
Remember me



This retrospective cohort study was reported according to the STROBE guidelines [8]. It received approval from the Ethics Committee of the Affiliated People's Hospital of Ningbo University (2022 Research No. 068), and a written informed consent was obtained from the participants for the publication of the results and any accompanying tables/figures.
PatientsWe collected data from the Department of Thyroid Breast Surgery, People’s Hospital of Ningbo University, Ningbo, China, between January 2022 and November 2022. The data was obtained from patients diagnosed with PTC who underwent total or near-total thyroidectomy with bilateral lymph node dissection in the central region.
Surgical methodsOur surgical approach involved the use of dyes as a routine procedure. Initially, we experimented with nanocarbon staining alone, which yielded fair staining results. Subsequently, we tried ICG dye alone and achieved favorable results. Based on these findings, we used a combination of two dyes in an attempt to generate synergistic effects. The surgical procedures and data collection were performed by the same surgical team. All patients underwent total or near-total thyroidectomy with bilateral central zone lymph node dissection.
In the combined group, after the thyroid tissue was exposed, an injection of CNP dye was administered into the thyroid gland (Chongqing Lemay Pharmaceutical Co., Chongqing, China). To minimize the risk of accidental CNP dye spillage and contamination of adjacent tissue, the injection site was compressed and coagulated using an electric knife (CNP imaging method). ICG (Chinese medicine approval number H20055881, Dandong Yichuang Pharmaceutical Co., Ltd., Liaoning, China), dissolved in sterile water, was administered intravenously. The ptoMedic NIR fluorescence endoscopy system was used to observe parathyroid fluorescence. A thorough visual examination was then conducted on the dorsal thyroid gland to identify any highly suspected parathyroid tissues. Following thyroidectomy and bilateral lymph node dissection in the central region, the same dose of ICG was reinjected. The glands identified preoperatively were re-evaluated using the ICG imaging method. In the CNP group, only the CNP imaging method was used, while in the ICG group, only the ICG imaging method was employed.
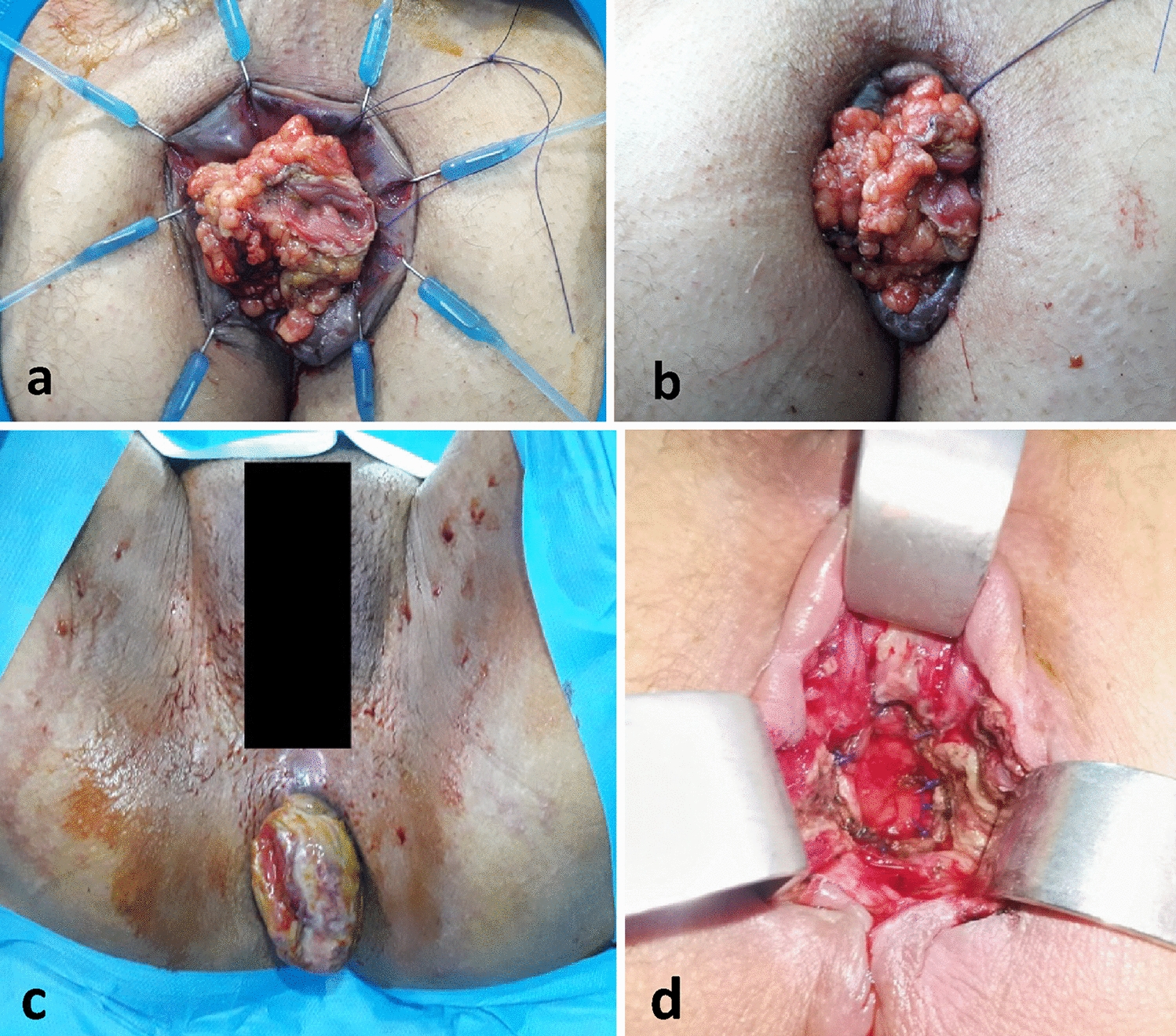
All three groups of patients had highly suspicious parathyroid tissue detected during surgery. For these tissues, those evaluated as having good activity are selected to be retained in situ. We perform fine needle aspiration (Fig. 1). The syringe is combined with a disposable intravenous indwelling needle, and an appropriate amount of the extract in the needle cavity is dripped into the PTH test paper monitoring point. (Eshzhu Zhun 20152402195, Wuhan Baioda Biotechnology Co., Ltd., Wuhan, China), and then the observation time was about 10 min to evaluate the results (PTH test method, Fig. 2). For highly suspicious parathyroid tissue that was mistakenly resected or whose activity was poorly evaluated, we removed 1 mm3 tissue samples for frozen section examination. If the parathyroid tissue was identified as parathyroid, autologous transplantation into muscle was performed.
Fig. 1
Fine needle aspiration of the parathyroid gland
Fig. 2
PTH test results shown. Image A indicates that non-parathyroid (PTH test negative), and image B indicates that is parathyroid (PTH test positive)
During surgeries involving ICG, we routinely invited three experienced specialists from outside the team to provide intraoperative support. The fluorescence intensity of parathyroid tissue in both ICG-only and combined groups was assessed using the grading system proposed by Fortuny et al. [9]. An ICG score of 0 indicated no fluorescence was observed, while a score of 1 indicated fluorescence in both the parathyroid gland and its surrounding tissue. A score of 2 (Fig. 3) indicated a higher fluorescence intensity in the parathyroid gland compared to the surrounding tissue (fluorescence grading method) [10]. For cases with a fluorescence grading score of 0, autologous transplantation was performed. If the score was 1, the evaluation was repeated, and if the score remained 1 after re-evaluation, fine needle puncture is performed to observe the blood supply. In cases where parathyroid flow was abundant, the parathyroid glands were preserved in situ, while in cases with no blood flow, autograft transplantation was performed. If the score was 2, in situ preservation treatment was conducted.
Fig. 3
Visualization of a parathyroid gland with a score of 2(blue arrows)1
To further evaluate the predictive value of fluorescence intensity for postoperative hypoparathyroidism, fluorescence score data were collected from the ICG group and the combined group. Based on the fluorescence intensity results, patients were divided into three groups: group 0, group 1, and group 2. Grouping criteria were as follows: patients with the highest intraoperative parathyroid score of 0 were included in group 0, those with a score of 1 were included in group 1, and those with a score of 2 were included in group 2.
Data collectionWe collected retrospective data collection EMRs (inpatient and outpatient records). These data included information on patients' gender, age, tumor size, height, weight, length of hospital stay, intraoperative operative time, intraoperative bleeding, number of intraoperatively identified parathyroid glands, number of transplanted parathyroid glands, postoperative drainage, and postoperative blood calcium and PTH levels on the first day, the third day, and the first, third, and sixth month after operation.
Postoperative hypoparathyroidism and hypocalcemia were determined based on postoperative PTH levels and blood calcium levels. Temporary hypoparathyroidism was defined as PTH levels < 15 pg/ml within 1 day after surgery or the presence of symptoms such as numbness or tingling in fingertips or perioral, hand, foot, or facial muscles, convulsions or epileptiform generalized convulsions, or multiple episodes of blood calcium < 2.0 mmol/L and blood phosphorus > 2.0 mmol/L, with recovery within 3 months. Permanent hypoparathyroidism was defined as requiring more than 6 months for recovery [11].
Basis for groupingThe inclusion criteria were the same for all patients: (1) signed informed consent for surgery; (2) age between 18 and 79 years, without gender or race restrictions; (3) PTC confirmed by routine postoperative pathology; (4) lesions with a maximum diameter < 30 mm.
Exclusion criteria included: (1) abnormal preoperative parathyroid hormone (PTH) levels; (2) lesions invading the thyroid peritoneum or surrounding tissues, or retrosternal goiter; and (3) combined parathyroid gland disease.
Ultimately, the clinical data of 136 patients who met the requirements were screened. Among the patients who initially met the inclusion criteria, five patients were excluded due to incomplete postoperative PTH reviews following the standard follow-up schedule. Additionally, seven patients were excluded as a result of early or delayed follow-up. As a result, we obtained and analyzed case data from a total of 124 patients.
Patients were divided into three groups based on the dye used during surgery: CNP group (CNP dye only, n = 38), ICG group (ICG dye only, n = 42), and combined group (combined CNP and ICG double dye, n = 44).
Statistical analysisSPSS.25.0 statistical software was used for statistical analysis of all data, and the measurement data of each group were expressed as \((\overline \, + \,S)\). The continuous variable differences between groups were analyzed using one-way analysis of variance (ANOVA), and the pairwise comparisons between groups were analyzed using the Student–Newman–Keuls (SNK) method. The differences in categorical variables were analyzed using the chi-square test. Receiver operating characteristic (ROC) curves were also plotted. P < 0.05 was considered statistically significant.
Comments (0)