populations [114]. This supports the hypothesis on a common pathogenetic background of impetigo herpetiformis and GPP. IL36RN variants were also detected in patients with AGEP, substantiating the already difficult differentiation with GPP [118].
TreatmentGPP is an infrequent entity. Therefore, large randomized controlled trials assessing the efficacy of different treatment modalities are lacking [101, 119]. There is even less data regarding autoinflammatory cases of GPP caused by IL36RN and CARD14 mutations.
Generally, it is recommended to treat acute severe GPP with cyclosporine or infliximab [120]. In more chronic cases, systemic retinoids (acitretin) and methotrexate can be considered. However, patients with autoinflammatory forms of pustular psoriasis may be recalcitrant to standard treatment modalities [50]. Furthermore, TNF inhibition with infliximab was shown to induce paradoxical palmoplantar pustulosis in a subset of patients with psoriasis vulgaris [121]. Therefore, off-label use of other biologics should be considered.
Based on experimental data, patients with IL36RN variants could benefit from the blockade of IL-36R signaling. This assumption was recently tested in a proof-of-concept study of spesolimab, an anti-IL-36R antibody which showed high efficacy after single-dose administration [122]. Spesolimab has been recently approved by the US Food and Drug Administration and the European Medicines Agency for the treatment of GPP flares in adults [123, 124]. Imsidolimab is another biologic targeting IL-36R under investigation in GPP [125]. In a clinical trial of palmoplantar pustulosis, imsidolimab failed to meet the primary outcomes.
Considering that both IL-36Ra deficiency and CARD14 hyperactivation induce inflammatory cascade involving Th1 and Th17 molecules, inhibition of those signals could be associated with favorable clinical outcomes. Indeed, patients with those variants were shown to improve after administration of biologics targeting IL-12/IL-23 (ustekinumab), IL-17 (secukinumab), and TNF (etanercept, infliximab, adalimumab) [119].
With respect to impetigo herpetiformis, most recent reports of cases refractory to conventional treatment (i.e., topical steroids, cyclosporine, and phototherapy) showed a favorable response to secukinumab [115,116,117]. TNF inhibitors, particularly certolizumab for its safety in pregnancy, also seem to be a potentially beneficial treatment strategy [102].
It is important to mention that systemic steroids can induce GPP exacerbations, especially if rapidly tapered. However, some data support their cautious use as adjuvant treatment in cases associated with systemic symptoms or arthritis. For example, the Japanese guidelines for the management of GPP advocate oral steroids particularly in pregnancy, during which many drugs are contraindicated because of their teratogenic potential [126].
Deficiency of Interleukin-1 Receptor Antagonist (DIRA)Clinical FeaturesDIRA is a rare, severe disorder associated with uncontrolled signaling via the IL-1R due to the deficiency of its negative regulator, the IL-1Ra [67, 68, 127].
DIRA usually starts in the neonatal period and has a dramatic course resulting in a mortality of up to 30% in untreated infants [127]. The clinical features involve a pustular rash imitating GPP, aseptic multifocal osteomyelitis, thrombotic events, and central nervous system vasculitis [67, 127]. In longstanding, non-treated disease hyperostosis may be seen. Additional disease stigmata involve elevation in acute phase proteins and pathergy.
HistologyThe findings on the cutaneous biopsy are identical to GPP. However, the inflammatory infiltrates may contain even larger amounts of neutrophils [67, 128].
Genetic BackgroundDIRA (OMIM no. 612852) is caused by biallelic loss-of-function pathogenic variants in IL1RN [127]. To date, 10 different variants have been reported. In the largest case series described to date, Aksentijevich et al. [129] presented 1 patient from Newfoundland who was homozygous for a deletion of 2 bp (c.156_157delCA) causing a frameshift mutation, three patients from families of Dutch ancestry homozygous for a nonsense mutation affecting the amino acid at position 77 (nucleotide mutation, c.229G → T; resultant amino acid mutation, E77X), two patients from a consanguineous Lebanese family homozygous for a nonsense mutation (c.160C → T), and one patient from Puerto Rico homozygous for a deletion of approximately 175 kb on chromosome 2q affecting six interleukin-1-related genes. Reportedly, the symptoms varied in terms of pustular rash severity and internal organ involvement even in patients with the same genotypes, which underscores the probable effect of environmental factors on the genotype-phenotype correlation.
TreatmentThe successful treatment of DIRA can be achieved by blocking the IL-1 inflammatory pathway. Among the possible treatment options are anakinra (recombinant IL-1Ra), canakinumab (an anti-IL-1β monoclonal antibody), and rilonacept (a soluble decoy IL-1R) [68, 130,131,132]. Treatment with those agents was shown to be effective in improving the balance between pro- and anti-inflammatory signaling via IL-1R and constricting the autoinflammatory cascade in DIRA.
Nucleotide-Binding Oligomerization Domain-Like Receptor Containing a PYRIN Domain 1 (NLRP1)-Associated Autoinflammatory Disease With Epithelial Dyskeratosis (NADED)As discussed above, NLRP1 inflammasomes are key structures orchestrating the immune response in the epithelia [133]. Akiyama et al. distinguished familial keratosis lichenoides chronica (KLC) as the prototypic AiKD associated with activating mutations in NLRP1 [5]. However, more cases of NLRP1 hyperactivation characterized primarily by skin and mucosal inflammation and variable systemic involvement have been described (Table 2). Similarities in terms of clinical presentation, histology, and pathogenesis justify expanding this group and distinguishing it as a separate endotype of AiKDs. Therefore, we propose a joint term of NLRP1-associated autoinflammatory disease with epithelial dyskeratosis (NADED) which encompasses the whole spectrum of AiKDs secondary to NLRP1 hyperactivation.
Clinical FeaturesThe onset of NADED is usually during infancy or early childhood [18, 74,75,76,
Comments (0)